Potrebbero piacerti anche
- Full Download Bontragers Textbook of Radiographic Positioning and Related Anatomy 9th Edition Lampignano Test BankDocumento36 pagineFull Download Bontragers Textbook of Radiographic Positioning and Related Anatomy 9th Edition Lampignano Test Bankjohn5kwillis100% (22)
- Yochum and Rowe - Cap 2 PDFDocumento119 pagineYochum and Rowe - Cap 2 PDFRICARDO LOPEZ FLORESNessuna valutazione finora
- Case Study On "Unilever in Brazil-Marketing Strategies For Low Income Consumers "Documento15 pagineCase Study On "Unilever in Brazil-Marketing Strategies For Low Income Consumers "Deepak BajpaiNessuna valutazione finora
- Nursing Care Plan For AIDS HIVDocumento3 pagineNursing Care Plan For AIDS HIVFARAH MAE MEDINA100% (2)
- Guide For Sustainable Design of NEOM CityDocumento76 pagineGuide For Sustainable Design of NEOM Cityxiaowei tuNessuna valutazione finora
- Magnetic Resonance Imaging - 2005 - Tench - Measurement of Cervical Spinal Cord Cross Sectional Area by MRI Using EdgeDocumento7 pagineMagnetic Resonance Imaging - 2005 - Tench - Measurement of Cervical Spinal Cord Cross Sectional Area by MRI Using EdgeAbhilash VemulaNessuna valutazione finora
- Normal Thickness and Appearance of The Prevertebral Soft Tissues On Multidetector CTDocumento6 pagineNormal Thickness and Appearance of The Prevertebral Soft Tissues On Multidetector CTresta_pxdNessuna valutazione finora
- SCHIZAS Qualitative GradingDocumento6 pagineSCHIZAS Qualitative GradingDitaAnggaraKusumaNessuna valutazione finora
- Contouring Inguinal and Femoral Nodes How Much Margin Is Needed Around The Vessels?Documento5 pagineContouring Inguinal and Femoral Nodes How Much Margin Is Needed Around The Vessels?Rainey AhmadNessuna valutazione finora
- Definingnoptimal Calcar Screw Positioning in Proximal Humerus Fracture FixationDocumento7 pagineDefiningnoptimal Calcar Screw Positioning in Proximal Humerus Fracture FixationAJ CésarNessuna valutazione finora
- Use of Ultrasonography As A Diagnostic and Therapeutic ToolDocumento11 pagineUse of Ultrasonography As A Diagnostic and Therapeutic ToolVojtěch ŠmídNessuna valutazione finora
- Influence of Age and Sex On The Position of The Conus Medullaris and Tuffier's Line in AdultsDocumento5 pagineInfluence of Age and Sex On The Position of The Conus Medullaris and Tuffier's Line in AdultsregarskidNessuna valutazione finora
- Anterior Loop of The Mental NerveDocumento8 pagineAnterior Loop of The Mental NerveMahily Pérez OrtizNessuna valutazione finora
- Scientific Abstracts Friday, 14 June 2019 1015Documento1 paginaScientific Abstracts Friday, 14 June 2019 1015حسام الدين إسماعيلNessuna valutazione finora
- Comparison of Standard Radiography and Computed Tomography in 21 Dogs With Maxillary Masses 2Documento5 pagineComparison of Standard Radiography and Computed Tomography in 21 Dogs With Maxillary Masses 2Joffre VelasquezNessuna valutazione finora
- Rycan 2021210036Documento7 pagineRycan 2021210036Imagenologia Hospital de ClinicasNessuna valutazione finora
- Ajr 21 25606Documento11 pagineAjr 21 25606ecavalcantiNessuna valutazione finora
- (10920684 - Neurosurgical Focus) Radiological Evaluation of Cervical Spine Involvement in Rheumatoid ArthritisDocumento7 pagine(10920684 - Neurosurgical Focus) Radiological Evaluation of Cervical Spine Involvement in Rheumatoid ArthritisPriyank OzaNessuna valutazione finora
- Resnick 2018Documento29 pagineResnick 2018Manuel Saúl Vicente CoasacaNessuna valutazione finora
