Potrebbero piacerti anche
- MCQ Thoracic SurgeryDocumento5 pagineMCQ Thoracic SurgeryKhamis Belal100% (6)
- FCPS Part1 Q BANK Physiology Flash Cards Very Important For Part 1Documento49 pagineFCPS Part1 Q BANK Physiology Flash Cards Very Important For Part 1Sehar IqbalNessuna valutazione finora
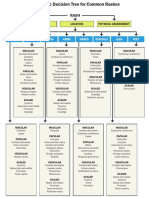
- WK 5 Rash Decision TreeDocumento1 paginaWK 5 Rash Decision TreeBetsy Brown ByersmithNessuna valutazione finora
- Answer Diagnosis: 1. RhythmDocumento2 pagineAnswer Diagnosis: 1. RhythmSuggula Vamsi KrishnaNessuna valutazione finora
- ATLSDocumento15 pagineATLSsouthstar9989% (9)
- Haemopoiesis: Composition of Whole Blood & Its ComponentsDocumento8 pagineHaemopoiesis: Composition of Whole Blood & Its ComponentsSafiya JamesNessuna valutazione finora
- Low BP - Decreased Cardiac Output - Improved Renal Blood FlowDocumento2 pagineLow BP - Decreased Cardiac Output - Improved Renal Blood Flowtantalizin marieNessuna valutazione finora
- 1 Ge Stimulations Mast Cell Degeneration Asthma AttackDocumento4 pagine1 Ge Stimulations Mast Cell Degeneration Asthma Attacknebbie06Nessuna valutazione finora
- Gene Related DiseaseDocumento3 pagineGene Related Diseasevivek govardhanamNessuna valutazione finora
- Genitourinary System: Renal FailureDocumento6 pagineGenitourinary System: Renal FailureEn ConejosNessuna valutazione finora
- Mnemonic of Some Rare Genetic Disease PDFDocumento9 pagineMnemonic of Some Rare Genetic Disease PDFfaraz100% (1)
- Staph. Aureus Staph. Epidermidis Staph. SaprophyticusDocumento5 pagineStaph. Aureus Staph. Epidermidis Staph. SaprophyticusTom PedersonNessuna valutazione finora
- Neuro Written III TablesDocumento5 pagineNeuro Written III TablesSolomon Seth SallforsNessuna valutazione finora
- Salmonela Thyposa: Disease Etiology Unique S&S Brief Patophysiology Diagnostic Treatment / Plan OthersDocumento8 pagineSalmonela Thyposa: Disease Etiology Unique S&S Brief Patophysiology Diagnostic Treatment / Plan OthersNatalia_WiryantoNessuna valutazione finora
- Diseases Link To Chromosomal Abnormalities: Chromoso Me Abnormality DiseaseDocumento7 pagineDiseases Link To Chromosomal Abnormalities: Chromoso Me Abnormality Diseasenreena aslamNessuna valutazione finora
- Present at 4-12 Months, Development Arrest From Pre-B To BDocumento2 paginePresent at 4-12 Months, Development Arrest From Pre-B To BWaoNessuna valutazione finora
- 'Aliah's Cardiovascular SystemDocumento45 pagine'Aliah's Cardiovascular SystemLuqman Al-Bashir FauziNessuna valutazione finora
- Characterstic Drug ToxicitiesDocumento3 pagineCharacterstic Drug ToxicitiesJorge PalazzoloNessuna valutazione finora
- Board Review Blood SupplyDocumento6 pagineBoard Review Blood Supplynewguy927Nessuna valutazione finora
- Differential Diagnosis of Genital Ulcer Differential Diagnosis of Genital UlcersDocumento3 pagineDifferential Diagnosis of Genital Ulcer Differential Diagnosis of Genital UlcersNurhayati HasanahNessuna valutazione finora
- Precipitating Factors:: Myocardial Cell Death (NecrosisDocumento2 paginePrecipitating Factors:: Myocardial Cell Death (NecrosisLean Ashly MacarubboNessuna valutazione finora
- Clinical Medicine CVS Tabulated 2019Documento5 pagineClinical Medicine CVS Tabulated 2019Justin TayabanNessuna valutazione finora
- Im-Ugib PudDocumento6 pagineIm-Ugib PudTrisNessuna valutazione finora
- Poliomyelitis Haemophilus Influenzae Type B VariecellaDocumento4 paginePoliomyelitis Haemophilus Influenzae Type B VariecellaJeanna Chong100% (1)
- A Bunch of Pharm ShitDocumento2 pagineA Bunch of Pharm ShitkatNessuna valutazione finora
- Cardio Block 3Documento62 pagineCardio Block 3Maya LaPradeNessuna valutazione finora
- Hema Part 3 Final PDFDocumento188 pagineHema Part 3 Final PDFH.B.ANessuna valutazione finora
