Potrebbero piacerti anche
- Treatment and Rehabilitation Center-CARAGA: EmailDocumento1 paginaTreatment and Rehabilitation Center-CARAGA: Emaildanny17phNessuna valutazione finora
- How To Make Homemade Ice CreamDocumento5 pagineHow To Make Homemade Ice Creamdanny17phNessuna valutazione finora
- Rehab in The Time of Drug WarDocumento5 pagineRehab in The Time of Drug Wardanny17phNessuna valutazione finora
- Philippine Eagles HymnDocumento2 paginePhilippine Eagles Hymndanny17ph100% (8)
- Molave Hotel: Carlitos HostelDocumento2 pagineMolave Hotel: Carlitos Hosteldanny17phNessuna valutazione finora
- While in ChinaDocumento1 paginaWhile in Chinadanny17phNessuna valutazione finora
- The Ongoing Evolution of Rotaract Is Redefining Its Place Within RotaryDocumento6 pagineThe Ongoing Evolution of Rotaract Is Redefining Its Place Within Rotarydanny17phNessuna valutazione finora
- Bond Investing Guide 1 To 3Documento4 pagineBond Investing Guide 1 To 3danny17phNessuna valutazione finora
- Primary Care Approach To ProteinuriaDocumento6 paginePrimary Care Approach To Proteinuriadanny17phNessuna valutazione finora
- Diagnosis and Management of Bacterial Meningitis in The Pediatric PopulationDocumento8 pagineDiagnosis and Management of Bacterial Meningitis in The Pediatric Populationdanny17phNessuna valutazione finora
- The Emergency Management and Treatment of Severe BurnsDocumento5 pagineThe Emergency Management and Treatment of Severe Burnsdanny17phNessuna valutazione finora
- Care of The Critically Ill Emergency Department Patient With Acute Kidney InjuryDocumento6 pagineCare of The Critically Ill Emergency Department Patient With Acute Kidney Injurydanny17phNessuna valutazione finora
- JFP - GrandRounds Red Eye, Blurry Vision and CoughDocumento3 pagineJFP - GrandRounds Red Eye, Blurry Vision and Coughdanny17phNessuna valutazione finora
- "Basal Cell Blanche" - A Diagnostic Maneuver To Increase Early Detection of Basal Cell CarcinomasDocumento3 pagine"Basal Cell Blanche" - A Diagnostic Maneuver To Increase Early Detection of Basal Cell Carcinomasdanny17phNessuna valutazione finora
- How Should We Manage An Acute Exacerbation of COPDDocumento3 pagineHow Should We Manage An Acute Exacerbation of COPDdanny17phNessuna valutazione finora
- How Should We Care For Atopic DermatitisDocumento2 pagineHow Should We Care For Atopic Dermatitisdanny17phNessuna valutazione finora
- JFP - GrandRounds Red Eye, Blurry Vision and CoughDocumento5 pagineJFP - GrandRounds Red Eye, Blurry Vision and Coughdanny17phNessuna valutazione finora
- Revisiting Spirometry in The Diagnosis of COPD PDFDocumento1 paginaRevisiting Spirometry in The Diagnosis of COPD PDFdanny17phNessuna valutazione finora
- Neck Mass How Would You TreatDocumento5 pagineNeck Mass How Would You Treatdanny17phNessuna valutazione finora
- Fever, Rash, and Peeling SkinDocumento4 pagineFever, Rash, and Peeling Skindanny17phNessuna valutazione finora
- How Should We Diagnose and Treat Osteoarthritis of The KneeDocumento3 pagineHow Should We Diagnose and Treat Osteoarthritis of The Kneedanny17phNessuna valutazione finora
- How Should We Diagnose and Treat Obstructive Sleep ApneaDocumento2 pagineHow Should We Diagnose and Treat Obstructive Sleep Apneadanny17phNessuna valutazione finora
- Hormone Replacement Therapy The Right Choice For Your PatientDocumento9 pagineHormone Replacement Therapy The Right Choice For Your Patientdanny17phNessuna valutazione finora
- How Should We Evaluate Constipation in Infants and ChildrenDocumento3 pagineHow Should We Evaluate Constipation in Infants and Childrendanny17phNessuna valutazione finora
- Diff Use Abdominal Pain, VomitingDocumento4 pagineDiff Use Abdominal Pain, Vomitingdanny17phNessuna valutazione finora
- Neck Mass How Would You TreatDocumento5 pagineNeck Mass How Would You Treatdanny17phNessuna valutazione finora
- How Should We Evaluate Constipation in Infants and ChildrenDocumento2 pagineHow Should We Evaluate Constipation in Infants and Childrendanny17phNessuna valutazione finora
- Diabetic Foot Ulcer and Poor Compliance How Would You TreatDocumento9 pagineDiabetic Foot Ulcer and Poor Compliance How Would You Treatdanny17phNessuna valutazione finora
- Dyspnea, PancytopeniaDocumento4 pagineDyspnea, Pancytopeniadanny17phNessuna valutazione finora
