Potrebbero piacerti anche
- Intrapartum AssessmentDocumento84 pagineIntrapartum AssessmentAnne Carlie Bucoy RoldanNessuna valutazione finora
- EXTERNAL FETAL MONITORING (NON - INVASIVE) (Autosaved)Documento54 pagineEXTERNAL FETAL MONITORING (NON - INVASIVE) (Autosaved)Maria Pina Barbado PonceNessuna valutazione finora
- Worksheet To Accompany FHR Review Video: Emerald Spangler May 6, 2021Documento3 pagineWorksheet To Accompany FHR Review Video: Emerald Spangler May 6, 2021Emerald SpanglerNessuna valutazione finora
- Assessment of Fetal Well BeingDocumento61 pagineAssessment of Fetal Well Beingsana khan008Nessuna valutazione finora
- Fetal Monitoring: Condition Causes GradeDocumento6 pagineFetal Monitoring: Condition Causes GradeSachin SinghNessuna valutazione finora
- Criteria of Normal Fetal Heart Rate (FHR)Documento14 pagineCriteria of Normal Fetal Heart Rate (FHR)عمر احمد شاكرNessuna valutazione finora
- CTGDocumento38 pagineCTGfahmiNessuna valutazione finora
- Intrapartum Fetal SurveillanceDocumento59 pagineIntrapartum Fetal SurveillanceGaylinel BongyadNessuna valutazione finora
- Intrapartum Fetal Monitoring EditedDocumento51 pagineIntrapartum Fetal Monitoring EditedObgyn DischargesNessuna valutazione finora
- CTG Interpretation: Dr. Areen AlnasanDocumento37 pagineCTG Interpretation: Dr. Areen AlnasanMohammad AlrefaiNessuna valutazione finora
- CARDIOTOCOGRAPHYDocumento5 pagineCARDIOTOCOGRAPHYPadma100% (1)
- Fetal Monitoring BasicsDocumento25 pagineFetal Monitoring BasicsKaren HutchinsonNessuna valutazione finora
- Fetal DistressDocumento65 pagineFetal DistressEdward OledanNessuna valutazione finora
- CTG Interpretation 1Documento27 pagineCTG Interpretation 1asri khazaliNessuna valutazione finora
- Intrapartum Fetal AssessmentDocumento52 pagineIntrapartum Fetal AssessmentAditya TejabaswaraNessuna valutazione finora
- Electronic Fetal MonitoringDocumento4 pagineElectronic Fetal MonitoringMauZungNessuna valutazione finora
- KTG MTGDocumento29 pagineKTG MTGArina fauziyantyNessuna valutazione finora
- How To Read A CTGDocumento31 pagineHow To Read A CTGAbdullah As'ad100% (1)
- Pregnancy Induced Hypertension PihDocumento17 paginePregnancy Induced Hypertension PihRose DeymNessuna valutazione finora
- I. Intrapartum Electronic Fetal Monitoring: Ob Rotation OsceDocumento24 pagineI. Intrapartum Electronic Fetal Monitoring: Ob Rotation OsceAngelie Therese ChuaNessuna valutazione finora
- CTG AryaDocumento39 pagineCTG AryaSucor PandeNessuna valutazione finora
- Introduction (Final)Documento11 pagineIntroduction (Final)Pureza Maye SalapangNessuna valutazione finora
- Fetal Heart TonesDocumento1 paginaFetal Heart TonesChristian Clyde N. JakosalemNessuna valutazione finora
- Intrapartum Fetal Monitoring TechniquesDocumento51 pagineIntrapartum Fetal Monitoring TechniquesticticNessuna valutazione finora
- CTG ReportingDocumento57 pagineCTG ReportingALIMBOYOGUEN RexorNessuna valutazione finora
- Fetal SurveillanceDocumento5 pagineFetal SurveillanceĶHwola ƏľsHokryNessuna valutazione finora
- OBGYN Objective - Module Study GuideDocumento79 pagineOBGYN Objective - Module Study GuideHema LaughsalotNessuna valutazione finora
- Intrapartum Fetal Assessment TechniquesDocumento80 pagineIntrapartum Fetal Assessment Techniqueszgra666Nessuna valutazione finora
- EFM Teaching Didactic FINALDocumento81 pagineEFM Teaching Didactic FINALNadia RestyNessuna valutazione finora
- Intrapartum Fetal MonitoringDocumento15 pagineIntrapartum Fetal MonitoringAnuradha Maurya100% (1)
- Understanding Pregnancy and Pregnancy-Related ConditionsDocumento77 pagineUnderstanding Pregnancy and Pregnancy-Related ConditionsPureza Maye SalapangNessuna valutazione finora
