Potrebbero piacerti anche
- Workbook and Casebook For Goodman and Gilman's The Pharmacological Basis of Therapeutics - 1st Edition (2016)Documento785 pagineWorkbook and Casebook For Goodman and Gilman's The Pharmacological Basis of Therapeutics - 1st Edition (2016)David Esteves Echanique93% (28)
- Piracetam and Piracetam Like Drugs From Basic.4Documento26 paginePiracetam and Piracetam Like Drugs From Basic.4jsoriano6Nessuna valutazione finora
- Neuropharmacology: Invited ReviewDocumento13 pagineNeuropharmacology: Invited ReviewAnthony SedivyNessuna valutazione finora
- Neurobiology of Kratom and Its Main Alkaloid MitragynineDocumento12 pagineNeurobiology of Kratom and Its Main Alkaloid MitragynineabyssnepNessuna valutazione finora
- Jurnal IntoksikasiDocumento9 pagineJurnal IntoksikasiRatee KumalaNessuna valutazione finora
- 1 s2.0 S0163725899000480 MainDocumento18 pagine1 s2.0 S0163725899000480 Mainwaciy70505Nessuna valutazione finora
- Lamp1999 Farmacocinetica Del MetronidazolDocumento21 pagineLamp1999 Farmacocinetica Del MetronidazolYonatan Gómez VargasNessuna valutazione finora
- Lauren B. Marangell - Concise Guide To Psychopharmacology (Second Edition) (2006) (238s)Documento261 pagineLauren B. Marangell - Concise Guide To Psychopharmacology (Second Edition) (2006) (238s)Oscar Alejandro Cardenas QuinteroNessuna valutazione finora
- Neuroscience and Biobehavioral ReviewsDocumento14 pagineNeuroscience and Biobehavioral ReviewsAndreas SugihartaNessuna valutazione finora
- Quetiapina in SKDocumento16 pagineQuetiapina in SKRobert MovileanuNessuna valutazione finora
- Analgesics in Patients With Hepatic Impairment .6-3Documento25 pagineAnalgesics in Patients With Hepatic Impairment .6-3Domenico LombardiniNessuna valutazione finora
- Magnesium Sulfate in Eclampsia and Pre-Eclampsia: Pharmacokinetic PrinciplesDocumento10 pagineMagnesium Sulfate in Eclampsia and Pre-Eclampsia: Pharmacokinetic PrinciplesIzhhar GemilangNessuna valutazione finora
- Toxicology and PharmacologyDocumento10 pagineToxicology and PharmacologyPravin KumarNessuna valutazione finora
- Ky Nure Nine AddictionDocumento17 pagineKy Nure Nine AddictionBlake BNessuna valutazione finora
- Addiction and 5HTDocumento47 pagineAddiction and 5HTByanca CamachoNessuna valutazione finora
- A05 001Documento59 pagineA05 001jaimeNessuna valutazione finora
- Clinical Pharmacokinetics of Amfetamine and Related SubstancesDocumento29 pagineClinical Pharmacokinetics of Amfetamine and Related SubstancesJoshua RibeiroNessuna valutazione finora
- Shock – modern clinical treatment conceptsDa EverandShock – modern clinical treatment conceptsNessuna valutazione finora
- 1 s2.0 S1936523320303818 MainDocumento11 pagine1 s2.0 S1936523320303818 MainAndi SuhriyanaNessuna valutazione finora
- Effects of Hypothermia On Pharmacokinetics and Pharmacodynamics A Systematic Review of Preclinical and Clinical StudiesDocumento18 pagineEffects of Hypothermia On Pharmacokinetics and Pharmacodynamics A Systematic Review of Preclinical and Clinical StudiesБагдат БримовNessuna valutazione finora
- Rosuvastatin A Review of Its Use in The.5Documento18 pagineRosuvastatin A Review of Its Use in The.5urbanincultureNessuna valutazione finora
- Studies With Psychedelic Drugs in Human VolunteersDocumento19 pagineStudies With Psychedelic Drugs in Human VolunteersbeneNessuna valutazione finora
