Potrebbero piacerti anche
- Brain Oscillations, Synchrony and Plasticity: Basic Principles and Application to Auditory-Related DisordersDa EverandBrain Oscillations, Synchrony and Plasticity: Basic Principles and Application to Auditory-Related DisordersNessuna valutazione finora
- Electroencephalographic Correlates of PsychometryDocumento4 pagineElectroencephalographic Correlates of PsychometrySabrina JonesNessuna valutazione finora
- Neural Correlates of Dispositional Mindfulness During Affect Labeling-560.FullDocumento6 pagineNeural Correlates of Dispositional Mindfulness During Affect Labeling-560.FullZenNessuna valutazione finora
- Brain Circuit Dysfunction in Post - Traumatic Stress Disorder: From Mouse To Man - Robert J. FensterDocumento17 pagineBrain Circuit Dysfunction in Post - Traumatic Stress Disorder: From Mouse To Man - Robert J. FensterAlvaro Arboledas LoriteNessuna valutazione finora
- The Lilly WaveDocumento1 paginaThe Lilly WaveErs IconoclastaNessuna valutazione finora
- Amato Asu 0010E 15958Documento558 pagineAmato Asu 0010E 15958Kat MurrayNessuna valutazione finora
- 10 Drives, Affects, Id Energies, and The Neuroscience of Emotions: Response To The Commentaries by Jaak Panksepp (Bowling Green, Ohio)Documento22 pagine10 Drives, Affects, Id Energies, and The Neuroscience of Emotions: Response To The Commentaries by Jaak Panksepp (Bowling Green, Ohio)Maximiliano PortilloNessuna valutazione finora
- The Detection of Electromagnetic Processes in The Ionosphere Caused by Seismic ActivityDocumento12 pagineThe Detection of Electromagnetic Processes in The Ionosphere Caused by Seismic Activityclaudiocastillo@gmail.comNessuna valutazione finora
- The Central Nervous System (CNS) Consists of The Brain and The Spinal Cord, Immersed in Cerebrospinal Fluid (CSF)Documento29 pagineThe Central Nervous System (CNS) Consists of The Brain and The Spinal Cord, Immersed in Cerebrospinal Fluid (CSF)userbarbosNessuna valutazione finora
- Effect of Electric and Magnetic Treatments On Germination of Bitter Gourd SeedDocumento6 pagineEffect of Electric and Magnetic Treatments On Germination of Bitter Gourd SeedspeknathsNessuna valutazione finora
- Principles of Anatomy and Physiology: Gerard J. Tortora - Bryan DerricksonDocumento12 paginePrinciples of Anatomy and Physiology: Gerard J. Tortora - Bryan DerricksonDiegoAlejandroCardonaNessuna valutazione finora
- Effects of Psilocybin On Hippocampal Neurogenesis and Extinction of Trace Fear ConditioningDocumento11 pagineEffects of Psilocybin On Hippocampal Neurogenesis and Extinction of Trace Fear ConditioningurkogNessuna valutazione finora
- The Physics and Neurobiology of MagnetoreDocumento10 pagineThe Physics and Neurobiology of MagnetoreAndrew LangeNessuna valutazione finora
- The Neurobiopolitics of Global Consciousness - Warren NeidichDocumento34 pagineThe Neurobiopolitics of Global Consciousness - Warren NeidichjohnnyNessuna valutazione finora
- The Brain Has A Body Adaptive Behavior Emerges From Interactions of Nervous System, Body and Environment by Hillel J. Chiel and Randall D. Beer 1997Documento5 pagineThe Brain Has A Body Adaptive Behavior Emerges From Interactions of Nervous System, Body and Environment by Hillel J. Chiel and Randall D. Beer 1997AmiraNessuna valutazione finora
- By Robert NaeslundDocumento17 pagineBy Robert Naeslundnelly1100% (1)
- Freud FailedDocumento20 pagineFreud FailedAbrar Mojeeb100% (1)
- Fifty Years of Supporting Parapsychology - The Parapsychology Foundation (1951-2001)Documento27 pagineFifty Years of Supporting Parapsychology - The Parapsychology Foundation (1951-2001)Pixel PerfectNessuna valutazione finora
- 1998 Parapsych Proceeding Part IIDocumento184 pagine1998 Parapsych Proceeding Part IIjossbrown3784100% (1)