- Vasculitis: Disorder Vessels Pathology Presentation Test TX OtherDocumento3 pagineVasculitis: Disorder Vessels Pathology Presentation Test TX OthermcwnotesNessuna valutazione finora
- HEMATOLOGYDocumento36 pagineHEMATOLOGYMA. ANDREA NICOLE BITOINNessuna valutazione finora
- Antimycobacterial Drugs PDFDocumento3 pagineAntimycobacterial Drugs PDFCas BuNessuna valutazione finora
- CVR PharmacologyDocumento6 pagineCVR PharmacologyRebecca MarshallNessuna valutazione finora
- FUN1 Pharmacology TableDocumento10 pagineFUN1 Pharmacology TableRebecca MarshallNessuna valutazione finora
- Chemical Pathology Reference Range 2017Documento19 pagineChemical Pathology Reference Range 2017Shobana RaveendranNessuna valutazione finora
- Antivirals, Rubella, Peecorna VIRUSDocumento3 pagineAntivirals, Rubella, Peecorna VIRUSErnie G. Bautista II, RN, MDNessuna valutazione finora
- All Forms of Shock - Lactic Acid Via Tissue Hypoxia Tubulare Nec Via Coagulation in PT TALDocumento10 pagineAll Forms of Shock - Lactic Acid Via Tissue Hypoxia Tubulare Nec Via Coagulation in PT TALlynk787Nessuna valutazione finora
- Tumor Immunology: I. Common Tumor MarkersDocumento2 pagineTumor Immunology: I. Common Tumor MarkersDivineGloryMalbuyoNessuna valutazione finora
- Pharmacology TableDocumento9 paginePharmacology TableMaryam KhushbakhatNessuna valutazione finora
- Marrow Study PlannerDocumento2 pagineMarrow Study Plannerpooja singh50% (2)
- Handouts Integumentary Sys Sp11 B201Documento7 pagineHandouts Integumentary Sys Sp11 B201Kelly TrainorNessuna valutazione finora
- Pathogens of The Vagina-Annie Espinosa - This Is The Revised VersionDocumento1 paginaPathogens of The Vagina-Annie Espinosa - This Is The Revised VersionMicroposterNessuna valutazione finora
- Abg InterpretationDocumento1 paginaAbg InterpretationPrincess EspadaNessuna valutazione finora
- Toxicology USMLE NotesDocumento15 pagineToxicology USMLE NotesDuncan JacksonNessuna valutazione finora
- Klasifikasi Dan Mekanisme ABDocumento8 pagineKlasifikasi Dan Mekanisme ABDeboyjackNessuna valutazione finora
- The Better You Get at Something, The More Enjoyable It Can BecomeDocumento6 pagineThe Better You Get at Something, The More Enjoyable It Can BecomeAshNessuna valutazione finora
- Bacterial Virulence FactorsDocumento2 pagineBacterial Virulence FactorsJulia IshakNessuna valutazione finora
- Neuroscience Pre-Midterm Pathways: Fall 2012Documento46 pagineNeuroscience Pre-Midterm Pathways: Fall 2012Yezin ShamoonNessuna valutazione finora
- MC Tumor MC Ca MC 1° Ca BrainDocumento12 pagineMC Tumor MC Ca MC 1° Ca BrainRyan TurnerNessuna valutazione finora
- Electrolyte Imbalance Cause Signs and Symptoms Intervention ConnectionDocumento6 pagineElectrolyte Imbalance Cause Signs and Symptoms Intervention ConnectionmkninnyNessuna valutazione finora
- 4.1d - Pathology of The Pituitary - Nov.10 - Dr. GalangDocumento4 pagine4.1d - Pathology of The Pituitary - Nov.10 - Dr. GalangMiel Raphael AranillaNessuna valutazione finora
- Gastro ExamDocumento2 pagineGastro ExamJessica Brittain-GeorgeNessuna valutazione finora
- Neisseria Meningitidis Strep Pneumoniae E. ColiDocumento3 pagineNeisseria Meningitidis Strep Pneumoniae E. ColiÐr SalmaNessuna valutazione finora
- Gyneacology Revision by All TeamDocumento14 pagineGyneacology Revision by All TeamSara EhabNessuna valutazione finora
- Decreased Hemoglobin Available For Erythrocytes Microcytic, Hypochromic Anemia More Hemoglobin Available For Erythrocytes Macrocytic AnemiaDocumento2 pagineDecreased Hemoglobin Available For Erythrocytes Microcytic, Hypochromic Anemia More Hemoglobin Available For Erythrocytes Macrocytic AnemiaIB leaksNessuna valutazione finora
- Abnormal LFTsDocumento2 pagineAbnormal LFTsRenu RosyNessuna valutazione finora
- NSAID's "Non-Steroidal Anti-Inflammatory Drugs": Mmbakhaitan@uqu - Edu.saDocumento19 pagineNSAID's "Non-Steroidal Anti-Inflammatory Drugs": Mmbakhaitan@uqu - Edu.saAhmed HossamNessuna valutazione finora
