Potrebbero piacerti anche
- Spinal Cord: Anatomy and NeuroimagingDocumento52 pagineSpinal Cord: Anatomy and NeuroimagingslojnotakNessuna valutazione finora
- Motor and Sensory Examination: Dr. Bandar Al Jafen, MD Consultant NeurologistDocumento36 pagineMotor and Sensory Examination: Dr. Bandar Al Jafen, MD Consultant NeurologistJim Jose Antony100% (1)
- Chromosomal AbnormalitiesDocumento3 pagineChromosomal AbnormalitiesYra Mie DitaroNessuna valutazione finora
- Cranial Rhythmic Impulse Related To The Traube-Hering-Mayer OscillationDocumento11 pagineCranial Rhythmic Impulse Related To The Traube-Hering-Mayer Oscillationthe_walnutNessuna valutazione finora
- Psycholinguistics: Language Disorder: Broca's AphasiaDocumento18 paginePsycholinguistics: Language Disorder: Broca's AphasiaSuciati AnandesNessuna valutazione finora
- Diagnosis of Systemic Lupus ErythematosusDocumento6 pagineDiagnosis of Systemic Lupus ErythematosusMuhammad Akhram ResmanaNessuna valutazione finora
- Tall StatureDocumento24 pagineTall StaturedianmutiaNessuna valutazione finora
- Epigenetics of EndometriosisDocumento21 pagineEpigenetics of EndometriosisirwinaNessuna valutazione finora
- Cluster Headache - MedlinePlus Medical EncyclopediaDocumento3 pagineCluster Headache - MedlinePlus Medical EncyclopediaUtpal KumarNessuna valutazione finora
- REFLEXESDocumento15 pagineREFLEXESSonali Soumyashree100% (2)
- Spinal CordDocumento4 pagineSpinal CordMabel LynNessuna valutazione finora
- Amyotrophic Lateral Sclerosis (ALS)Documento19 pagineAmyotrophic Lateral Sclerosis (ALS)adilabasi100% (1)
- Copy-Classification of Psychiatric DisordersDocumento56 pagineCopy-Classification of Psychiatric Disordersshadrach bineyNessuna valutazione finora
- Apraxia, Agnosia and Disconnection SyndromesDocumento65 pagineApraxia, Agnosia and Disconnection SyndromesDhawal Narang100% (1)
- Alzheimer's Disease and Oral CareDocumento5 pagineAlzheimer's Disease and Oral CarebkprosthoNessuna valutazione finora
- Fact Sheet 1 - Addiction OverviewDocumento5 pagineFact Sheet 1 - Addiction Overviewgoldbergleah100% (1)
- Disoreder of PerceptionDocumento36 pagineDisoreder of PerceptionUmar Khan100% (1)
- Parietal Lobe TestingDocumento5 pagineParietal Lobe TestingvinodksahuNessuna valutazione finora
- Brain Areas - Location and FunctionDocumento12 pagineBrain Areas - Location and FunctionMattGilmoreNessuna valutazione finora
- Paranoid Schizophrenia: OlehDocumento52 pagineParanoid Schizophrenia: Olehbunga julia100% (1)
- Explore the Nervous System in 40 CharactersDocumento31 pagineExplore the Nervous System in 40 CharactersDeology JuaninoNessuna valutazione finora
- Amyotrophic Lateral SclerosisDocumento15 pagineAmyotrophic Lateral SclerosisYakan AbdulrahmanNessuna valutazione finora
- Efferent Visual System (Ocular Motor Pathways)Documento38 pagineEfferent Visual System (Ocular Motor Pathways)riskhapangestika100% (1)
- Chapter14 Aphasia FINAL 16edDocumento83 pagineChapter14 Aphasia FINAL 16edAldo Hip NaranjoNessuna valutazione finora
- D.O School InformationDocumento102 pagineD.O School Informationkape1oneNessuna valutazione finora
- National Aphasia Association (NAADocumento10 pagineNational Aphasia Association (NAAAmorBabe Tabasa-PescaderoNessuna valutazione finora
- Acid-Base Regulation and Disorders: Key ConceptsDocumento54 pagineAcid-Base Regulation and Disorders: Key ConceptsPaolo Uccello100% (1)
- Epileptology Book PDFDocumento280 pagineEpileptology Book PDFRikizu HobbiesNessuna valutazione finora
- The Anatomy of the Human Peritoneum and Abdominal Cavity: Considered from the Standpoint of Development and Comparative AnatomyDa EverandThe Anatomy of the Human Peritoneum and Abdominal Cavity: Considered from the Standpoint of Development and Comparative AnatomyNessuna valutazione finora
