Potrebbero piacerti anche
- Clinical PelvimetryDocumento3 pagineClinical PelvimetryValerie Gonzaga-Carandang0% (1)
- Med Thics Reporting Group 6Documento14 pagineMed Thics Reporting Group 6Nestley TiongsonNessuna valutazione finora
- Men Don't Love Women Like You - The Brutal Truth About Dating, Relationships, and How To Go From Placeholder To Game ChangerDocumento360 pagineMen Don't Love Women Like You - The Brutal Truth About Dating, Relationships, and How To Go From Placeholder To Game ChangerDiana VuchingerNessuna valutazione finora
- SexologyDocumento91 pagineSexologyGuduna Guduna Darbuashvili100% (1)
- Physiology of LaborDocumento16 paginePhysiology of LaborRodrerick De lafuentesNessuna valutazione finora
- OB1 3.1 Normal Labor and Delivery IDocumento6 pagineOB1 3.1 Normal Labor and Delivery IManjulaNessuna valutazione finora
- BR1 - PSP - Physiology of LaborDocumento41 pagineBR1 - PSP - Physiology of Laborshare fosNessuna valutazione finora
- Overview: Intrapartum Care:: Oxytocin TheoryDocumento5 pagineOverview: Intrapartum Care:: Oxytocin TheoryZach BuenavistaNessuna valutazione finora
- Physiology of LaborDocumento17 paginePhysiology of Laborsennaavia12Nessuna valutazione finora
- 7-Onset & Physiology of LaborDocumento15 pagine7-Onset & Physiology of LaborNlsNessuna valutazione finora
- Labor and Birth Process and NURSING MANAGEMENT (Chapter 13 and 14) False Labor Factors That Affect LaborDocumento7 pagineLabor and Birth Process and NURSING MANAGEMENT (Chapter 13 and 14) False Labor Factors That Affect LaborSHARLAIN GAIL V. MELECIONessuna valutazione finora
- 1 s2.0 S1751721419302301 MainDocumento7 pagine1 s2.0 S1751721419302301 MainLilik AnggrainiNessuna valutazione finora
- 8 Physio OB - Physiology of Labor I - IIDocumento14 pagine8 Physio OB - Physiology of Labor I - IIArnoldBorromeoNessuna valutazione finora
- Normal Labor and DeliveryDocumento116 pagineNormal Labor and DeliveryDagnachew kasayeNessuna valutazione finora
- Labor and DeliveryDocumento114 pagineLabor and DeliveryLouis Carlos Roderos100% (1)
- Normal Labor: Ms. Mayuri Patel Sandra Shroff Rofel College of Nursing, VapiDocumento48 pagineNormal Labor: Ms. Mayuri Patel Sandra Shroff Rofel College of Nursing, Vapivimmy47100% (1)
- (OBa) 1.6 Matrnal Adaptations To Pregnncy (Marinas) - PacisDocumento10 pagine(OBa) 1.6 Matrnal Adaptations To Pregnncy (Marinas) - PacisClyde Yuchengco Cu-unjiengNessuna valutazione finora
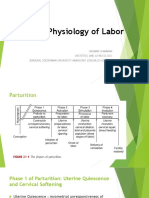
- Four Phases of Parturition: Phase 1 Phase 2 Phase 3 Phase 4Documento2 pagineFour Phases of Parturition: Phase 1 Phase 2 Phase 3 Phase 4Elizer Mario Pre Raboy100% (1)
- Puerperium (Trans)Documento7 paginePuerperium (Trans)Charlie65129Nessuna valutazione finora
- ANNOTATIONDocumento2 pagineANNOTATIONVaniegrace Angel BalagonNessuna valutazione finora
- Induction of LabourDocumento62 pagineInduction of LabourSam christenNessuna valutazione finora
- Phy Ist Stag LBRDocumento9 paginePhy Ist Stag LBRAparna KinginiNessuna valutazione finora
- Ncma217 Week 7Documento5 pagineNcma217 Week 7Polly ArcheronNessuna valutazione finora
- Latent Phase of LaborDocumento8 pagineLatent Phase of LaborKevin SNessuna valutazione finora
- Maternal Reviewer MidtermmDocumento5 pagineMaternal Reviewer Midtermmriveraapriljan22Nessuna valutazione finora
- Faal Partus: Naifah Luthfiyah Putri 15-009Documento58 pagineFaal Partus: Naifah Luthfiyah Putri 15-009NaifahLuthfiyahPutriNessuna valutazione finora
- LaborDocumento32 pagineLaborJustine Vens G. AgustinNessuna valutazione finora
