Potrebbero piacerti anche
- A Sample of The Completed Essential Principles Conformity Checklist MD CCLDocumento12 pagineA Sample of The Completed Essential Principles Conformity Checklist MD CCLAyman Ali100% (1)
- HESU OrganogramDocumento29 pagineHESU OrganogramHEMS SAMCH100% (4)
- AO 2016-0006 Revised Guidelines On The Surveillance and Response of AEFIDocumento22 pagineAO 2016-0006 Revised Guidelines On The Surveillance and Response of AEFIReanne Pauline Manipon100% (2)
- Ewars BrochureDocumento2 pagineEwars Brochuresheela bethapudiNessuna valutazione finora
- AO 2010-0017 - AEFI SurveillanceDocumento14 pagineAO 2010-0017 - AEFI SurveillancereynulfomdNessuna valutazione finora
- National Infection Prevention and Control Board Assurance FrameworkDocumento55 pagineNational Infection Prevention and Control Board Assurance FrameworkhebasnmcNessuna valutazione finora
- 1 - AEFI Management - May 6, 2021Documento29 pagine1 - AEFI Management - May 6, 2021niel dejarmeNessuna valutazione finora
- ADL Future of Pharmacovigilance 1674559487Documento8 pagineADL Future of Pharmacovigilance 1674559487Irvins vietnamNessuna valutazione finora
- AO 2022 0051 Revised National Policy On Infection Prevention and Control in All Public and Private Health FacilitiesDocumento19 pagineAO 2022 0051 Revised National Policy On Infection Prevention and Control in All Public and Private Health FacilitiesBrian VargasNessuna valutazione finora
- DC 2023-0223 - Reporting Process in The Monitoring of Health Facility Preparedness and Health-Related Events During El NinoDocumento14 pagineDC 2023-0223 - Reporting Process in The Monitoring of Health Facility Preparedness and Health-Related Events During El NinoDigos Doctors' Hospital, Inc. IT DepartmentNessuna valutazione finora
- Guidelines in Surveillance and Response To Adverse Events Following Immunization (AEFI)Documento71 pagineGuidelines in Surveillance and Response To Adverse Events Following Immunization (AEFI)Fred C. MirandaNessuna valutazione finora
- F:/P11/NHI/TRICOMM/AAHCA09 - 001.XML: ON Reemption of Tate AWSDocumento8 pagineF:/P11/NHI/TRICOMM/AAHCA09 - 001.XML: ON Reemption of Tate AWSVino DNessuna valutazione finora
- dm2022 0033Documento7 paginedm2022 0033barogregNessuna valutazione finora
- Work Instruction For Management of AEFI MungaparDocumento18 pagineWork Instruction For Management of AEFI Mungaparworkwithsumit02Nessuna valutazione finora
- Vigilance ReportingDocumento6 pagineVigilance Reportingashwin AshwinNessuna valutazione finora
- India AEFI Guidelines FINAL Draft DocumentDocumento67 pagineIndia AEFI Guidelines FINAL Draft DocumentPrabir Kumar ChatterjeeNessuna valutazione finora
- DOH 210111 DM 2021 0047 Interim Guidelines On Masterlisting For The COVID 19 Electronic Immunization Registry CEIR Phase 1Documento9 pagineDOH 210111 DM 2021 0047 Interim Guidelines On Masterlisting For The COVID 19 Electronic Immunization Registry CEIR Phase 1kima conNessuna valutazione finora
- Ethical Consideration in Nursing Republic ActsDocumento16 pagineEthical Consideration in Nursing Republic Acts- HY0ENGJUNNessuna valutazione finora
- Ao2022 0005Documento29 pagineAo2022 0005Tristan del RosarioNessuna valutazione finora
- National Tech Guidelines For IsdrDocumento616 pagineNational Tech Guidelines For IsdrYahya H SakwaNessuna valutazione finora