- The Triptans: A Summary: CNS Drugs November 1999Documento16 pagineThe Triptans: A Summary: CNS Drugs November 1999Divaz HedyaNessuna valutazione finora
- Sorkin 1987Documento50 pagineSorkin 1987Galuh EkaNessuna valutazione finora
- Duloxetine: Clinical Pharmacokinetics and Drug InteractionsDocumento14 pagineDuloxetine: Clinical Pharmacokinetics and Drug InteractionsMario HBNessuna valutazione finora
- Pharmacology & Therapeutics: Karsten K. Madsen, H. Steve White, Arne SchousboeDocumento8 paginePharmacology & Therapeutics: Karsten K. Madsen, H. Steve White, Arne SchousboeDr. Kaushal Kishor SharmaNessuna valutazione finora
- Nicotine Use in Schizophrenia: The Self Medication HypothesesDocumento14 pagineNicotine Use in Schizophrenia: The Self Medication Hypothesesbluedevil2790Nessuna valutazione finora
- Cheer 2004Documento31 pagineCheer 2004bagusarditya husadhaNessuna valutazione finora
- Antipsicoticos AtipicosDocumento21 pagineAntipsicoticos AtipicosAndrea CoronaNessuna valutazione finora
- Adherence To Antipsychotics in Schizophrenia PDFDocumento168 pagineAdherence To Antipsychotics in Schizophrenia PDFCosmin Ungureanu100% (1)
- Unit 30Documento17 pagineUnit 30BeenishFatimaNessuna valutazione finora
- Hayley Depressioncomorbid2 Lect3401Documento74 pagineHayley Depressioncomorbid2 Lect3401Shawn HayleyNessuna valutazione finora
- Ketamine JaffdispubDocumento12 pagineKetamine JaffdispubT Smith AndresNessuna valutazione finora
- Farmacocinetica y Farmacodinami de MMF Clin Pharmacokinet 2007 46 1 13-58Documento46 pagineFarmacocinetica y Farmacodinami de MMF Clin Pharmacokinet 2007 46 1 13-58Maria Marina Papaginovic LeivaNessuna valutazione finora
- Qi Chong 2021 Do Medicines Commonly Used by Older Adults Impact Their Nutriente StatusDocumento15 pagineQi Chong 2021 Do Medicines Commonly Used by Older Adults Impact Their Nutriente StatusJennifer AnguloNessuna valutazione finora
- EscitalopramDocumento21 pagineEscitalopramalejandra torresNessuna valutazione finora
- The Pharmacology of StatinsDocumento9 pagineThe Pharmacology of StatinsSantiago BaronNessuna valutazione finora
- Advanced Drug Delivery Reviews: Contents Lists Available atDocumento32 pagineAdvanced Drug Delivery Reviews: Contents Lists Available atLe Victor DungNessuna valutazione finora
- Analytical Methods To Monitor Dopamine Metabolism in Plasma-DADocumento28 pagineAnalytical Methods To Monitor Dopamine Metabolism in Plasma-DAKuanNessuna valutazione finora
- Tocolytic AgentDocumento13 pagineTocolytic AgentHania Asmarani RahmanitaNessuna valutazione finora
- Goodman and Gilman's The Pharmacological Basis of TherapeuticsDocumento105 pagineGoodman and Gilman's The Pharmacological Basis of TherapeuticsDiky PratamaNessuna valutazione finora
- Sumtriptan Mas NaproxenoDocumento79 pagineSumtriptan Mas NaproxenoLeonardo Antonio Medina AguileraNessuna valutazione finora
- Atomoxetine: A Review of Its Use in Attention-Deficit Hyperactivity Disorder in Children and AdolescentsDocumento24 pagineAtomoxetine: A Review of Its Use in Attention-Deficit Hyperactivity Disorder in Children and AdolescentsGanellNessuna valutazione finora
- Drug Medi Int-EngDocumento25 pagineDrug Medi Int-EngnurayuramndaniNessuna valutazione finora
