Potrebbero piacerti anche
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- Post ProductionDocumento1 paginaPost ProductionClarkKent Fabro BatucanNessuna valutazione finora
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- BPP 170-194Documento25 pagineBPP 170-194ClarkKent Fabro BatucanNessuna valutazione finora
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- BPP 144-169Documento25 pagineBPP 144-169ClarkKent Fabro BatucanNessuna valutazione finora
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- Immersion Evaluation ToolsDocumento1 paginaImmersion Evaluation ToolsClarkKent Fabro BatucanNessuna valutazione finora
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- SAVE THE DATE (August 21-22, 2018) : (Board Walk, Rotunda, Heritage Sites)Documento1 paginaSAVE THE DATE (August 21-22, 2018) : (Board Walk, Rotunda, Heritage Sites)ClarkKent Fabro BatucanNessuna valutazione finora
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- SHS Core - Contemporary Philippine Arts From The Regions CG PDFDocumento4 pagineSHS Core - Contemporary Philippine Arts From The Regions CG PDFJake Arman Principe79% (33)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Moving ExamDocumento2 pagineMoving ExamClarkKent Fabro BatucanNessuna valutazione finora
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- Session PlanDocumento5 pagineSession PlanClarkKent Fabro Batucan100% (1)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- SF1 & 2Documento47 pagineSF1 & 2ClarkKent Fabro BatucanNessuna valutazione finora
- Identifying School and Community: Resources in Case of An Injury or EmergencyDocumento12 pagineIdentifying School and Community: Resources in Case of An Injury or EmergencyClarkKent Fabro BatucanNessuna valutazione finora
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- Fuel and Engine Control NewDocumento1 paginaFuel and Engine Control NewClarkKent Fabro BatucanNessuna valutazione finora
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (74)
- The History of IlganDocumento1 paginaThe History of IlganClarkKent Fabro BatucanNessuna valutazione finora
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- Simple Interest A P (1 + RT) Compound Interest A P (1 +R/T) Future Value With Simple Interest F P (1 +RT)Documento1 paginaSimple Interest A P (1 + RT) Compound Interest A P (1 +R/T) Future Value With Simple Interest F P (1 +RT)ClarkKent Fabro BatucanNessuna valutazione finora
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- Ohms Law WorksheetDocumento1 paginaOhms Law WorksheetMohmmed Ahmed100% (1)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- Elements of LiteratureDocumento2 pagineElements of LiteratureClarkKent Fabro BatucanNessuna valutazione finora
- KPI's: March 4, 2019Documento15 pagineKPI's: March 4, 2019ClarkKent Fabro BatucanNessuna valutazione finora
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- EIM - NewDocumento43 pagineEIM - NewClarkKent Fabro BatucanNessuna valutazione finora
- Possible Questions For Oral Questioning (FBS NC II)Documento31 paginePossible Questions For Oral Questioning (FBS NC II)ClarkKent Fabro BatucanNessuna valutazione finora
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- KPI's: March 4, 2019Documento15 pagineKPI's: March 4, 2019ClarkKent Fabro BatucanNessuna valutazione finora
- Chapter 1Documento9 pagineChapter 1ClarkKent Fabro Batucan100% (1)
- LABEL For SchoolDocumento2 pagineLABEL For SchoolClarkKent Fabro BatucanNessuna valutazione finora
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- SHS Core - Contemporary Philippine Arts From The Regions CG PDFDocumento4 pagineSHS Core - Contemporary Philippine Arts From The Regions CG PDFJake Arman Principe79% (33)
- ZorenDocumento1 paginaZorenClarkKent Fabro BatucanNessuna valutazione finora
- SHS Core - Personal Development CG in English 20160224 PDFDocumento6 pagineSHS Core - Personal Development CG in English 20160224 PDFcaroline dullete100% (6)
- Lesson Plan in MathDocumento1 paginaLesson Plan in MathClarkKent Fabro BatucanNessuna valutazione finora
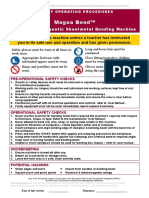
- Magna Bend SopDocumento1 paginaMagna Bend SopClarkKent Fabro Batucan0% (1)
- CosmoDocumento87 pagineCosmovrihad100% (1)
- Student Questionnaire Vocational Upper Secondary Education (Grade 11)Documento9 pagineStudent Questionnaire Vocational Upper Secondary Education (Grade 11)ClarkKent Fabro BatucanNessuna valutazione finora