- 2016 - A Possible Flux Density Value of 10 - 12 W M - 2 For 'Spontaneous' Photon Emissions in Fixed Human Brain Tissue Was Spinoza CorrectDocumento5 pagine2016 - A Possible Flux Density Value of 10 - 12 W M - 2 For 'Spontaneous' Photon Emissions in Fixed Human Brain Tissue Was Spinoza CorrectraduNessuna valutazione finora
- Leading-Edge NeuroscienceDocumento3 pagineLeading-Edge Neurosciencegabyk68Nessuna valutazione finora
- Healing Through The Mind Author WellspringDocumento78 pagineHealing Through The Mind Author WellspringResearch Center for Training and Development100% (1)
- Esoteric Healing Modern PerspectiveDocumento4 pagineEsoteric Healing Modern PerspectiveMaria Luisa ParraNessuna valutazione finora
- Kirlian Photos Using Transparent ElectrodesDocumento31 pagineKirlian Photos Using Transparent Electrodesgrewa153Nessuna valutazione finora
- Brain PlasticityDocumento7 pagineBrain Plasticityfederson2760Nessuna valutazione finora
- Semantic Memory Cognitive and Neuroanatomical Perspectives - OriginalDocumento9 pagineSemantic Memory Cognitive and Neuroanatomical Perspectives - OriginalCarolina Paz Herrera RamosNessuna valutazione finora
- Galileo's Lament, and The Collapse of The Social SciencesDocumento246 pagineGalileo's Lament, and The Collapse of The Social SciencesArt MarrNessuna valutazione finora
- Russell - Circumplex ModelDocumento25 pagineRussell - Circumplex ModelBotorogeanu MirelaNessuna valutazione finora
- Behavioral Neuroscience, Also Known As Biological PsychologyDocumento11 pagineBehavioral Neuroscience, Also Known As Biological PsychologyConColNessuna valutazione finora
- Nicolas Rouleau and Michael A. Persinger: Key WordsDocumento15 pagineNicolas Rouleau and Michael A. Persinger: Key WordsSamuel HansonNessuna valutazione finora
- LIMBIC SYSTEM PPT by AmulyaDocumento54 pagineLIMBIC SYSTEM PPT by AmulyaSid KolgeNessuna valutazione finora
- We Are Electric Sally Adee - Livro ElectomaDocumento262 pagineWe Are Electric Sally Adee - Livro ElectomaFrancers FrançaNessuna valutazione finora
- Cap II - Curs 5 - 6 - Somatosensory System - 2014 - 2015 - PDFDocumento137 pagineCap II - Curs 5 - 6 - Somatosensory System - 2014 - 2015 - PDFMaria MadalinaNessuna valutazione finora
- Charles Tart - Marijuana Intoxication, Psi and Spiritual ExperiencesDocumento16 pagineCharles Tart - Marijuana Intoxication, Psi and Spiritual ExperiencesElianKithaNessuna valutazione finora
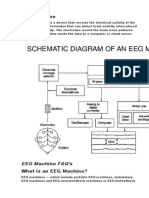
- EEG MachineDocumento3 pagineEEG MachineOlea ScorpanNessuna valutazione finora
- Neural Basis of ConsciousnessDocumento13 pagineNeural Basis of ConsciousnessAlejandro León100% (1)
- Brain and Neural NetworksDocumento17 pagineBrain and Neural NetworksKristyle BalagosaNessuna valutazione finora
- Laserneedle-Acupuncture Science and Practice GerhaDocumento2 pagineLaserneedle-Acupuncture Science and Practice GerhaBeaNessuna valutazione finora
- Introduction To Psychology (Psych 10) Professor Keith HolyoakDocumento60 pagineIntroduction To Psychology (Psych 10) Professor Keith HolyoakRosalind W. WongNessuna valutazione finora
- Adding Intelligence To Internet, The Global Brain: 1) IntroductionDocumento7 pagineAdding Intelligence To Internet, The Global Brain: 1) IntroductionSimmi JoshiNessuna valutazione finora
- Treatment of Facial Pain With I Ching Ba PDFDocumento6 pagineTreatment of Facial Pain With I Ching Ba PDFrendao100% (1)
- Brain Music System Assisted Living FinalDocumento4 pagineBrain Music System Assisted Living Finaladrian_attard_trevisanNessuna valutazione finora
- Drugs and Tinnitus - Neil Bauman PHD - April '09Documento2 pagineDrugs and Tinnitus - Neil Bauman PHD - April '09DownTheTheRabbitHole108Nessuna valutazione finora
- Chapter 3-1-15Documento11 pagineChapter 3-1-15Winda AnnishaNessuna valutazione finora