- Hiperplasia Condilar3Documento5 pagineHiperplasia Condilar3Alejandra Oliveros VargasNessuna valutazione finora
- Meazzini 2020Documento7 pagineMeazzini 2020Gabriel BravoNessuna valutazione finora
- Kinematic Evaluation of Cervical Sagittal Balance and Thoracic Inlet AlignmentDocumento13 pagineKinematic Evaluation of Cervical Sagittal Balance and Thoracic Inlet Alignmentdr.s.russo5172Nessuna valutazione finora
- Ojsadmin, 302Documento7 pagineOjsadmin, 302Abhilash VemulaNessuna valutazione finora
- Carotid Body Tumors: Objective Criteria To Predict The Shamblin Group On MR ImagingDocumento6 pagineCarotid Body Tumors: Objective Criteria To Predict The Shamblin Group On MR ImagingDevi MNessuna valutazione finora
- Morphometric Study of The Atlas: Estudo Morfométrico Do AtlasDocumento8 pagineMorphometric Study of The Atlas: Estudo Morfométrico Do AtlasazevedoNessuna valutazione finora
- Neckshaft AngleDocumento5 pagineNeckshaft Angleritee.shresthaNessuna valutazione finora
- Conséquence Neuro Des TorticolisDocumento10 pagineConséquence Neuro Des TorticolisLaidetNessuna valutazione finora
- The Journal of ArthroplastyDocumento4 pagineThe Journal of ArthroplastyFrancisco J DominguezNessuna valutazione finora
- Localizing The L5 Vertebra Using Nerve Morphology On MRI - An Accurate and Reliable TechniqueDocumento7 pagineLocalizing The L5 Vertebra Using Nerve Morphology On MRI - An Accurate and Reliable TechniqueThiago Astil RizzettoNessuna valutazione finora
- Accuracy of Xray and Mri in Defining Tumor MarginDocumento7 pagineAccuracy of Xray and Mri in Defining Tumor MarginDinda SaviraNessuna valutazione finora
- Vestibular SchwanomaDocumento10 pagineVestibular SchwanomaUsman Agus PrasetyoNessuna valutazione finora
- Por Qué Los Ortodoncistas Necesitan Saber Sobre La Hipomineralización de Los Incisivos MolaresDocumento1 paginaPor Qué Los Ortodoncistas Necesitan Saber Sobre La Hipomineralización de Los Incisivos MolaresmiriancoguevargasNessuna valutazione finora
- Radiotherapy and OncologyDocumento8 pagineRadiotherapy and OncologyÁgnes ZongorNessuna valutazione finora
- Nasal Cavity Shape in Unilateral Choanal Atresia and The Role of Fetal Ventilation in Facial GrowthDocumento6 pagineNasal Cavity Shape in Unilateral Choanal Atresia and The Role of Fetal Ventilation in Facial GrowthNalendra Tri WidhianartoNessuna valutazione finora
- Brs 0000000000000335Documento11 pagineBrs 0000000000000335Suttinont SurapuchongNessuna valutazione finora
- AJODO-2013 Barghan 143 6 888Documento5 pagineAJODO-2013 Barghan 143 6 888player osamaNessuna valutazione finora
- The Knee: Parm Johal, Mohammed A. Hassaballa, Jonathan D. Eldridge, Andrew J. PorteousDocumento3 pagineThe Knee: Parm Johal, Mohammed A. Hassaballa, Jonathan D. Eldridge, Andrew J. Porteousosman gorkemNessuna valutazione finora
- Wilson 2017Documento13 pagineWilson 2017DaniNessuna valutazione finora
- 1613 FullDocumento4 pagine1613 FullDanu BagoesNessuna valutazione finora
- Seguridad Social en AlemaniaDocumento8 pagineSeguridad Social en AlemaniaMichael RojasNessuna valutazione finora
- Ce (Ra1) F (T) PF1 (Sy SS) Pfa (Sy SS)Documento4 pagineCe (Ra1) F (T) PF1 (Sy SS) Pfa (Sy SS)Abhilash VemulaNessuna valutazione finora
- Retrospective Study of Craniovertebral Junction (CVJ) Anomalies: A Clinical Profi Le and Outcome Analysis of Surgically Treated PatientsDocumento7 pagineRetrospective Study of Craniovertebral Junction (CVJ) Anomalies: A Clinical Profi Le and Outcome Analysis of Surgically Treated PatientsNaga MuthuNessuna valutazione finora
