Potrebbero piacerti anche
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (74)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- Health Insurance in Switzerland ETHDocumento57 pagineHealth Insurance in Switzerland ETHguzman87Nessuna valutazione finora
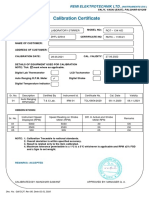
- Calibration CertificateDocumento1 paginaCalibration CertificateSales GoldClassNessuna valutazione finora
- Enerparc - India - Company Profile - September 23Documento15 pagineEnerparc - India - Company Profile - September 23AlokNessuna valutazione finora
- Fernando Salgado-Hernandez, A206 263 000 (BIA June 7, 2016)Documento7 pagineFernando Salgado-Hernandez, A206 263 000 (BIA June 7, 2016)Immigrant & Refugee Appellate Center, LLCNessuna valutazione finora
- Brochure Ref 670Documento4 pagineBrochure Ref 670veerabossNessuna valutazione finora
- What Caused The Slave Trade Ruth LingardDocumento17 pagineWhat Caused The Slave Trade Ruth LingardmahaNessuna valutazione finora
- Hayashi Q Econometica 82Documento16 pagineHayashi Q Econometica 82Franco VenesiaNessuna valutazione finora
- 18 - PPAG-100-HD-C-001 - s018 (VBA03C013) - 0 PDFDocumento1 pagina18 - PPAG-100-HD-C-001 - s018 (VBA03C013) - 0 PDFSantiago GarciaNessuna valutazione finora
- Dissertation On Indian Constitutional LawDocumento6 pagineDissertation On Indian Constitutional LawCustomPaperWritingAnnArbor100% (1)
- Recommended Practices For Developing An Industrial Control Systems Cybersecurity Incident Response CapabilityDocumento49 pagineRecommended Practices For Developing An Industrial Control Systems Cybersecurity Incident Response CapabilityJohn DavisonNessuna valutazione finora
- Notifier AMPS 24 AMPS 24E Addressable Power SupplyDocumento44 pagineNotifier AMPS 24 AMPS 24E Addressable Power SupplyMiguel Angel Guzman ReyesNessuna valutazione finora
- P394 WindActions PDFDocumento32 pagineP394 WindActions PDFzhiyiseowNessuna valutazione finora
- DesalinationDocumento4 pagineDesalinationsivasu1980aNessuna valutazione finora
- Income Statement, Its Elements, Usefulness and LimitationsDocumento5 pagineIncome Statement, Its Elements, Usefulness and LimitationsDipika tasfannum salamNessuna valutazione finora
- SEERS Medical ST3566 ManualDocumento24 pagineSEERS Medical ST3566 ManualAlexandra JanicNessuna valutazione finora
- Privacy: Based On Slides Prepared by Cyndi Chie, Sarah Frye and Sharon Gray. Fifth Edition Updated by Timothy HenryDocumento50 paginePrivacy: Based On Slides Prepared by Cyndi Chie, Sarah Frye and Sharon Gray. Fifth Edition Updated by Timothy HenryAbid KhanNessuna valutazione finora
- Introduction To Motor DrivesDocumento24 pagineIntroduction To Motor Drivessukhbat sodnomdorjNessuna valutazione finora
- G.R. No. 185449, November 12, 2014 Del Castillo Digest By: DOLARDocumento2 pagineG.R. No. 185449, November 12, 2014 Del Castillo Digest By: DOLARTheodore DolarNessuna valutazione finora
- PLT Lecture NotesDocumento5 paginePLT Lecture NotesRamzi AbdochNessuna valutazione finora
- Resume Jameel 22Documento3 pagineResume Jameel 22sandeep sandyNessuna valutazione finora
- 3412C EMCP II For PEEC Engines Electrical System: Ac Panel DC PanelDocumento4 pagine3412C EMCP II For PEEC Engines Electrical System: Ac Panel DC PanelFrancisco Wilson Bezerra FranciscoNessuna valutazione finora
- Amerisolar AS 7M144 HC Module Specification - CompressedDocumento2 pagineAmerisolar AS 7M144 HC Module Specification - CompressedMarcus AlbaniNessuna valutazione finora
- Extent of The Use of Instructional Materials in The Effective Teaching and Learning of Home Home EconomicsDocumento47 pagineExtent of The Use of Instructional Materials in The Effective Teaching and Learning of Home Home Economicschukwu solomon75% (4)
- Ikea AnalysisDocumento33 pagineIkea AnalysisVinod BridglalsinghNessuna valutazione finora
- Business Environment Analysis - Saudi ArabiaDocumento24 pagineBusiness Environment Analysis - Saudi ArabiaAmlan JenaNessuna valutazione finora
- Sample Annual BudgetDocumento4 pagineSample Annual BudgetMary Ann B. GabucanNessuna valutazione finora
- TSB 120Documento7 pagineTSB 120patelpiyushbNessuna valutazione finora
- Lab Session 7: Load Flow Analysis Ofa Power System Using Gauss Seidel Method in MatlabDocumento7 pagineLab Session 7: Load Flow Analysis Ofa Power System Using Gauss Seidel Method in MatlabHayat AnsariNessuna valutazione finora
- Cic Tips Part 1&2Documento27 pagineCic Tips Part 1&2Yousef AlalawiNessuna valutazione finora
- PeopleSoft Application Engine Program PDFDocumento17 paginePeopleSoft Application Engine Program PDFSaurabh MehtaNessuna valutazione finora