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- SHS Core - Personal Development CG in English 20160224 PDFDocumento6 pagineSHS Core - Personal Development CG in English 20160224 PDFcaroline dullete100% (6)
- NLN Medication Exam Study Guide QuizletDocumento36 pagineNLN Medication Exam Study Guide Quizletmaniz442Nessuna valutazione finora
- Musicophilia Tales of Music and The BrainDocumento3 pagineMusicophilia Tales of Music and The BrainClark's Eye on Books0% (1)
- Guidelines For High Flow Oxygen Therapy (AIRVO ) On The WardsDocumento11 pagineGuidelines For High Flow Oxygen Therapy (AIRVO ) On The WardsBurhanNessuna valutazione finora
- Book-Color Therapy-Bioptroninfow Q&ADocumento13 pagineBook-Color Therapy-Bioptroninfow Q&ASherry ImhofNessuna valutazione finora
- Eating Disorder Examination Questionnaire PDFDocumento5 pagineEating Disorder Examination Questionnaire PDFLuka KukinaNessuna valutazione finora
- Piperacilina Tazobactam Vs Meropenem en BacteremiasDocumento11 paginePiperacilina Tazobactam Vs Meropenem en BacteremiasSMIBA MedicinaNessuna valutazione finora
- Problem Statement: "Effectiveness of Mint Leaves Paste On Dysmenorrhea Among Adolescent Girls"Documento12 pagineProblem Statement: "Effectiveness of Mint Leaves Paste On Dysmenorrhea Among Adolescent Girls"tanmai nooluNessuna valutazione finora
- Promo Pinkerbell ClinicDocumento3 paginePromo Pinkerbell ClinicNatalia DeviaNessuna valutazione finora
- CBT The Evidence Based ApproachDocumento22 pagineCBT The Evidence Based ApproachzoyachaudharycollegeNessuna valutazione finora
- Autoimmune Hepatitis - SLE Overlap SyndromeDocumento2 pagineAutoimmune Hepatitis - SLE Overlap SyndromeMulyono Aba AthiyaNessuna valutazione finora
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- DiltiazemDocumento2 pagineDiltiazemE100% (1)
- Immersive VR SCIDocumento11 pagineImmersive VR SCIsana siddiqueNessuna valutazione finora
- Diabetes FactsDocumento3 pagineDiabetes Factsfirdauskm100% (1)
- Case Study For OligohydramniosDocumento7 pagineCase Study For Oligohydramniosbjhilario86% (14)
- Salvador Minuchin On Family Therapy: Instructor'S ManualDocumento48 pagineSalvador Minuchin On Family Therapy: Instructor'S ManualAisyah Zulkepli100% (1)
- PBL Lobs Liver WeekDocumento7 paginePBL Lobs Liver WeekescuchoNessuna valutazione finora
- An English Translation of The Sushruta Samhita Vol 3 Uttara Tantra (1916) - Kaviraj Kunja Lal Bhishagratna PDFDocumento534 pagineAn English Translation of The Sushruta Samhita Vol 3 Uttara Tantra (1916) - Kaviraj Kunja Lal Bhishagratna PDFspandaa100% (1)
- Nerve Conduction StudiesDocumento5 pagineNerve Conduction Studiessen ANessuna valutazione finora
- 2007 PN Test PreparationDocumento29 pagine2007 PN Test Preparationfairwoods80% (5)
- Kinetic Control Cap1Documento17 pagineKinetic Control Cap1Yennifer Serna MoncadaNessuna valutazione finora
- Udan's Neuro, Musculoskel, EentDocumento2 pagineUdan's Neuro, Musculoskel, EentReygie Marsada100% (4)
- Development of A Classification System For Periodontal Diseases and Conditions - Armitage 1999Documento6 pagineDevelopment of A Classification System For Periodontal Diseases and Conditions - Armitage 1999csryderNessuna valutazione finora
- 2014 June - Makomba Games For Diabetic Children - Presentation at ILAMI Tel Aviv - Ofer Atzmon PDFDocumento25 pagine2014 June - Makomba Games For Diabetic Children - Presentation at ILAMI Tel Aviv - Ofer Atzmon PDFOfer AtzmonNessuna valutazione finora
- ABTBook PDFDocumento142 pagineABTBook PDFCoca TemeliescuNessuna valutazione finora
- Idjsr 5 (1) 25-28Documento4 pagineIdjsr 5 (1) 25-28Krupali JainNessuna valutazione finora
- A Case of Chronic Insomnia Cured by HomoeopathyDocumento6 pagineA Case of Chronic Insomnia Cured by HomoeopathyHomoeopathic Pulse100% (2)
- Ajakaiye Deborah Letter of Reference (HCPC) Uith DraftDocumento3 pagineAjakaiye Deborah Letter of Reference (HCPC) Uith DraftTimz CityNessuna valutazione finora
- Acute Respiratory Distress in ChildrenDocumento25 pagineAcute Respiratory Distress in Childrensai ram100% (1)
- Cleft Palate: Wan Khadijah Wan Yusoff Noor Afika Binti AzriDocumento91 pagineCleft Palate: Wan Khadijah Wan Yusoff Noor Afika Binti AzriWOne WannNessuna valutazione finora
- Ercp (Baron)Documento487 pagineErcp (Baron)Ciprian-Nicolae MunteanNessuna valutazione finora