- Abnormal Cardiotocography - "CTG"Documento47 pagineAbnormal Cardiotocography - "CTG"Ahmad Mustaqim SulaimanNessuna valutazione finora
- Assessment of Fetal WellbeingDocumento71 pagineAssessment of Fetal WellbeingDanny Apw100% (2)
- FHR Strip Interpretation GuideDocumento2 pagineFHR Strip Interpretation GuidemunkeeluvdesignsNessuna valutazione finora
- Non Stress Test 1Documento8 pagineNon Stress Test 1Ala'a Emerald AguamNessuna valutazione finora
- OB - Hypertensive Disorders in PregnancyDocumento6 pagineOB - Hypertensive Disorders in PregnancyM MNessuna valutazione finora
- Saint Gabriel General Hospital: Root Cause Analysis IfudDocumento14 pagineSaint Gabriel General Hospital: Root Cause Analysis IfuddawitNessuna valutazione finora
- Hypertension in Pregnancy: Understanding and Managing RisksDocumento69 pagineHypertension in Pregnancy: Understanding and Managing RisksNatif BoteNessuna valutazione finora
- Pcol Cover To CoverDocumento214 paginePcol Cover To CoverJec OcampoNessuna valutazione finora
- Neonatology Document on Prematurity ComplicationsDocumento22 pagineNeonatology Document on Prematurity Complicationsipad jojNessuna valutazione finora
- PIH Preeclampsia and EclampsiaDocumento13 paginePIH Preeclampsia and EclampsiaRisqi YuliNessuna valutazione finora
- CTG Interpretation CmeDocumento32 pagineCTG Interpretation CmeNurshawina KamaludinNessuna valutazione finora
- CTG - Koass 09 Jan 2023Documento35 pagineCTG - Koass 09 Jan 2023Artiana RahmadiniNessuna valutazione finora
- OxytocinDocumento1 paginaOxytocinnylix23Nessuna valutazione finora
- EFM: Interpreting Fetal Heart Rate TracingsDocumento45 pagineEFM: Interpreting Fetal Heart Rate TracingsMadhu Sudhan PandeyaNessuna valutazione finora
- Neonatal Respiratory Distress: Causes, Signs, and ManagementDocumento21 pagineNeonatal Respiratory Distress: Causes, Signs, and ManagementtyapalupiNessuna valutazione finora
- Fetal DistressDocumento3 pagineFetal DistressMaria Donabella OngueNessuna valutazione finora
- Increased Intracranial Pressure and Seizure Feb 14Documento2 pagineIncreased Intracranial Pressure and Seizure Feb 14anime listNessuna valutazione finora
- Anestesi pada ObstetriDocumento20 pagineAnestesi pada ObstetriTri Ari dityaNessuna valutazione finora
- Fetal Assessment During LaborDocumento3 pagineFetal Assessment During LaborMariya ZafraniNessuna valutazione finora
- How To Read A CTGDocumento11 pagineHow To Read A CTGiwennieNessuna valutazione finora
- Fetal Heart Rate MonitoringDocumento13 pagineFetal Heart Rate MonitoringNinaSimone17Nessuna valutazione finora
- Reduced Fetal MovementsDocumento9 pagineReduced Fetal MovementsLois KankowskiNessuna valutazione finora
- OB - Hypertensive DisordersDocumento4 pagineOB - Hypertensive DisordersJasmine Nicole RemetreNessuna valutazione finora
- NCM 109 MCN Semifinals Topic 1 PIHDocumento2 pagineNCM 109 MCN Semifinals Topic 1 PIHQUEZON, BRITNEY KIM E.Nessuna valutazione finora
- 13-HTN in PregnancyDocumento71 pagine13-HTN in PregnancybenNessuna valutazione finora
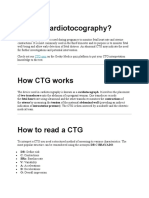
- What Is Cardiotocography?: Cardiotocography (CTG) Is Used During Pregnancy To Monitor Fetal Heart Rate and UterineDocumento18 pagineWhat Is Cardiotocography?: Cardiotocography (CTG) Is Used During Pregnancy To Monitor Fetal Heart Rate and Uterineمحمداحمد محمدنور ابايزيدNessuna valutazione finora
- Intracranial Hypertension or Increased ICPDocumento11 pagineIntracranial Hypertension or Increased ICPRomina Irish MatutinoNessuna valutazione finora