- Jpeck,+june2021 Telemetry Monitoring SpreadDocumento2 pagineJpeck,+june2021 Telemetry Monitoring Spreadtublight sNessuna valutazione finora
- Ao 2011-0009Documento21 pagineAo 2011-0009Joline UrbinaNessuna valutazione finora
- CHN 2 MidtermsDocumento16 pagineCHN 2 MidtermsDarylle Hannah De GuzmanNessuna valutazione finora
- National Pharmacovigilance Roadmap 2020Documento39 pagineNational Pharmacovigilance Roadmap 2020TafereMulawNessuna valutazione finora
- Departmental Experience and Lessons Learned With Accelerated Introduction of Telemedicine During The COVID-19 CrisisDocumento8 pagineDepartmental Experience and Lessons Learned With Accelerated Introduction of Telemedicine During The COVID-19 Crisistresy kalawaNessuna valutazione finora
- Assistant: SecretariesDocumento15 pagineAssistant: Secretarieskima conNessuna valutazione finora
- DOH AO 2016-0002 National Policy On Infection Prevention & Control in Healthcare FacilitiesDocumento9 pagineDOH AO 2016-0002 National Policy On Infection Prevention & Control in Healthcare FacilitiesAmeng Gosim100% (1)
- NPVGDocumento109 pagineNPVGMuhammad Noman bin FiazNessuna valutazione finora
- Dilg Memocircular 2021123 - Acae50912eDocumento4 pagineDilg Memocircular 2021123 - Acae50912ejvpvillanuevaNessuna valutazione finora
- Office of The Secretary: InterimDocumento8 pagineOffice of The Secretary: InterimRvBombetaNessuna valutazione finora
- Office of The: SecretaryDocumento15 pagineOffice of The: SecretaryMark RiveraNessuna valutazione finora
- Executive Order Template (MESU)Documento5 pagineExecutive Order Template (MESU)IKay Floresta Valencia100% (1)
- Organisation of Resilient Health and Social Care Following The Covid-19 PandemicDocumento2 pagineOrganisation of Resilient Health and Social Care Following The Covid-19 PandemicChristineNessuna valutazione finora
- Revised AEFI Guidelines Execute SummaryDocumento8 pagineRevised AEFI Guidelines Execute SummarymadhuNessuna valutazione finora
- Biological Evaluation of Medical DevicesDocumento6 pagineBiological Evaluation of Medical DevicesCarlos Alberto Torres LunaNessuna valutazione finora
- Office: of The SecretaryDocumento8 pagineOffice: of The SecretaryLyht TVNessuna valutazione finora
- 20.01.2020 Advisory On Novel Coronavirus Outbreak in Wuhan City of ChinaDocumento3 pagine20.01.2020 Advisory On Novel Coronavirus Outbreak in Wuhan City of ChinaShiv kumarNessuna valutazione finora
- Guidelines On The Implementation of Telemedicine in The Delivery of Individual-Based Health ServicesDocumento29 pagineGuidelines On The Implementation of Telemedicine in The Delivery of Individual-Based Health ServicesKristel HipolitoNessuna valutazione finora
- National EPI 2021 PDFDocumento40 pagineNational EPI 2021 PDFyeabsira gashawNessuna valutazione finora
- Philly COVID-19 Restaurant Safety Checklist & Outdoor Dining GuidelinesDocumento42 paginePhilly COVID-19 Restaurant Safety Checklist & Outdoor Dining GuidelinesPhillyVoice.com100% (1)
- R F I R: Edesigning The ALL Ncident EportDocumento9 pagineR F I R: Edesigning The ALL Ncident EportSheNessuna valutazione finora
- (HPB) 3 (1) Protecting Consumers Through Improved Pharmacovigilance PDFDocumento2 pagine(HPB) 3 (1) Protecting Consumers Through Improved Pharmacovigilance PDFMaria roxanne HernandezNessuna valutazione finora
- Office: The of The SecretaryDocumento25 pagineOffice: The of The SecretaryJoseph Raymund BautistaNessuna valutazione finora