- (Patho OB) Dystocia Due To Abnormalities in Power and Passage-Dr. Ahyong-Reyes (Bernabe)Documento5 pagine(Patho OB) Dystocia Due To Abnormalities in Power and Passage-Dr. Ahyong-Reyes (Bernabe)Shia LevyNessuna valutazione finora
- Disordersofuterinecontractionprecipitatelabourprematurelabourandprolongedlabour 190504053246Documento68 pagineDisordersofuterinecontractionprecipitatelabourprematurelabourandprolongedlabour 190504053246DrPreeti Thakur ChouhanNessuna valutazione finora
- Abnormal Labor + InfertilityDocumento12 pagineAbnormal Labor + InfertilityKristine VanzuelaNessuna valutazione finora
- Abnormal Labor and Infertility 2016 PDFDocumento12 pagineAbnormal Labor and Infertility 2016 PDFLarissa TacalanNessuna valutazione finora
- NCM 107maternal FinalsDocumento84 pagineNCM 107maternal FinalsFranz goNessuna valutazione finora
- (Maternal) FINALSDocumento86 pagine(Maternal) FINALSRM DemetilloNessuna valutazione finora
- The Latent Phase of LaborDocumento8 pagineThe Latent Phase of LaborLoisana Meztli Figueroa PreciadoNessuna valutazione finora
- MCN MidtermsDocumento39 pagineMCN MidtermsJinnijinniNessuna valutazione finora
- Physiology of ParturitionDocumento85 paginePhysiology of ParturitionDark MomentzNessuna valutazione finora
- First Stage of Labor: Midwife Obstetrician InduceDocumento2 pagineFirst Stage of Labor: Midwife Obstetrician InduceChe CacatianNessuna valutazione finora
- Emergency Cases (Document (A4 Portrait) )Documento14 pagineEmergency Cases (Document (A4 Portrait) )Joelyn DulayNessuna valutazione finora
- NCM 107 - SL - Mat - 1Documento100 pagineNCM 107 - SL - Mat - 1marilexdomagsangNessuna valutazione finora
- n3633 MM Module 1 Unit 1Documento71 paginen3633 MM Module 1 Unit 1jonscastro450Nessuna valutazione finora
- Labor: Williams 25th EditionDocumento27 pagineLabor: Williams 25th EditionNoelle Grace Ulep BaromanNessuna valutazione finora
- Physiology of LaborDocumento49 paginePhysiology of LaborGunung MahameruNessuna valutazione finora
- 3F Intranatal NotesDocumento5 pagine3F Intranatal NotesAlyssa Claire TumulakNessuna valutazione finora
- Normal Labor 2013 Nursing GabstDocumento125 pagineNormal Labor 2013 Nursing GabstYibelu BazezewNessuna valutazione finora
- Midl Nursing NowDocumento213 pagineMidl Nursing Nowbemina jaNessuna valutazione finora
- Physiology of LaborDocumento25 paginePhysiology of LaborLaica Barcelona0% (1)
- Puerperium and AnalgesiaDocumento12 paginePuerperium and AnalgesiaKim RamosNessuna valutazione finora
- Intrartum/Intrapartal Period: Phenomena and Process of Labor and Delivery I. Onset of LaborDocumento14 pagineIntrartum/Intrapartal Period: Phenomena and Process of Labor and Delivery I. Onset of Laborclaireaongchua1275Nessuna valutazione finora
- Normal Labor and DeliveryDocumento29 pagineNormal Labor and DeliveryManish ShahNessuna valutazione finora
- 4 Theories of Labor Onset 0 Signs of LaborDocumento13 pagine4 Theories of Labor Onset 0 Signs of Labormamsh KlangNessuna valutazione finora
- Chapter 21Documento2 pagineChapter 21Camilla Fernandez-de DiosNessuna valutazione finora
- BR-mechanism of Human Partition ICADocumento20 pagineBR-mechanism of Human Partition ICARaissa 'Icha' Nurwany RizalNessuna valutazione finora
- Uterine ProlapseDocumento1 paginaUterine ProlapseJeivey VercideNessuna valutazione finora
- Unit 3 1Documento19 pagineUnit 3 1Preeti ChouhanNessuna valutazione finora
- Concept Map Module 5Documento2 pagineConcept Map Module 5Ruthangela GarciaNessuna valutazione finora