- High Blood Pressure: Natural Self-help for Hypertension, including 60 recipesDa EverandHigh Blood Pressure: Natural Self-help for Hypertension, including 60 recipesNessuna valutazione finora
- Endocrinology Notes for Medical StudentsDa EverandEndocrinology Notes for Medical StudentsValutazione: 4 su 5 stelle4/5 (1)
- Search For The Cleanest and Greenest Brgy GuidelinesDocumento9 pagineSearch For The Cleanest and Greenest Brgy GuidelinesAnonymous elSqPhzKNessuna valutazione finora
- Urinary Tract InfectionsDocumento15 pagineUrinary Tract InfectionsAnonymous elSqPhzKNessuna valutazione finora
- Cardio PicsDocumento5 pagineCardio PicsAnonymous elSqPhzKNessuna valutazione finora
- Adaptations: Causing Increased WorkloadDocumento3 pagineAdaptations: Causing Increased WorkloadAnonymous elSqPhzKNessuna valutazione finora
- Atherosclerosis and Peripheral Vascular DiseaseDocumento1 paginaAtherosclerosis and Peripheral Vascular DiseaseAnonymous elSqPhzKNessuna valutazione finora
- AHA Hypertension Guidelines 2017Documento22 pagineAHA Hypertension Guidelines 2017Anonymous elSqPhzKNessuna valutazione finora
- Prasympathetic: Cholinergic System: Cholinomimetic: You Make Them MoreDocumento1 paginaPrasympathetic: Cholinergic System: Cholinomimetic: You Make Them MoreAnonymous elSqPhzKNessuna valutazione finora
- Prayer Before StudyingDocumento1 paginaPrayer Before StudyingAnonymous elSqPhzKNessuna valutazione finora
- Most Common Pathologies in Gastrointestinal Tract and LiverDocumento6 pagineMost Common Pathologies in Gastrointestinal Tract and LiverBobet ReñaNessuna valutazione finora
- Historyand Physical SampleDocumento5 pagineHistoryand Physical SampleTsukikage12Nessuna valutazione finora
- Atherosclerosis and Peripheral Vascular DiseaseDocumento1 paginaAtherosclerosis and Peripheral Vascular DiseaseAnonymous elSqPhzKNessuna valutazione finora
- Prasympathetic: Cholinergic System: Cholinomimetic: You Make Them MoreDocumento1 paginaPrasympathetic: Cholinergic System: Cholinomimetic: You Make Them MoreAnonymous elSqPhzKNessuna valutazione finora
- Soapwhat To WriteDocumento1 paginaSoapwhat To WriteJoriza TamayoNessuna valutazione finora
- MS3 Survival GuideDocumento50 pagineMS3 Survival Guideprahul2588Nessuna valutazione finora
- Soapwhat To WriteDocumento1 paginaSoapwhat To WriteJoriza TamayoNessuna valutazione finora
- SGD Biochem1Documento6 pagineSGD Biochem1Anonymous elSqPhzKNessuna valutazione finora
- RibsDocumento2 pagineRibsAnonymous elSqPhzKNessuna valutazione finora
- StaphDocumento2 pagineStaphAnonymous elSqPhzKNessuna valutazione finora
- Antimicrobial Drugs 2Documento2 pagineAntimicrobial Drugs 2Anonymous elSqPhzKNessuna valutazione finora
- MedDocumento22 pagineMedAnonymous elSqPhzKNessuna valutazione finora
- Resume - Mendoza, Kaori (Medical Technologist)Documento2 pagineResume - Mendoza, Kaori (Medical Technologist)Anonymous elSqPhzKNessuna valutazione finora
- Antimicrobial Drugs 1Documento2 pagineAntimicrobial Drugs 1Anonymous elSqPhzKNessuna valutazione finora
- Bacterial protein synthesis inhibitors targeting ribosomesDocumento5 pagineBacterial protein synthesis inhibitors targeting ribosomesAnonymous elSqPhzKNessuna valutazione finora
- SGD Biochem1Documento6 pagineSGD Biochem1Anonymous elSqPhzKNessuna valutazione finora
- Reaction Paper: Research MethodsDocumento2 pagineReaction Paper: Research MethodsAnonymous elSqPhzKNessuna valutazione finora
- Hair Transplant Surgery SummaryDocumento2 pagineHair Transplant Surgery SummaryothairclubNessuna valutazione finora
- Clinical TeachingDocumento21 pagineClinical Teachingtanmai nooluNessuna valutazione finora