- Event-Based Surveillance Protocol: Disease Control Division Ministry of Health Malaysia 2018Documento42 pagineEvent-Based Surveillance Protocol: Disease Control Division Ministry of Health Malaysia 2018Kalpanah GurumurthyNessuna valutazione finora
- dc2020-0321 DOH PRC PCW CertificationDocumento7 paginedc2020-0321 DOH PRC PCW Certificationiamaj8Nessuna valutazione finora
- WWW - Csc.gov - PH - Phocadownload - MC2021 - MC No. 16, S. 2021Documento6 pagineWWW - Csc.gov - PH - Phocadownload - MC2021 - MC No. 16, S. 2021esmie distorNessuna valutazione finora
- Facility-Based Surveillance Activities For COVID-19 Infection and Outcomes AmongDocumento7 pagineFacility-Based Surveillance Activities For COVID-19 Infection and Outcomes AmongDr. CiciNessuna valutazione finora
- Drug Information Journal 2005 Jefferys 73 80Documento8 pagineDrug Information Journal 2005 Jefferys 73 80MIGUEL ANGEL CASTRO LEALNessuna valutazione finora
- dm2023-0339 Reiteration On Providing Adherence Counseling and Employing Multi-Month Dispensing of Antiretroviral (ARV) Drugs For PLHIVDocumento2 paginedm2023-0339 Reiteration On Providing Adherence Counseling and Employing Multi-Month Dispensing of Antiretroviral (ARV) Drugs For PLHIVithran khoNessuna valutazione finora
- Surveillance System For Attacks On Health Care (SSA)Documento34 pagineSurveillance System For Attacks On Health Care (SSA)bonface njiririNessuna valutazione finora
- Ceir Presentation 01132021Documento16 pagineCeir Presentation 01132021Norman PosugacNessuna valutazione finora
- Onclusions AND Ecommendations: Xvii. ConclusionsDocumento13 pagineOnclusions AND Ecommendations: Xvii. ConclusionsMarco CastroNessuna valutazione finora
- HCPN Orientation 1Documento39 pagineHCPN Orientation 1jai ebuenNessuna valutazione finora
- Office of The Secretary: RegionDocumento25 pagineOffice of The Secretary: RegionMarky OlorvidaNessuna valutazione finora
- Ra 10918 - Legal PharmacyDocumento13 pagineRa 10918 - Legal PharmacyAlyssa PascualNessuna valutazione finora
- Who Adverse Events Following Immunization (Aefi) Causality Assessment 815Documento2 pagineWho Adverse Events Following Immunization (Aefi) Causality Assessment 815VaccineInformation100% (2)
- Initial Implementation Guidance For Federal Agencies On Updates To Federal Agency COVID-19 Workplace Safety ProtocolsDocumento11 pagineInitial Implementation Guidance For Federal Agencies On Updates To Federal Agency COVID-19 Workplace Safety ProtocolsFedSmith Inc.Nessuna valutazione finora
- Office THE: OF SecretaryDocumento12 pagineOffice THE: OF SecretaryJomelle WongNessuna valutazione finora
- AEFI-Monitoring-and-Reporting-2023Documento22 pagineAEFI-Monitoring-and-Reporting-2023City Health Center 6 CaalibangbanganNessuna valutazione finora
- Manual for the Management of Operations during an Animal Health EmergencyDa EverandManual for the Management of Operations during an Animal Health EmergencyNessuna valutazione finora
- Tutorial 1 Process Heat TransferDocumento4 pagineTutorial 1 Process Heat TransferSuraya JohariNessuna valutazione finora
- TCRP Wheel Rail Noise ReportDocumento220 pagineTCRP Wheel Rail Noise ReportAnonymous OmwbxkB100% (1)
- 101 Union of Filipro Employees Vs Vivar (Labor)Documento1 pagina101 Union of Filipro Employees Vs Vivar (Labor)Kayelyn Lat100% (1)