- Pharmacodynamics and Pharmacokinetics of Spiramycin and Their Clinical SignificanceDocumento8 paginePharmacodynamics and Pharmacokinetics of Spiramycin and Their Clinical SignificanceSalmadiar Riska UlimazaimNessuna valutazione finora
- VZVXXXZVDocumento342 pagineVZVXXXZVRahul GuptaNessuna valutazione finora
- Cockshott2000 Article ClinicalPharmacokineticsOfGoseDocumento24 pagineCockshott2000 Article ClinicalPharmacokineticsOfGoseChurrizo IslamiNessuna valutazione finora
- PharmacistsDocumento16 paginePharmacistsanon-20862Nessuna valutazione finora
- Mitragina Analytical StudyDocumento49 pagineMitragina Analytical Studycts5131Nessuna valutazione finora
- EmbalmingDocumento9 pagineEmbalmingEvi LoNessuna valutazione finora
- Free Drug Metabolic Clearance in Elderly People: and Evan J. BeggDocumento25 pagineFree Drug Metabolic Clearance in Elderly People: and Evan J. BeggPei Ru ChinNessuna valutazione finora
- Clinical Pharmacokinetics Volume 50 Issue 2 2011 (Doi 10.2165/11534750-000000000-00000) DR Garry G. Graham, Jeroen Punt, Manit Arora, Richard O. Day, Ma - Clinical Pharmacokinetics of MetforminDocumento18 pagineClinical Pharmacokinetics Volume 50 Issue 2 2011 (Doi 10.2165/11534750-000000000-00000) DR Garry G. Graham, Jeroen Punt, Manit Arora, Richard O. Day, Ma - Clinical Pharmacokinetics of MetforminRob Sandoval StebanNessuna valutazione finora
- Tireoide e MitocondriaDocumento11 pagineTireoide e MitocondriaAdelia DominiqueNessuna valutazione finora
- Devillier 2008Documento14 pagineDevillier 2008LeonardoMartínezNessuna valutazione finora
- Antidepressants For Smoking Cessation (Review)Documento125 pagineAntidepressants For Smoking Cessation (Review)ammar_ashor100% (1)
- Conventional Drug Delivery Routes, Recent Developments and Future Prospects - Tugas SPO "Documento21 pagineConventional Drug Delivery Routes, Recent Developments and Future Prospects - Tugas SPO "Niken Dwi100% (1)
- Selección de Antibióticos Por Vía Parenteral en Pacientes AmbulatoriosDocumento25 pagineSelección de Antibióticos Por Vía Parenteral en Pacientes AmbulatoriosErick Antonio Castillo Gurdian100% (1)
- Cyclophosphamide Versus Methylprednisolone For Treating Neuropsychiatric Involvement in Systemic Lupus Erythematosus (Review)Documento33 pagineCyclophosphamide Versus Methylprednisolone For Treating Neuropsychiatric Involvement in Systemic Lupus Erythematosus (Review)Jocsi Barros HerreraNessuna valutazione finora
- Sample OutputDocumento110 pagineSample OutputMohana MuraliNessuna valutazione finora
- Dyslipoproteinemia - Strategies for Diagnosis and TherapyDa EverandDyslipoproteinemia - Strategies for Diagnosis and TherapyNessuna valutazione finora
- Histori Nilai Kandidat UKMPPD Feb 2019Documento25 pagineHistori Nilai Kandidat UKMPPD Feb 2019Fariz RifqiNessuna valutazione finora
- Elektif Maret 2019Documento59 pagineElektif Maret 2019Fariz RifqiNessuna valutazione finora
- Paulzen 2016Documento3 paginePaulzen 2016Fariz RifqiNessuna valutazione finora
- Valproic Acid and Risperidone: A Drug Interaction?: To The EditorDocumento2 pagineValproic Acid and Risperidone: A Drug Interaction?: To The EditorFariz RifqiNessuna valutazione finora
- Flanagan Et Al 2019Documento9 pagineFlanagan Et Al 2019Regulatório IndividualNessuna valutazione finora
- Injection Product List HDocumento11 pagineInjection Product List Halnikki25kNessuna valutazione finora
