Potrebbero piacerti anche
- Daftar Obat Puskesmas KanjiloDocumento2 pagineDaftar Obat Puskesmas KanjiloAhmad SalimNessuna valutazione finora
- Guia Practica Fa 2016Documento90 pagineGuia Practica Fa 2016Juan Carlos SuarezNessuna valutazione finora
- Kon SensusDocumento10 pagineKon SensusAhmad SalimNessuna valutazione finora
- Kon SensusDocumento10 pagineKon SensusAhmad SalimNessuna valutazione finora
- Komodo DragonDocumento3 pagineKomodo DragonAhmad SalimNessuna valutazione finora
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5783)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (72)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (119)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- School Development Plan 2022Documento3 pagineSchool Development Plan 2022Nora Herrera100% (6)
- Design Proposal For North Public & Suite Areas Decorative Lighting, Solaire Quezon CityDocumento42 pagineDesign Proposal For North Public & Suite Areas Decorative Lighting, Solaire Quezon CityRichard Libunao BelduaNessuna valutazione finora
- 1 Osteology (MCQ)Documento12 pagine1 Osteology (MCQ)Utkarsh MishraNessuna valutazione finora
- Currency Exchnage FormatDocumento1 paginaCurrency Exchnage FormatSarvjeet SinghNessuna valutazione finora
- Dimensions of Comparative EducationDocumento5 pagineDimensions of Comparative Educationeminentsurvivor9Nessuna valutazione finora
- Module 3 FP Client AssessmentDocumento54 pagineModule 3 FP Client AssessmentJhunna TalanganNessuna valutazione finora
- Tax Invoice: New No 30, Old No 24 Bhagirathi Ammal ST, T Nagar, Chennai 600017 CIN: U74900TN2011PTC083121 State Code: 33Documento1 paginaTax Invoice: New No 30, Old No 24 Bhagirathi Ammal ST, T Nagar, Chennai 600017 CIN: U74900TN2011PTC083121 State Code: 33golu84Nessuna valutazione finora
- Sciencedirect Sciencedirect SciencedirectDocumento7 pagineSciencedirect Sciencedirect SciencedirectMohamed Amine NZNessuna valutazione finora
- Bleed Fan SelectionDocumento4 pagineBleed Fan Selectionomar abdullahNessuna valutazione finora
- Imaging With FTK ImagerDocumento9 pagineImaging With FTK ImagerRobert LeighNessuna valutazione finora
- Lembar Kerja Lap Keu - Tahap 1Documento4 pagineLembar Kerja Lap Keu - Tahap 1Safana AuraNessuna valutazione finora
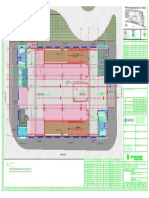
- Key plan and area statement comparison for multi-level car park (MLCPDocumento1 paginaKey plan and area statement comparison for multi-level car park (MLCP121715502003 BOLLEMPALLI BINDU SREE SATYANessuna valutazione finora
- C15 DiagranmaDocumento2 pagineC15 Diagranmajose manuel100% (1)
- Astm 630Documento3 pagineAstm 630InfoNessuna valutazione finora
- Ball Bearings 1Documento17 pagineBall Bearings 1ManicharanNessuna valutazione finora
- 7-Seater MPV: Kia SingaporeDocumento16 pagine7-Seater MPV: Kia SingaporeadiNessuna valutazione finora
- Underground Water Tanks Cleaning ScopeDocumento2 pagineUnderground Water Tanks Cleaning ScopeOsama AhmedNessuna valutazione finora
- Easa Ad 2023-0133 1Documento6 pagineEasa Ad 2023-0133 1Pedro LucasNessuna valutazione finora
- Adoption ApplicationDocumento3 pagineAdoption ApplicationwriterhildNessuna valutazione finora
- MGN 363Documento14 pagineMGN 363Nitin PatidarNessuna valutazione finora
- 150 C++ BitsDocumento55 pagine150 C++ BitsRavi Varma D V SNessuna valutazione finora
- BL ListDocumento8 pagineBL ListStraña Abigail Alonsabe Villacis100% (1)
- Eslit-Vinea-LA 03 Task #1-4Documento11 pagineEslit-Vinea-LA 03 Task #1-4darkNessuna valutazione finora
- Noor Hafifi Bin Jalal: Operating Code 1: Demand ForecastDocumento47 pagineNoor Hafifi Bin Jalal: Operating Code 1: Demand ForecastGopalakrishnan SekharanNessuna valutazione finora
- Ec010 505 Applied Electromagnetic TheoryDocumento2 pagineEc010 505 Applied Electromagnetic Theorywalternampimadom100% (1)
- Appeal Tax Procedure (Malaysia)Documento2 pagineAppeal Tax Procedure (Malaysia)Zati TyNessuna valutazione finora
- Examen 03 Aula - F PostgradoDocumento5 pagineExamen 03 Aula - F PostgradodiegoNessuna valutazione finora
- Keyence cv700 - Man2Documento232 pagineKeyence cv700 - Man2kamaleon85Nessuna valutazione finora
- List of RelaysDocumento26 pagineList of RelaysadhyarthaNessuna valutazione finora
- Vào 10 - Sở L NG Sơn 2022-2023Documento5 pagineVào 10 - Sở L NG Sơn 2022-2023Lan HuongNessuna valutazione finora