- Effects of Hand Massage On Anxiety in Cataract Surgery Using Local AnesthesiaDocumento7 pagineEffects of Hand Massage On Anxiety in Cataract Surgery Using Local AnesthesiaJuhendriDwiAGNessuna valutazione finora
- Dhanushiya A-P Saravanan (0359079) Classification of NSAIDsDocumento12 pagineDhanushiya A-P Saravanan (0359079) Classification of NSAIDsaurtho sadaaf sharrarNessuna valutazione finora
- A Client With Osteoarthritis: Nursing Care PlanDocumento1 paginaA Client With Osteoarthritis: Nursing Care PlangeeDeeeeNessuna valutazione finora
- Cardiac Transplantation 2012Documento163 pagineCardiac Transplantation 2012ForonNessuna valutazione finora
- 1A - Discussion ForumDocumento3 pagine1A - Discussion ForumGionne Carlo GomezNessuna valutazione finora
- Ichroma II Test Panels 210331 104829Documento2 pagineIchroma II Test Panels 210331 104829Sinergy DiagnosticNessuna valutazione finora
- Physical Therapy Practice QuestionsDocumento53 paginePhysical Therapy Practice QuestionsJohn Ryan ParisNessuna valutazione finora
- Hemolytic Anemia IIDocumento18 pagineHemolytic Anemia IIrizuka-chanNessuna valutazione finora
- Heart Healthy Patient HandoutsDocumento4 pagineHeart Healthy Patient Handoutsasxi791Nessuna valutazione finora
- Psycopharmacology For PhysicianDocumento2 paginePsycopharmacology For PhysicianSyawal PratamaNessuna valutazione finora
- Amonoo 2019Documento12 pagineAmonoo 2019zozNessuna valutazione finora
- Hospice Social Work - Dona J. ReeseDocumento26 pagineHospice Social Work - Dona J. ReeseColumbia University Press100% (3)
- Anti Psychotic DrugsDocumento2 pagineAnti Psychotic DrugsJohn Corpuz100% (1)
- Essay 1 JPDocumento7 pagineEssay 1 JPapi-640252318Nessuna valutazione finora
- Surat IjinDocumento6 pagineSurat IjinNaeny FajriahNessuna valutazione finora
- Brain-Gut Interactions and Maintenance Factors in Pediatric Gastroenterological Disorders: Recommendations For Clinical CareDocumento13 pagineBrain-Gut Interactions and Maintenance Factors in Pediatric Gastroenterological Disorders: Recommendations For Clinical Carefezia TiffaniNessuna valutazione finora
- Brain InfectionsDocumento18 pagineBrain InfectionsSarah Naura IrbahNessuna valutazione finora
- Anja Ainamo 1992 in His 18 Year Follow Up Study AfterDocumento215 pagineAnja Ainamo 1992 in His 18 Year Follow Up Study AfterSuperna TiwariNessuna valutazione finora
- What Is The Most Important Component of Blood Pressure: Systolic, Diastolic or Pulse Pressure?Documento5 pagineWhat Is The Most Important Component of Blood Pressure: Systolic, Diastolic or Pulse Pressure?Susan SuárezNessuna valutazione finora
- Respon Imunitas Dan Badai Sitokin Severe AcuteDocumento26 pagineRespon Imunitas Dan Badai Sitokin Severe AcuteteguhNessuna valutazione finora
- Spasm OmenDocumento30 pagineSpasm OmenJehanzeb Tariq100% (1)
- JaundiceDocumento2 pagineJaundiceGajanan JagtapNessuna valutazione finora
- CD 34845Documento2 pagineCD 34845ReaMetrix100% (2)
- Drug Study Ceftriaxone SodiumDocumento3 pagineDrug Study Ceftriaxone SodiumPrincess Queenie OlarteNessuna valutazione finora
- Chapter 53: Nursing Management: Sexually Transmitted DiseasesDocumento4 pagineChapter 53: Nursing Management: Sexually Transmitted DiseasesjefrocNessuna valutazione finora
- The Anatomical and Physiological Properties of The SignsDocumento5 pagineThe Anatomical and Physiological Properties of The SignstusharNessuna valutazione finora
- Intravenous Induction AgentsDocumento59 pagineIntravenous Induction Agentsroundnumber100% (1)
- Infectious Bursal Disease: Transmission, Pathogenesis, Pathology and Control - An OverviewDocumento14 pagineInfectious Bursal Disease: Transmission, Pathogenesis, Pathology and Control - An OverviewAfdol StoryNessuna valutazione finora