- TC YrmnDocumento18 pagineTC Yrmnangelica cuevasNessuna valutazione finora
- 5550-Article Text-42309-3-10-20220104Documento8 pagine5550-Article Text-42309-3-10-20220104the OGs. 96Nessuna valutazione finora
- Assessment of Location and Course of Inferior Alveolar Canal Using Cone Beam Computed TomographyDocumento17 pagineAssessment of Location and Course of Inferior Alveolar Canal Using Cone Beam Computed TomographyIJAR JOURNALNessuna valutazione finora
- 16.pjohns-26-5prevertebral Soft Tissue ThicknessDocumento5 pagine16.pjohns-26-5prevertebral Soft Tissue ThicknessWahyu JuliandaNessuna valutazione finora
- 2011 - Kim, Kim, Beriwal - Contouring Inguinal and Femoral Nodes How Much Margin Is Needed Around The VesselsDocumento1 pagina2011 - Kim, Kim, Beriwal - Contouring Inguinal and Femoral Nodes How Much Margin Is Needed Around The VesselsPoljarLijanNessuna valutazione finora
- Chong 2015Documento5 pagineChong 2015yaniNessuna valutazione finora
- 20026Documento7 pagine20026zelvininaprilia990Nessuna valutazione finora
- Assessment of Radial Torsion Using Computed Tomography in Dogs With and Without Antebrachial Limb DeformityDocumento8 pagineAssessment of Radial Torsion Using Computed Tomography in Dogs With and Without Antebrachial Limb DeformityNathaly DejoyNessuna valutazione finora
- Of Mandibular Condylar Positi Ntal Occlusion Factors in An Somatic PopulationDocumento7 pagineOf Mandibular Condylar Positi Ntal Occlusion Factors in An Somatic PopulationDanilo BorjaNessuna valutazione finora
- 2 PDFDocumento6 pagine2 PDFOtto NaftariNessuna valutazione finora
- Elbow Radiographic Anatomy Measurement TDocumento11 pagineElbow Radiographic Anatomy Measurement TRadoi Sandina RodicaNessuna valutazione finora
- 1530 Jul 27Documento6 pagine1530 Jul 27kelvin amahNessuna valutazione finora
- Schei de Man 1980Documento17 pagineSchei de Man 1980Stefany ArzuzaNessuna valutazione finora
- Craniocervical Instability in Patients With Hypermobility Connective Disorders 2165 7939 1000299 PDFDocumento3 pagineCraniocervical Instability in Patients With Hypermobility Connective Disorders 2165 7939 1000299 PDFATRAGENessuna valutazione finora
- 01 - Diagnosing Childhood Acetabular Dysplasia Using The Lateral Margin of The SourcilDocumento9 pagine01 - Diagnosing Childhood Acetabular Dysplasia Using The Lateral Margin of The Sourcilcarloa marioNessuna valutazione finora
- Building A Better Mousetrap: The Diagnosis of Metastatic Cervical AdenopathyDocumento4 pagineBuilding A Better Mousetrap: The Diagnosis of Metastatic Cervical Adenopathyyaya1yaya1Nessuna valutazione finora
- A Novel Method For Assessing Postoperative Femoral Head Reduction in Developmental Dysplasia of The HipDocumento6 pagineA Novel Method For Assessing Postoperative Femoral Head Reduction in Developmental Dysplasia of The HipmicNessuna valutazione finora
- Surgical Management of Chordoma - A Systematic ReviewDocumento17 pagineSurgical Management of Chordoma - A Systematic ReviewHugo JBNessuna valutazione finora
- Quantifying Scaphoid Malalignment Based Upon Height-to-Length Ratios Obtained by 3-Dimensional Computed TomographyDocumento7 pagineQuantifying Scaphoid Malalignment Based Upon Height-to-Length Ratios Obtained by 3-Dimensional Computed TomographyLUIS SALVADOR FLORESNessuna valutazione finora
- Gamma Knife in CPA TUmorDocumento11 pagineGamma Knife in CPA TUmorGorila JuliNessuna valutazione finora
- J Ultrasmedbio 2014 12 509Documento1 paginaJ Ultrasmedbio 2014 12 509Mahatria RajNessuna valutazione finora