- Case 01 - Maternal PhysiologyDocumento5 pagineCase 01 - Maternal PhysiologyRem AlfelorNessuna valutazione finora
- (PHYSIOOB) 2.2 ParturitionDocumento6 pagine(PHYSIOOB) 2.2 ParturitionRONALDO CUANessuna valutazione finora
- OB2 - Problems With The PowerDocumento10 pagineOB2 - Problems With The PowerYanaNessuna valutazione finora
- Intrapartum 1: Intrapartum Period Intrapartal CareDocumento10 pagineIntrapartum 1: Intrapartum Period Intrapartal CareJane MartinNessuna valutazione finora
- 1 Labor and Delivery ProcessDocumento13 pagine1 Labor and Delivery ProcessBardiaga JmayNessuna valutazione finora
- The Breast: Morphology, Physiology, and LactationDa EverandThe Breast: Morphology, Physiology, and LactationNessuna valutazione finora
- The CervixDa EverandThe CervixJoseph JordanNessuna valutazione finora
- Conception to Confinement: Facts an Antenatal Mother should KnowDa EverandConception to Confinement: Facts an Antenatal Mother should KnowNessuna valutazione finora
- Lab DiagnosisDocumento42 pagineLab DiagnosisNestley TiongsonNessuna valutazione finora
- Case Presentation Group 5: Patron Rayo Reyes Salazar Sandhu Sandoval Sangalang SasakiDocumento28 pagineCase Presentation Group 5: Patron Rayo Reyes Salazar Sandhu Sandoval Sangalang SasakiNestley TiongsonNessuna valutazione finora
- Power Passages and Passenger PDFDocumento13 paginePower Passages and Passenger PDFNestley TiongsonNessuna valutazione finora
- Physiology of Parturition PDFDocumento17 paginePhysiology of Parturition PDFNestley TiongsonNessuna valutazione finora
- BioethicsDocumento86 pagineBioethicsNestley TiongsonNessuna valutazione finora
- Clinical AND ADVANCE Pathology: TopicDocumento7 pagineClinical AND ADVANCE Pathology: TopicNestley TiongsonNessuna valutazione finora
- Benign Tumor Vulva Epidemiol OGY Etiology Clinical Manifestation Pathogenesis MorphologyDocumento3 pagineBenign Tumor Vulva Epidemiol OGY Etiology Clinical Manifestation Pathogenesis MorphologyNestley TiongsonNessuna valutazione finora
- Cervical BiopsyDocumento17 pagineCervical BiopsyNestley TiongsonNessuna valutazione finora
- Sexually Transmitted InfectionsDocumento4 pagineSexually Transmitted InfectionsNestley TiongsonNessuna valutazione finora
- Abdominal TraumaDocumento4 pagineAbdominal TraumaNestley TiongsonNessuna valutazione finora
- Immunohematology PDFDocumento126 pagineImmunohematology PDFNicole Tan Calayca100% (1)
- Psych Ward HistoryDocumento6 paginePsych Ward HistoryNestley TiongsonNessuna valutazione finora
- Respi DisordersDocumento8 pagineRespi DisordersNestley TiongsonNessuna valutazione finora
- Clinicopharmacological ConferenceDocumento7 pagineClinicopharmacological ConferenceNestley TiongsonNessuna valutazione finora
- CPC Compiled Report FinalDocumento24 pagineCPC Compiled Report FinalNestley TiongsonNessuna valutazione finora
- Case 2b TuberculosisDocumento37 pagineCase 2b TuberculosisNestley Tiongson100% (1)
- Lungs Benign and MalignantDocumento7 pagineLungs Benign and MalignantNestley TiongsonNessuna valutazione finora
- Cis 2018 PDFDocumento3 pagineCis 2018 PDFTara Oliveros Dela CruzNessuna valutazione finora
- N. Meningitidis (MENINGOCOCCUS) : Meningococcemia/MeningitisDocumento5 pagineN. Meningitidis (MENINGOCOCCUS) : Meningococcemia/MeningitisNestley TiongsonNessuna valutazione finora
- Neuromuscular Junction DsoDocumento9 pagineNeuromuscular Junction DsoNestley TiongsonNessuna valutazione finora
- Adrenal Gland - Surgical PathologyDocumento3 pagineAdrenal Gland - Surgical PathologyNestley TiongsonNessuna valutazione finora