- Propranolol ER Capsule 018553 RC07-14Documento2 paginePropranolol ER Capsule 018553 RC07-14Gloria J GonzálezNessuna valutazione finora
- GCC Human Drugs Subv2.1Documento103 pagineGCC Human Drugs Subv2.1AmrNessuna valutazione finora
- Doctor ExhibitDocumento110 pagineDoctor ExhibitKFORNessuna valutazione finora
- AMRI API ProductCatalog WebDocumento16 pagineAMRI API ProductCatalog Webমোঃ এমদাদুল হকNessuna valutazione finora
- Printed Material Module 7 Gastrointestinal System Drugs - PDFDocumento45 paginePrinted Material Module 7 Gastrointestinal System Drugs - PDFShang MacarayonNessuna valutazione finora
- Surat Pesanan Obat Apotek Ym 123Documento4 pagineSurat Pesanan Obat Apotek Ym 123ymNessuna valutazione finora
- Responsible Use of Opioid in Indonesia: Highlight On OxycodoneDocumento34 pagineResponsible Use of Opioid in Indonesia: Highlight On OxycodonearifwahyudiNessuna valutazione finora
- Potassium CHLORIDEDocumento20 paginePotassium CHLORIDEAnto PaulNessuna valutazione finora
- Drowsiness, Sedation, LightDocumento2 pagineDrowsiness, Sedation, LightGrape JuiceNessuna valutazione finora
- Dose Response CurveDocumento29 pagineDose Response CurveMaria khurshidNessuna valutazione finora
- JNC8 HTNDocumento2 pagineJNC8 HTNTaradifaNurInsi0% (1)
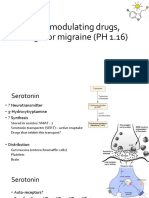
- 5-HT Modulating Drugs, Drugs For Migraine (PH 1.16)Documento13 pagine5-HT Modulating Drugs, Drugs For Migraine (PH 1.16)shruti sangwanNessuna valutazione finora
- Bisoprolol PDFDocumento69 pagineBisoprolol PDFDuwi Efasari100% (3)
- Gastrointestinal Diseases: Clinical Pharmacist Hasan BayashotDocumento117 pagineGastrointestinal Diseases: Clinical Pharmacist Hasan BayashotRawabi SalehNessuna valutazione finora
- DOSIS ANAK Obat SirupDocumento2 pagineDOSIS ANAK Obat SirupSiti Hardiyanti BaharuddinNessuna valutazione finora
- Classification and Pharmacology of ProgestinsDocumento10 pagineClassification and Pharmacology of ProgestinsancaNessuna valutazione finora
- Laporan Stok Harian 27 JANUARI 2022Documento64 pagineLaporan Stok Harian 27 JANUARI 2022HakimNessuna valutazione finora
- First-Pass EffectDocumento2 pagineFirst-Pass EffectMartin CelestinoNessuna valutazione finora
- WHO Policy Statement - The Use of Opened Multi-Dose Vials of Vaccine in Subsequent Immunization SessionsDocumento13 pagineWHO Policy Statement - The Use of Opened Multi-Dose Vials of Vaccine in Subsequent Immunization SessionscristineNessuna valutazione finora
- CPS Info Dimenhydrinate (Gravol)Documento5 pagineCPS Info Dimenhydrinate (Gravol)Ann A.Nessuna valutazione finora
- Demerol DrugDocumento2 pagineDemerol DrugMsOrange100% (1)
- Therapeutics in Aquaculture (AAH 301 1+1)Documento25 pagineTherapeutics in Aquaculture (AAH 301 1+1)RISHIKANessuna valutazione finora
- N Main DivisionDocumento14 pagineN Main DivisiondhananjaybhatejaNessuna valutazione finora
- GLP-1 Analog Dosing ChartDocumento1 paginaGLP-1 Analog Dosing ChartTheepan Thurai100% (1)
- Rekapan Kendali StokDocumento10 pagineRekapan Kendali StokRirin RistianiNessuna valutazione finora
- AntibioticsDocumento13 pagineAntibioticsJOrgeNessuna valutazione finora
- New QuestionnreDocumento3 pagineNew Questionnreawadesh44raiNessuna valutazione finora
- Tocolytic AgentDocumento13 pagineTocolytic AgentHania Asmarani RahmanitaNessuna valutazione finora