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (73)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- Causes of Ischemic Stroke: October 2010Documento19 pagineCauses of Ischemic Stroke: October 2010Pajokka 10Nessuna valutazione finora
- Acute Renal FailureDocumento33 pagineAcute Renal FailureAqsa Akbar AliNessuna valutazione finora
- Updated How To Deal ACS in Limited Resources Facilities - Danie Syahrir, DR., SP - JPDocumento32 pagineUpdated How To Deal ACS in Limited Resources Facilities - Danie Syahrir, DR., SP - JPmaria sintaNessuna valutazione finora
- Anterior Triangle of NeckDocumento13 pagineAnterior Triangle of NeckÑäd ÉèmNessuna valutazione finora
- Drug Study: Patient: B.V Age: 58y/oDocumento2 pagineDrug Study: Patient: B.V Age: 58y/oAndrea Sibayan SorianoNessuna valutazione finora
- Xeljanz Initiation ChecklistDocumento8 pagineXeljanz Initiation ChecklistRawan ZayedNessuna valutazione finora
- Duty Report: March 24 2021Documento54 pagineDuty Report: March 24 2021Abi ArifiNessuna valutazione finora
- Gynecology: 3.09 - AmenorrheaDocumento13 pagineGynecology: 3.09 - AmenorrheaAnna Mae MarantanNessuna valutazione finora
- Mksap PulmonaryDocumento77 pagineMksap PulmonaryAna Roman100% (4)
- Guillain Barre Syndrome: M.Widiastuti Samekto Fak - Kedokteran UndipDocumento30 pagineGuillain Barre Syndrome: M.Widiastuti Samekto Fak - Kedokteran UndipDani Yustiardi Munarso100% (1)
- Febrile Convulsion & EpilepsyDocumento17 pagineFebrile Convulsion & EpilepsyprajwalNessuna valutazione finora
- March 7 2013 Mount Ayr Record-NewsDocumento14 pagineMarch 7 2013 Mount Ayr Record-NewsMountAyrRecordNewsNessuna valutazione finora
- Precocious PubertyDocumento13 paginePrecocious PubertyLee Woan ChyiNessuna valutazione finora
- Cirrhosis AndrewDocumento33 pagineCirrhosis Andrewlionel andreaNessuna valutazione finora
- A Clinical Vignette On Raoultella Planticola BacteremiaDocumento5 pagineA Clinical Vignette On Raoultella Planticola BacteremiaJamie FleetNessuna valutazione finora
- Cases Journal: Acquired Nonobstructive Urinary Bladder Diverticulum: A CaseDocumento3 pagineCases Journal: Acquired Nonobstructive Urinary Bladder Diverticulum: A CaseIrma Suriani DarwisNessuna valutazione finora
- Student - Surgery - August 27 PDFDocumento242 pagineStudent - Surgery - August 27 PDFAselian BenedictorNessuna valutazione finora
- A 68-Year-Old Man With Swollen Legs: Exemplary CBCR Case 2Documento14 pagineA 68-Year-Old Man With Swollen Legs: Exemplary CBCR Case 2nadim13Nessuna valutazione finora
- Neuro UrologyDocumento53 pagineNeuro UrologymoominjunaidNessuna valutazione finora
- 2.D17 419 Kastriot Meqa Agim BegzatiDocumento6 pagine2.D17 419 Kastriot Meqa Agim BegzatiAndi Ndaru WNessuna valutazione finora
- Fecal IncontinenceDocumento25 pagineFecal IncontinenceBinita ShresthaNessuna valutazione finora
- GBS MCQDocumento6 pagineGBS MCQMoonNessuna valutazione finora
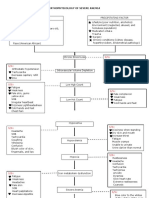
- Pathophysiology of Severe AnemiaDocumento3 paginePathophysiology of Severe AnemiaChrizley Shawn DeroniaNessuna valutazione finora
- Bipolar Disorders and Carbamazepine PharmacokinetiDocumento5 pagineBipolar Disorders and Carbamazepine PharmacokinetiAgr YuroNessuna valutazione finora
- The Medical Management of Abnormal Uterine Bleeding in Reproductive-Aged WomenDocumento14 pagineThe Medical Management of Abnormal Uterine Bleeding in Reproductive-Aged Womendiegoesteban1234Nessuna valutazione finora
- Shin LuluDocumento2 pagineShin LuluEka HimawanNessuna valutazione finora
- 01 Admission Discharge Criteria and TriageDocumento5 pagine01 Admission Discharge Criteria and TriageSuhasani JainNessuna valutazione finora
- Hyperglycemia in Pregnant Ladies and Its Outcome Out in The Opd, Labor Ward, Gynecology and Obstetrics, Lady Atichison Hospital, LahoreDocumento7 pagineHyperglycemia in Pregnant Ladies and Its Outcome Out in The Opd, Labor Ward, Gynecology and Obstetrics, Lady Atichison Hospital, LahoreiajpsNessuna valutazione finora
- Paces Guide 2012 From Online NotesDocumento228 paginePaces Guide 2012 From Online NotesThistell ThistleNessuna valutazione finora
- Neurophysiology: Understanding How The Nervous System WorksDocumento72 pagineNeurophysiology: Understanding How The Nervous System WorkshardianNessuna valutazione finora