- Clinical Microbiology Laboratory Test RequisitionDocumento1 paginaClinical Microbiology Laboratory Test RequisitionRhodjane Dela Cruz0% (1)
- Maternity Nursing ReviewDocumento54 pagineMaternity Nursing ReviewJr Robis100% (6)
- Legal Medicine Report On Impotency and SterilityDocumento22 pagineLegal Medicine Report On Impotency and SterilityAnna L. Ilagan-MalipolNessuna valutazione finora
- Final Report of PJBL (Organa Genitalia)Documento17 pagineFinal Report of PJBL (Organa Genitalia)NASYWANessuna valutazione finora
- FINAL CervicalCA7BDocumento6 pagineFINAL CervicalCA7BRommel OliverasNessuna valutazione finora
- Addiego, Belzer, Comolli, Moger, Perry, Whipple Female Ejaculation A Case StudyDocumento11 pagineAddiego, Belzer, Comolli, Moger, Perry, Whipple Female Ejaculation A Case StudyCocoNessuna valutazione finora
- Perineal Lacteration PDFDocumento4 paginePerineal Lacteration PDFJocel Mae Aguillon SumagangNessuna valutazione finora
- Proper Abnormal Labour Questions Level 300 2nd SemDocumento30 pagineProper Abnormal Labour Questions Level 300 2nd SemMutale KabweNessuna valutazione finora
- Obstetrics Nursing QuestionsDocumento13 pagineObstetrics Nursing Questionsicy43150% (2)
- Bartholin's Gland Cyst Presenting As Anterior Vaginal Wall Cyst: An Unusual PresentationDocumento2 pagineBartholin's Gland Cyst Presenting As Anterior Vaginal Wall Cyst: An Unusual PresentationNabil Sangga BuanaNessuna valutazione finora
- Prelim Reviewer 2023Documento83 paginePrelim Reviewer 2023jakexsanchez1515Nessuna valutazione finora
- GCPDocumento89 pagineGCPmaria apolonia mancaoNessuna valutazione finora
- Case StudyDocumento45 pagineCase StudykimJCANessuna valutazione finora
- NCP2 - Active PhaseDocumento14 pagineNCP2 - Active PhasepriyankaNessuna valutazione finora
- Medical History Report Medical Prescreen QuestionnaireDocumento4 pagineMedical History Report Medical Prescreen Questionnairejames antonioNessuna valutazione finora
- Non Venereal InfectionsDocumento25 pagineNon Venereal Infectionssahil muhammedNessuna valutazione finora
- Katie The Pure Romance Lady BlogsDocumento20 pagineKatie The Pure Romance Lady Blogskproctor317Nessuna valutazione finora
- People Vs EchegarayDocumento4 paginePeople Vs EchegarayMAry Jovan PanganNessuna valutazione finora
- Nurs 5343 Emergency Obstetrics CareDocumento92 pagineNurs 5343 Emergency Obstetrics CareRachel BiokoNessuna valutazione finora
- Pp. v. Aca-Ac, GR 142500, 2001Documento22 paginePp. v. Aca-Ac, GR 142500, 2001Christia Sandee SuanNessuna valutazione finora
- Libro de Endocrino y FertilidadDocumento684 pagineLibro de Endocrino y FertilidadClaudia Mercedes Alonso Cuevas100% (1)
- REPRODUCTIVE SYSTEM DLP (AutoRecovered)Documento6 pagineREPRODUCTIVE SYSTEM DLP (AutoRecovered)Roshieko Dennise LaraNessuna valutazione finora
- Medical Instruments by Kiboma JamesDocumento27 pagineMedical Instruments by Kiboma Jamesf.abrahamNessuna valutazione finora
- Whitehouse V Jordan (1980) UKHL 12 (17 December 1980)Documento27 pagineWhitehouse V Jordan (1980) UKHL 12 (17 December 1980)Natalie DouglasNessuna valutazione finora
- Ob - Maternal AnatomyDocumento8 pagineOb - Maternal AnatomyLeslee Cruz - BernardinoNessuna valutazione finora
- 1.7 Surgery For Cyst or Abscess of The Bartholin Gland With Special Reference To The Newer OperatasDocumento3 pagine1.7 Surgery For Cyst or Abscess of The Bartholin Gland With Special Reference To The Newer OperatasMuh IkhsanNessuna valutazione finora
- Exilis Ultra 360 Catalogue 6hFRZpjsQ2iiiLJDocumento13 pagineExilis Ultra 360 Catalogue 6hFRZpjsQ2iiiLJJohn LuNessuna valutazione finora