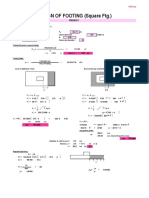
- Design of Footing (Square FTG.) : M Say, L 3.75Documento2 pagineDesign of Footing (Square FTG.) : M Say, L 3.75victoriaNessuna valutazione finora
- Manual On Power System ProtectionDocumento393 pagineManual On Power System ProtectionSakthi Murugan88% (17)
- CSP Study Course 2 Willard StephensonDocumento137 pagineCSP Study Course 2 Willard Stephensonsamer alrawashdehNessuna valutazione finora
- 1.2 Server Operating SystemDocumento20 pagine1.2 Server Operating SystemAzhar AhmadNessuna valutazione finora
- Engineer Noor Ahmad CVDocumento5 pagineEngineer Noor Ahmad CVSayed WafiNessuna valutazione finora
- A Job InterviewDocumento8 pagineA Job Interviewa.rodriguezmarcoNessuna valutazione finora
- Forecasting and Demand Management PDFDocumento39 pagineForecasting and Demand Management PDFKazi Ajwad AhmedNessuna valutazione finora
- 2017 Directory WO Member PagesDocumento112 pagine2017 Directory WO Member PagessberkowitzNessuna valutazione finora
- Option - 1 Option - 2 Option - 3 Option - 4 Correct Answer MarksDocumento4 pagineOption - 1 Option - 2 Option - 3 Option - 4 Correct Answer MarksKISHORE BADANANessuna valutazione finora
- VM PDFDocumento4 pagineVM PDFTembre Rueda RaúlNessuna valutazione finora
- Fixed Plug-In Motor A2Fe: Series 6Documento24 pagineFixed Plug-In Motor A2Fe: Series 6Michail ArmitageNessuna valutazione finora
- Research On The Marketing Communication Strategy of Tesla Motors in China Under The Background of New MediaDocumento5 pagineResearch On The Marketing Communication Strategy of Tesla Motors in China Under The Background of New MediaSiddharth ChaudharyNessuna valutazione finora
- Rule 63Documento43 pagineRule 63Lady Paul SyNessuna valutazione finora
- Hey Can I Try ThatDocumento20 pagineHey Can I Try Thatapi-273078602Nessuna valutazione finora
- Student ManualDocumento19 pagineStudent ManualCarl Jay TenajerosNessuna valutazione finora
- MBA-CM - ME - Lecture 16 Market Structure AnalysisDocumento11 pagineMBA-CM - ME - Lecture 16 Market Structure Analysisrohan_solomonNessuna valutazione finora
- 580N 580SN 580SN WT 590SN With POWERSHUTTLE ELECTRICAL SCHEMATICDocumento2 pagine580N 580SN 580SN WT 590SN With POWERSHUTTLE ELECTRICAL SCHEMATICEl Perro100% (1)
- 00 Saip 76Documento10 pagine00 Saip 76John BuntalesNessuna valutazione finora
- Question BankDocumento42 pagineQuestion Bank02 - CM Ankita AdamNessuna valutazione finora
- Software Test ISO StandardsDocumento2 pagineSoftware Test ISO StandardsTony DavisNessuna valutazione finora
- Raport de Incercare TL 82 Engleza 2015 MasticDocumento3 pagineRaport de Incercare TL 82 Engleza 2015 MasticRoxana IoanaNessuna valutazione finora
- David Sm15 Inppt 06Documento57 pagineDavid Sm15 Inppt 06Halima SyedNessuna valutazione finora
- Astm D2940 D2940M 09Documento1 paginaAstm D2940 D2940M 09INDIRA DEL CARMEN BERMEJO FERN�NDEZNessuna valutazione finora
- Wind Turbines Fundamentals Technologies Application Economics 2nd EditionDocumento3 pagineWind Turbines Fundamentals Technologies Application Economics 2nd Editionhafidztampan0% (1)
- Thematic CodingDocumento31 pagineThematic CodingLance Jazekmiel DOMINGONessuna valutazione finora
- MSA & Destructive TestDocumento4 pagineMSA & Destructive Testanon_902607157100% (1)
- Link Belt Rec Parts LastDocumento15 pagineLink Belt Rec Parts LastBishoo ShenoudaNessuna valutazione finora