- Autonomic Nervous SystemDocumento20 pagineAutonomic Nervous Systempeter911xNessuna valutazione finora
- Introduction and Organization of Nervous System: Presented by Dr. Amen FatimaDocumento37 pagineIntroduction and Organization of Nervous System: Presented by Dr. Amen FatimaShanailNessuna valutazione finora
- Understanding Stroke and HemiplegiaDocumento17 pagineUnderstanding Stroke and HemiplegiaSathias SundariNessuna valutazione finora
- Temporal LobeDocumento68 pagineTemporal LobeRupinder GillNessuna valutazione finora
- PALS Helpful Hints 2015 Guidelines Posted Nov 2016Documento5 paginePALS Helpful Hints 2015 Guidelines Posted Nov 2016Mj Teate100% (1)
- Clinical Approach To Brainstem LesionsDocumento10 pagineClinical Approach To Brainstem LesionsJosé SánchezNessuna valutazione finora
- AphasiaDocumento71 pagineAphasiaVarun B RenukappaNessuna valutazione finora
- Approach To Myopathy by AnkitDocumento83 pagineApproach To Myopathy by AnkitankitNessuna valutazione finora
- Cervical Cancer: Causes, Symptoms, Prevention & TreatmentDocumento21 pagineCervical Cancer: Causes, Symptoms, Prevention & TreatmentKen Edward ZataNessuna valutazione finora
- Organization of the Nervous System: Neurons, Glia & ClassificationDocumento33 pagineOrganization of the Nervous System: Neurons, Glia & ClassificationOctavio Mancini100% (2)
- The Truth About The Flu ShotDocumento5 pagineThe Truth About The Flu ShotPoorMexicanNessuna valutazione finora
- Spinal CordDocumento48 pagineSpinal CordDr.Saber - Ar - Raffi100% (1)
- Infusion Pumps, Large-Volume - 040719081048Documento59 pagineInfusion Pumps, Large-Volume - 040719081048Freddy Cruz BeltranNessuna valutazione finora
- CP PDFDocumento7 pagineCP PDFannaNessuna valutazione finora
- A1. Functional Areas of Cerebral CortexDocumento3 pagineA1. Functional Areas of Cerebral Cortexspindr07Nessuna valutazione finora
- Nervous SystemDocumento49 pagineNervous SystemJoyce NieveraNessuna valutazione finora
- Phantom Limbs and Plastic BrainDocumento19 paginePhantom Limbs and Plastic BrainZinneRah RahManNessuna valutazione finora
- Classification of Sleep DisordersDocumento15 pagineClassification of Sleep Disorderselvinegunawan100% (1)
- Mental Status Examination (Mse) : The MSE Is A "Snapshot" of A Patient at A Specific TimeDocumento19 pagineMental Status Examination (Mse) : The MSE Is A "Snapshot" of A Patient at A Specific TimeSree ZNessuna valutazione finora
- Sarawuth Noppiboon ID 56070700020 BioPhEPs SystemsDocumento5 pagineSarawuth Noppiboon ID 56070700020 BioPhEPs SystemsSarawuth NoppiboonNessuna valutazione finora
- Brain Anatomy and FunctionDocumento8 pagineBrain Anatomy and FunctionwildankunNessuna valutazione finora
- Functional Areas of BrainDocumento8 pagineFunctional Areas of BrainirfanzukriNessuna valutazione finora
- Anat 6.6 Cerebellum - DeriadaDocumento11 pagineAnat 6.6 Cerebellum - Deriadalovelots1234Nessuna valutazione finora
- Anatomy and Physiology of BrainDocumento21 pagineAnatomy and Physiology of BrainNavjot BrarNessuna valutazione finora
- Anatomical Positions and Terminology GuideDocumento127 pagineAnatomical Positions and Terminology GuideMaria JozilynNessuna valutazione finora
- Necrosis NotesDocumento3 pagineNecrosis Notesjerad19Nessuna valutazione finora
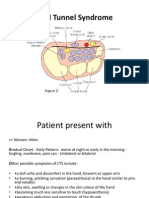
- Carpal Tunnel Syndrome Power Point PresentationDocumento6 pagineCarpal Tunnel Syndrome Power Point Presentationapi-237061134Nessuna valutazione finora
- Type Gene Description: Becker's Muscular Dystrophy Duchenne Muscular Dystrophy DystrophinDocumento4 pagineType Gene Description: Becker's Muscular Dystrophy Duchenne Muscular Dystrophy DystrophinNikhilKapoorNessuna valutazione finora
- Students Clinical Case AnalysisDocumento5 pagineStudents Clinical Case Analysisjacc_282Nessuna valutazione finora
- Cerebellum AnatomyDocumento21 pagineCerebellum AnatomyhassaanjamilNessuna valutazione finora
