Potrebbero piacerti anche
- Review Article Role of Colors in Therapeutics Swami Gaurav: Volume: I: Issue-3: Nov-Dec - 2010Documento6 pagineReview Article Role of Colors in Therapeutics Swami Gaurav: Volume: I: Issue-3: Nov-Dec - 2010DidikPrasetyoSuliNessuna valutazione finora
- About Education in The UK: A. BackgroundDocumento3 pagineAbout Education in The UK: A. BackgroundDidikPrasetyoSuliNessuna valutazione finora
- IMPORTANT INFORMATION-Documenation AuditDocumento4 pagineIMPORTANT INFORMATION-Documenation AuditDidikPrasetyoSuliNessuna valutazione finora
- SpeakingDocumento1 paginaSpeakingDidikPrasetyoSuliNessuna valutazione finora
- Describing WoundsDocumento4 pagineDescribing WoundsDidikPrasetyoSuliNessuna valutazione finora
- Pen JaraDocumento12 paginePen JaraDidikPrasetyoSuliNessuna valutazione finora
- Benzathine Penicillin G For The Management of RHDDocumento8 pagineBenzathine Penicillin G For The Management of RHDDidikPrasetyoSuliNessuna valutazione finora
- Lampiran 9 Tabulasi Data Umum Karakteristik Pekerja Penambang BelerangDocumento2 pagineLampiran 9 Tabulasi Data Umum Karakteristik Pekerja Penambang BelerangDidikPrasetyoSuliNessuna valutazione finora
- SGRDGFGD FullDocumento9 pagineSGRDGFGD FullDidikPrasetyoSuliNessuna valutazione finora
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5795)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (74)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1091)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- Nice Pre y Post NatalDocumento369 pagineNice Pre y Post NatalBernardo LinaresNessuna valutazione finora
- TDM of Valproic AcidDocumento43 pagineTDM of Valproic Acidryo_ninukNessuna valutazione finora
- The Contribution of Environmental Exposure To The Etiology of Autism Spectrum DisorderDocumento23 pagineThe Contribution of Environmental Exposure To The Etiology of Autism Spectrum DisorderCristina SolerNessuna valutazione finora
- Advisory On Reiteration of Ao 2021 0012 Implementing Guidelines On The Medicine Access Program For Health 2Documento7 pagineAdvisory On Reiteration of Ao 2021 0012 Implementing Guidelines On The Medicine Access Program For Health 2ncd.bulacanNessuna valutazione finora
- The National Drugs List: of Syrian Arab RepublicDocumento72 pagineThe National Drugs List: of Syrian Arab RepublicportosinNessuna valutazione finora
- DepakoteDocumento2 pagineDepakotedana100% (1)
- Emergency Management of The Paediatric Patient With Convulsive Status Epilepticus - Canadian Paediatric SocietyDocumento7 pagineEmergency Management of The Paediatric Patient With Convulsive Status Epilepticus - Canadian Paediatric SocietyAlberto VictorNessuna valutazione finora
- Neurology Question Bank 2015Documento99 pagineNeurology Question Bank 2015Paz Vida100% (7)
- Tienam Leaflet Eng-102!12!03Documento2 pagineTienam Leaflet Eng-102!12!03MikeNessuna valutazione finora
- Approach To Epilepsy POWER POINT - EDITEDDocumento41 pagineApproach To Epilepsy POWER POINT - EDITEDVipul NagnesiaNessuna valutazione finora
- PhenyltriazineDocumento2 paginePhenyltriazineabcdeNessuna valutazione finora
- Seizures and Epilepsy in Patients With Ischaemic StrokeDocumento17 pagineSeizures and Epilepsy in Patients With Ischaemic StrokeAnali Durán CorderoNessuna valutazione finora
- Valproic AcidDocumento5 pagineValproic AcidMark PradsNessuna valutazione finora
- Drugs Med-SurgTest 3Documento6 pagineDrugs Med-SurgTest 3Sarah PlunkettNessuna valutazione finora
- DR Kakaza Lectures and Ward Round Notes - 0220Documento61 pagineDR Kakaza Lectures and Ward Round Notes - 0220sun108100% (1)
- Anti Epileptic Drugs: Department of Pharmacology, SMS Medical College, JPRDocumento24 pagineAnti Epileptic Drugs: Department of Pharmacology, SMS Medical College, JPRAnitha Mary DambaleNessuna valutazione finora
- USFDA Approvals by CompanyDocumento136 pagineUSFDA Approvals by CompanyAsthaNessuna valutazione finora
- Drug Study PsychiaDocumento10 pagineDrug Study PsychiaIRA MONIQUE CABADENNessuna valutazione finora
- Epilepsy and Seizure DisordersDocumento38 pagineEpilepsy and Seizure DisordersMalueth AnguiNessuna valutazione finora
- Somali Essential Medicines List 2019Documento36 pagineSomali Essential Medicines List 2019Usama MohaNessuna valutazione finora
- Valproic AcidDocumento15 pagineValproic AcidNadya PrafitaNessuna valutazione finora
- Valproate-Induced Hair Loss - What To Tell Patients - MDedge PsychiatryDocumento3 pagineValproate-Induced Hair Loss - What To Tell Patients - MDedge Psychiatrydo leeNessuna valutazione finora
- Complete Drug FormularyDocumento96 pagineComplete Drug FormularyRPh Krishna Chandra JagritNessuna valutazione finora
- Practice Guidelines: ACOG Guidelines On Psychiatric Medication Use During Pregnancy and Lactation - American Family PhysicianDocumento4 paginePractice Guidelines: ACOG Guidelines On Psychiatric Medication Use During Pregnancy and Lactation - American Family PhysicianKim Villeneuve100% (1)
- Neuropsych RX CardsDocumento15 pagineNeuropsych RX CardsLarry TenhoffNessuna valutazione finora
- Pharmacology of Drugs Acting On Central Nervous System 1st (Mam) PDFDocumento47 paginePharmacology of Drugs Acting On Central Nervous System 1st (Mam) PDFRahul palsNessuna valutazione finora
- Valproate Interaction With Carbapenems: Review and RecommendationsDocumento7 pagineValproate Interaction With Carbapenems: Review and RecommendationsGajah NauliNessuna valutazione finora
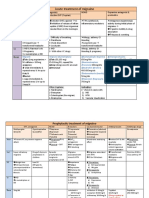
- Acute Treatment of Migraine: ActionDocumento3 pagineAcute Treatment of Migraine: ActionFathy ElsheshtawyNessuna valutazione finora
- Multiple Choice Questions For Part IVDocumento18 pagineMultiple Choice Questions For Part IVTarek MohsenNessuna valutazione finora
- Valproic Acid and Risperidone: A Drug Interaction?: To The EditorDocumento2 pagineValproic Acid and Risperidone: A Drug Interaction?: To The EditorFariz RifqiNessuna valutazione finora