- When Medicine Took An Alternative Path: History of Medicine in ChinaDocumento6 pagineWhen Medicine Took An Alternative Path: History of Medicine in ChinaKrlos Patiño SierraNessuna valutazione finora
- Visible Body 3d Human Anatomy Atlas MacDocumento1 paginaVisible Body 3d Human Anatomy Atlas MacteamrawajituNessuna valutazione finora
- Kevin Chen - Book Review: Scientific Qigong Exploration: The Wonders and Mysteries of Qi by Lu, ZuyinDocumento6 pagineKevin Chen - Book Review: Scientific Qigong Exploration: The Wonders and Mysteries of Qi by Lu, ZuyinSonyRedNessuna valutazione finora
- 1.7 Introduction To Neuroanatomy PDFDocumento80 pagine1.7 Introduction To Neuroanatomy PDFCarina SuarezNessuna valutazione finora
- AMS CEPES-Laser Documentation ExperiencesDocumento27 pagineAMS CEPES-Laser Documentation ExperiencesmichNessuna valutazione finora
- Ingber Lecture: From Cellular Mechanotransduction To Biologically Inspired EngineeringDocumento14 pagineIngber Lecture: From Cellular Mechanotransduction To Biologically Inspired EngineeringTensegrity Wiki100% (2)
- Wisdom of The AncientsDocumento5 pagineWisdom of The AncientsPreeti Rekha Vijay SurveNessuna valutazione finora
- Crude DrugsDocumento44 pagineCrude DrugsShruti RajNessuna valutazione finora
- Bioelectromagnetics Volume 17 Joseph L. Kirschvink - Microwave Absorption by Magnetite - A Possible Mechanism For Coupling NoDocumento8 pagineBioelectromagnetics Volume 17 Joseph L. Kirschvink - Microwave Absorption by Magnetite - A Possible Mechanism For Coupling NoJose SygNessuna valutazione finora
- Brain Fitness For Positive AgingDocumento65 pagineBrain Fitness For Positive AgingMary GomezNessuna valutazione finora
- Field RNG Exploration: M. Jackson Memorial (2009)Documento6 pagineField RNG Exploration: M. Jackson Memorial (2009)Bryan J WilliamsNessuna valutazione finora
- Ramachandran, Neuroscience, The New PhilosophyDocumento15 pagineRamachandran, Neuroscience, The New PhilosophyAnonymous pgWs18GDG1Nessuna valutazione finora
- Self Cingulo PosteriorDocumento7 pagineSelf Cingulo PosteriorJose ZapataNessuna valutazione finora
- (Re-) Mapping The Concept of DreamingDocumento5 pagine(Re-) Mapping The Concept of DreamingEduardo VLNessuna valutazione finora
- Biochemical and Pharmacological Roles of Adenosylmethionine and the Central Nervous System: Proceedings of an International Round Table on Adenosylmethionine and the Central Nervous System, Naples, Italy, May 1978Da EverandBiochemical and Pharmacological Roles of Adenosylmethionine and the Central Nervous System: Proceedings of an International Round Table on Adenosylmethionine and the Central Nervous System, Naples, Italy, May 1978Vincenzo ZappiaNessuna valutazione finora
- Physiology & Behavior: Tong Wang, Cun-Zhi Liu, Jian-Chun Yu, Wen Jiang, Jing-Xian HanDocumento7 paginePhysiology & Behavior: Tong Wang, Cun-Zhi Liu, Jian-Chun Yu, Wen Jiang, Jing-Xian Handouglasvargas-1Nessuna valutazione finora
- Acupuncture Regulates The Aging-Related Changes in Gene Pro Le Expression of The Hippocampus in Senescence-Accelerated Mouse (SAMP10)Documento6 pagineAcupuncture Regulates The Aging-Related Changes in Gene Pro Le Expression of The Hippocampus in Senescence-Accelerated Mouse (SAMP10)douglasvargas-1Nessuna valutazione finora
- Historia MTCHDocumento62 pagineHistoria MTCHdouglasvargas-1Nessuna valutazione finora
- Historia MTCHDocumento31 pagineHistoria MTCHdouglasvargas-1Nessuna valutazione finora
- Vih PDFDocumento10 pagineVih PDFdouglasvargas-1Nessuna valutazione finora
- Fitri PunyaDocumento351 pagineFitri PunyaFajar LestariNessuna valutazione finora
- Neurobiology of The Neuron and The NeurogliaDocumento6 pagineNeurobiology of The Neuron and The NeurogliaBarney CordovaNessuna valutazione finora
- Development of Nervous SystemDocumento59 pagineDevelopment of Nervous SystemtuhinNessuna valutazione finora