- MRI of the Spine: A Guide for Orthopedic SurgeonsDa EverandMRI of the Spine: A Guide for Orthopedic SurgeonsNessuna valutazione finora
- Aa DistriDocumento3 pagineAa Distriakosiminda143Nessuna valutazione finora
- KKS Equipment Matrik No PM Description PM StartDocumento3 pagineKKS Equipment Matrik No PM Description PM StartGHAZY TUBeNessuna valutazione finora
- Sheridan Specialized Building Products LLC - Queue Solutions Commercial Proposal by SeQure TechnologiesDocumento6 pagineSheridan Specialized Building Products LLC - Queue Solutions Commercial Proposal by SeQure Technologiessailesh psNessuna valutazione finora
- HP 6940 Manual CompleteDocumento150 pagineHP 6940 Manual CompletepaglafouNessuna valutazione finora
- Claudia Maienborn, Semantics, 381Documento34 pagineClaudia Maienborn, Semantics, 381robert guimaraesNessuna valutazione finora
- Nurses Guide To Family Assessment and InterventionDocumento9 pagineNurses Guide To Family Assessment and InterventionKaye CorNessuna valutazione finora
- What Role Does Imagination Play in Producing Knowledge About The WorldDocumento1 paginaWhat Role Does Imagination Play in Producing Knowledge About The WorldNathanael Samuel KuruvillaNessuna valutazione finora
- Couvade SyndromeDocumento5 pagineCouvade SyndromejudssalangsangNessuna valutazione finora
- Synopsis SsDocumento14 pagineSynopsis SsJYOTI KATIYAR SVUNessuna valutazione finora
- MnemonicsDocumento1 paginaMnemonicsSunil Boyz-uNessuna valutazione finora
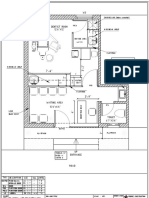
- Dental Clinic - Floor Plan R3-2Documento1 paginaDental Clinic - Floor Plan R3-2kanagarajodisha100% (1)
- Project 2 Analysis of Florida WaterDocumento8 pagineProject 2 Analysis of Florida WaterBeau Beauchamp100% (1)
- Instruction Manual Il-Obct-R1: Slip-Over Current Transformer ObctDocumento2 pagineInstruction Manual Il-Obct-R1: Slip-Over Current Transformer Obctبوحميدة كمالNessuna valutazione finora
- Hasan Bin Ekram: Career ObjectiveDocumento3 pagineHasan Bin Ekram: Career ObjectiveHasan SarikNessuna valutazione finora
- Speaking Quý 1 2024Documento43 pagineSpeaking Quý 1 2024Khang HoàngNessuna valutazione finora
- Opentext Documentum Archive Services For Sap: Configuration GuideDocumento38 pagineOpentext Documentum Archive Services For Sap: Configuration GuideDoond adminNessuna valutazione finora
- R917007195 Comando 8RDocumento50 pagineR917007195 Comando 8RRodrigues de OliveiraNessuna valutazione finora
- Code of Conduct For Public OfficialDocumento17 pagineCode of Conduct For Public OfficialHaNessuna valutazione finora
- University Grading System - VTUDocumento3 pagineUniversity Grading System - VTUmithilesh8144Nessuna valutazione finora
- Assignment OSDocumento11 pagineAssignment OSJunaidArshadNessuna valutazione finora
- BPI - I ExercisesDocumento241 pagineBPI - I Exercisesdivyajeevan89Nessuna valutazione finora
- Exchange 2010 UnderstandDocumento493 pagineExchange 2010 UnderstandSeKoFieNessuna valutazione finora
- Saeed Sentence Relation and Truth (Summary)Documento11 pagineSaeed Sentence Relation and Truth (Summary)Mohammad Hassan100% (1)
- You'Re My Everything - Glenn FredlyDocumento2 pagineYou'Re My Everything - Glenn FredlyTommy Juliansyah MarsenoNessuna valutazione finora
- Kalitantra-Shava Sadhana - WikipediaDocumento5 pagineKalitantra-Shava Sadhana - WikipediaGiano BellonaNessuna valutazione finora
- Poster PresentationDocumento3 paginePoster PresentationNipun RavalNessuna valutazione finora