- Notes Lecture No 1 PathologyDocumento4 pagineNotes Lecture No 1 PathologyDr-Rukhshanda RamzanNessuna valutazione finora
- Nerve InjuryDocumento46 pagineNerve InjuryNofilia Citra CandraNessuna valutazione finora
- Diseases of The Spinal CordDocumento89 pagineDiseases of The Spinal CordLolla SinwarNessuna valutazione finora
- CNS Tumors: Adult Tumors Tend To Be Supratentorial (70%) Pediatric Tumors Tend To Be Infratentorial (70%)Documento8 pagineCNS Tumors: Adult Tumors Tend To Be Supratentorial (70%) Pediatric Tumors Tend To Be Infratentorial (70%)Jessica Febrina WuisanNessuna valutazione finora
- Cerebral Hemispheres 2018 PDFDocumento69 pagineCerebral Hemispheres 2018 PDFlailatul husnaNessuna valutazione finora
- Depanshu Belwal Power PointDocumento12 pagineDepanshu Belwal Power PointvickyvermaNessuna valutazione finora
- Types of ExcerciseDocumento13 pagineTypes of ExcerciseTefera LeteboNessuna valutazione finora
- Neurology - Headache NotesDocumento3 pagineNeurology - Headache NotessarahNessuna valutazione finora
- Pseudo BulbarDocumento5 paginePseudo BulbarRegina CaeciliaNessuna valutazione finora
- Nerve Muscle PhysioDocumento30 pagineNerve Muscle Physiopatel_hanisha06Nessuna valutazione finora
- Craniovertebral Junction Anatomy & RadiologyDocumento130 pagineCraniovertebral Junction Anatomy & Radiologydrarunrao100% (1)
- Lowe Syndrome (Oculocerebrorenal syndrome) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsDa EverandLowe Syndrome (Oculocerebrorenal syndrome) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNessuna valutazione finora
- Noac GuidelinesDocumento40 pagineNoac GuidelinesCocosul Cocosului CocosaruluiNessuna valutazione finora
- Alvis-Miranda WhatDocumento11 pagineAlvis-Miranda WhatRikizu HobbiesNessuna valutazione finora
- Autonomic Disfunction in Primary Sleep DisorderDocumento64 pagineAutonomic Disfunction in Primary Sleep DisorderRikizu HobbiesNessuna valutazione finora
- Peripheral Neuropathy: Neurology Rotation Lecture SeriesDocumento9 paginePeripheral Neuropathy: Neurology Rotation Lecture SeriesFandi Dwi CahyandiNessuna valutazione finora
- Basic UltrasoundDocumento43 pagineBasic UltrasoundRikizu HobbiesNessuna valutazione finora
- Mitochondrial Myopathy and Exercise PresentationDocumento103 pagineMitochondrial Myopathy and Exercise PresentationRikizu HobbiesNessuna valutazione finora
- ParkinsonDocumento86 pagineParkinsonRikizu HobbiesNessuna valutazione finora
- Jadwal SimposiumDocumento2 pagineJadwal SimposiumRikizu HobbiesNessuna valutazione finora
- ParkinsonDocumento86 pagineParkinsonRikizu HobbiesNessuna valutazione finora
- Neuro-Talk Taunton 2014Documento29 pagineNeuro-Talk Taunton 2014Rikizu HobbiesNessuna valutazione finora
- Mitochondrial Myopathy: How Exercise Can HelpDocumento36 pagineMitochondrial Myopathy: How Exercise Can HelpSri HariNessuna valutazione finora
- Neuropathic Pain - Diagnosis Mechanism and ManagementDocumento66 pagineNeuropathic Pain - Diagnosis Mechanism and ManagementRikizu HobbiesNessuna valutazione finora
- AlsDocumento22 pagineAlsRikizu Hobbies100% (1)
- Als PPTDocumento8 pagineAls PPTRikizu HobbiesNessuna valutazione finora
- Activities of Daily Living: Basic Health & Safety #1 DSP Core Curriculum RequirementDocumento24 pagineActivities of Daily Living: Basic Health & Safety #1 DSP Core Curriculum RequirementRikizu HobbiesNessuna valutazione finora
- Activities of Daily LivingDocumento29 pagineActivities of Daily LivingAsraa MaryamNessuna valutazione finora
- Complications of Com: Dr. Ajay Manickam Junior Resident, Dept of Ent RG Kar Medical CollegeDocumento88 pagineComplications of Com: Dr. Ajay Manickam Junior Resident, Dept of Ent RG Kar Medical CollegeRikizu Hobbies100% (1)
- Aan Guideline 887 PDFDocumento110 pagineAan Guideline 887 PDFRikizu HobbiesNessuna valutazione finora