- Thermal Conductivity Data For Different TissuesDocumento14 pagineThermal Conductivity Data For Different TissuesZuneid AlamNessuna valutazione finora
- Atrophy of The Parietal Lobe in Preclinical DementiaDocumento10 pagineAtrophy of The Parietal Lobe in Preclinical DementiaNícolas CavalcanteNessuna valutazione finora
- ICSE Class 8 Biology Selina Solution Chapter 7 The Nervous SystemDocumento7 pagineICSE Class 8 Biology Selina Solution Chapter 7 The Nervous Systemarshadff890Nessuna valutazione finora
- Central Nervous SystemDocumento1 paginaCentral Nervous Systemlez2Nessuna valutazione finora
- Chapter 6 QuestionsDocumento2 pagineChapter 6 QuestionsGabo DanteNessuna valutazione finora
- The Structure & Functioning of The Nervous SystemDocumento177 pagineThe Structure & Functioning of The Nervous SystemISHITA GOEL 19224115Nessuna valutazione finora
- Types of NeuronsDocumento10 pagineTypes of NeuronsJaspherBalderaNessuna valutazione finora
- CVD Infarct 1Documento92 pagineCVD Infarct 1JohnMichaelDominguezNessuna valutazione finora
- Aphasia TableDocumento2 pagineAphasia Tablelakshmi priyaNessuna valutazione finora
- Central Nervous System - Brain and Spinal CordDocumento8 pagineCentral Nervous System - Brain and Spinal CordArrianne Sjairra PimentelNessuna valutazione finora
- 7 0 Student WorkbookDocumento17 pagine7 0 Student Workbookapi-343368893Nessuna valutazione finora
- COPIC Color ChartDocumento1 paginaCOPIC Color ChartEstephani Cal DerNessuna valutazione finora
- Shaywitz 1998Documento6 pagineShaywitz 1998jorgedacunhaNessuna valutazione finora
- Case Study Ucmed 6TH FloorDocumento44 pagineCase Study Ucmed 6TH FloorPasay Trisha Faye Y.Nessuna valutazione finora
- Aspects of Personal Dev. ModuleDocumento83 pagineAspects of Personal Dev. ModuleAlice BienvinutoNessuna valutazione finora
- Name: - Section: - : Personal Development Quarter 4 - Week 1 & 2 The Power of MindDocumento7 pagineName: - Section: - : Personal Development Quarter 4 - Week 1 & 2 The Power of MindMatt Gabriel LacierdaNessuna valutazione finora
- The Powers of The Mind Perdev ReportDocumento2 pagineThe Powers of The Mind Perdev ReportUelNessuna valutazione finora
- DiensefalonDocumento31 pagineDiensefalonIngrid AykeNessuna valutazione finora
- 2011 @radproflib D Karthikeyan Step PDFDocumento310 pagine2011 @radproflib D Karthikeyan Step PDFToma BichirNessuna valutazione finora
- The What and How of Prefrontal Cortical Organization: Randall C. O'ReillyDocumento7 pagineThe What and How of Prefrontal Cortical Organization: Randall C. O'ReillyAvengingBrainNessuna valutazione finora
- Characterizing The Subtype of Anhedonia in Major Depressive DisorderDocumento9 pagineCharacterizing The Subtype of Anhedonia in Major Depressive DisorderGkani ChrysoulaNessuna valutazione finora
- Virtual Brain DissectionDocumento15 pagineVirtual Brain DissectionJill KoehlerNessuna valutazione finora
- Human BrainDocumento45 pagineHuman BrainNirmal BhowmickNessuna valutazione finora
- 208-Broca's Region-Yosef Grodzinsky, Katrin Amunts-0195177649-Oxford University Press, USA-2006-4 PDFDocumento436 pagine208-Broca's Region-Yosef Grodzinsky, Katrin Amunts-0195177649-Oxford University Press, USA-2006-4 PDFMedved BozanaNessuna valutazione finora
- Brain Encephalon: - Brain: Embrionally Comes From Ectoderm PartDocumento72 pagineBrain Encephalon: - Brain: Embrionally Comes From Ectoderm PartHana AdivaNessuna valutazione finora
- 10-20 System (EEG) - Wikipedia, The Free EncyclopediaDocumento2 pagine10-20 System (EEG) - Wikipedia, The Free EncyclopediaDuncan WilliamsNessuna valutazione finora
- Neurobiology of Emotions: An Update: International Review of PsychiatryDocumento16 pagineNeurobiology of Emotions: An Update: International Review of PsychiatryEva Bastida MercadoNessuna valutazione finora