- 387-Article Text-3866-1-10-20100329Documento5 pagine387-Article Text-3866-1-10-20100329Rikizu HobbiesNessuna valutazione finora
- Case Series Otogenic Brain AbcessDocumento31 pagineCase Series Otogenic Brain AbcessRikizu HobbiesNessuna valutazione finora
- AneurysmDocumento62 pagineAneurysmRikizu HobbiesNessuna valutazione finora
- Lim 2017Documento19 pagineLim 2017Rikizu HobbiesNessuna valutazione finora
- Otogenic Brain AbscessDocumento27 pagineOtogenic Brain AbscessRikizu HobbiesNessuna valutazione finora
- DeOliveiraManoel AneurysmalSubarachnoidHemorrhage PDFDocumento16 pagineDeOliveiraManoel AneurysmalSubarachnoidHemorrhage PDFRikizu HobbiesNessuna valutazione finora
- 387 3866 1 PB PDFDocumento4 pagine387 3866 1 PB PDFMannit ButtarNessuna valutazione finora
- Altmann 2016Documento5 pagineAltmann 2016Rikizu HobbiesNessuna valutazione finora
- A J B P R: Sian Ournal of Iochemical and Harmaceutical EsearchDocumento5 pagineA J B P R: Sian Ournal of Iochemical and Harmaceutical EsearchNAVNEET BAGGANessuna valutazione finora
- Signs of Latent TetanyDocumento3 pagineSigns of Latent TetanyJohn GettyNessuna valutazione finora
- Fistulas Enterocutaneas MaingotDocumento20 pagineFistulas Enterocutaneas MaingotroyvillafrancaNessuna valutazione finora
- Ijmrhs Vol 2 Issue 1Documento110 pagineIjmrhs Vol 2 Issue 1editorijmrhs100% (1)
- Malignant Hyperthermia: Pre-Hospital Emergency Care Recommendations Recommendations For Hospital Emergency DepartmentsDocumento6 pagineMalignant Hyperthermia: Pre-Hospital Emergency Care Recommendations Recommendations For Hospital Emergency DepartmentsHelend Ndra TaribukaNessuna valutazione finora
- TOPIC 3.A Bag TechniqueDocumento38 pagineTOPIC 3.A Bag TechniqueJayrelle D. Safran100% (1)
- A History of Prostate Cancer Cancer, Men and Medicine First Edition PDFDocumento248 pagineA History of Prostate Cancer Cancer, Men and Medicine First Edition PDFMarcela Osorio DugandNessuna valutazione finora
- Probiotics vs Prebiotics: Differences, Advantages, TrendsDocumento5 pagineProbiotics vs Prebiotics: Differences, Advantages, TrendsNaevisweloveuNessuna valutazione finora
- How To Protect Yourself and OthersDocumento2 pagineHow To Protect Yourself and OtherslistmyclinicNessuna valutazione finora
- SurgeryDocumento3 pagineSurgeryBanu KubendiranNessuna valutazione finora
- Microchem Non GLP ASTM E1052 Study Report NG14797Documento6 pagineMicrochem Non GLP ASTM E1052 Study Report NG14797MaryDianne RamosNessuna valutazione finora
- Impact of Estrogen Type On Cardiovascular Safety of Combined OralDocumento12 pagineImpact of Estrogen Type On Cardiovascular Safety of Combined OralMary SuescaNessuna valutazione finora
- AIDS (Powerpoint Summary)Documento14 pagineAIDS (Powerpoint Summary)iris203550% (2)
- Miliaria Pustulosa (Infetrop)Documento11 pagineMiliaria Pustulosa (Infetrop)Muhammad mukramNessuna valutazione finora
- Qip ProjectDocumento13 pagineQip Projectapi-534216481Nessuna valutazione finora
- Enzyme Disorder ProjectDocumento10 pagineEnzyme Disorder Projectria wuNessuna valutazione finora
- Organ Systems InterviewDocumento2 pagineOrgan Systems InterviewJohn Carlo MontemayorNessuna valutazione finora
- Approved Private Hospitals List for CG Govt EmployeesDocumento12 pagineApproved Private Hospitals List for CG Govt Employeesm_asitNessuna valutazione finora
- SimChart Charting RequirementsDocumento3 pagineSimChart Charting RequirementsMatt McClenahanNessuna valutazione finora
- What Is ScabiesDocumento7 pagineWhat Is ScabiesKenNessuna valutazione finora
- 3rd Summer EvalDocumento5 pagine3rd Summer Evalapi-569210408Nessuna valutazione finora
- Understanding Plasma Cell Dyscrasias: MGUS, Myeloma, Waldenstrom's and AmyloidosisDocumento41 pagineUnderstanding Plasma Cell Dyscrasias: MGUS, Myeloma, Waldenstrom's and AmyloidosisDr MonikaNessuna valutazione finora