- Review For The 2° Semester Exam Alessandro Mo6a, UVVG, 3 YearDocumento9 pagineReview For The 2° Semester Exam Alessandro Mo6a, UVVG, 3 Yeardjxela89Nessuna valutazione finora
- Patho CA - Acute PancreatitisDocumento1 paginaPatho CA - Acute PancreatitisKNessuna valutazione finora
- Internal Medicine Quick TablesDocumento276 pagineInternal Medicine Quick Tablesjoey plouffeNessuna valutazione finora
- Source Hormone Major Action: Adrenal CortexDocumento3 pagineSource Hormone Major Action: Adrenal CortexReisha FungoNessuna valutazione finora
- Bam Slam Drug CardDocumento4 pagineBam Slam Drug CardLeticia GonzalezNessuna valutazione finora
- Intracellular AccumulationsDocumento3 pagineIntracellular AccumulationsSean MatthewNessuna valutazione finora
- 4 Intracellular AccumulationsDocumento24 pagine4 Intracellular AccumulationsReetu BaralNessuna valutazione finora
- An Introduction To NutritionDocumento17 pagineAn Introduction To NutritionAlejandra Diaz RojasNessuna valutazione finora
- The History of Immunology and VaccinesDocumento32 pagineThe History of Immunology and VaccinesClement del RosarioNessuna valutazione finora
- The Accidental AddictsDocumento6 pagineThe Accidental AddictsnorthandsouthnzNessuna valutazione finora
- Innate ImmunityDocumento43 pagineInnate ImmunityhunarsandhuNessuna valutazione finora
- Volkan GurelDocumento5 pagineVolkan Gurelapi-392209800Nessuna valutazione finora
- Welcome To The Celestial Biolabs LimitedDocumento8 pagineWelcome To The Celestial Biolabs LimitedsaahilsinghiNessuna valutazione finora
- Proposal For Defense Group 3Documento77 pagineProposal For Defense Group 3Kristiene Kyle AquinoNessuna valutazione finora
- Cancer Fighting StrategiesDocumento6 pagineCancer Fighting StrategiesDahneel RehfahelNessuna valutazione finora
- Dattatray Et Al. - 1970 - A Comprehensive Review On Polyalthia LongifoliaDocumento24 pagineDattatray Et Al. - 1970 - A Comprehensive Review On Polyalthia LongifoliaCauridasNessuna valutazione finora
- Dr. Syed Shakeel Ahmad: ObjectiveDocumento3 pagineDr. Syed Shakeel Ahmad: ObjectiveSyed Shakeel AhmadNessuna valutazione finora
- Morning Report: Supervisor: Dr. Rusdhy A.H., SP - OG Medical StudentsDocumento8 pagineMorning Report: Supervisor: Dr. Rusdhy A.H., SP - OG Medical StudentsEra MoetzNessuna valutazione finora
- Hybrid Hues 2008Documento196 pagineHybrid Hues 2008Kulsharma100% (1)
- Diuretics Antidiabetics AnalgesicsDocumento7 pagineDiuretics Antidiabetics AnalgesicsBillQueNessuna valutazione finora
- Template For Care Plan AssignmentDocumento8 pagineTemplate For Care Plan AssignmentAnn OgoloNessuna valutazione finora
- Pcog Notes (Alkaloids II)Documento4 paginePcog Notes (Alkaloids II)sadburgerNessuna valutazione finora
- Ancondroplasia DwarfismDocumento10 pagineAncondroplasia DwarfismjordandeanNessuna valutazione finora
- PSM 2 PypDocumento186 paginePSM 2 PypsuriNessuna valutazione finora
- Skin Cancers Risk Factors, Prevention and TherapyDocumento281 pagineSkin Cancers Risk Factors, Prevention and Therapyellibrero1972Nessuna valutazione finora
- Chapter II - Bodies of Fire - The Accupuncture MeridiansDocumento41 pagineChapter II - Bodies of Fire - The Accupuncture MeridiansScott Canter100% (1)
- Felicias Resume 1Documento1 paginaFelicias Resume 1api-357153848Nessuna valutazione finora
- Consulta de MedicamentosDocumento39 pagineConsulta de MedicamentosJhonWainerLopezNessuna valutazione finora
- Procedure For Penicillin Skin TestingDocumento4 pagineProcedure For Penicillin Skin TestingHarshan Isuru KumaraNessuna valutazione finora
- Mobicare BrochureDocumento4 pagineMobicare Brochuremicrobotica126Nessuna valutazione finora
- RNI For Malaysians-SummaryDocumento2 pagineRNI For Malaysians-SummaryAimi Hannani100% (1)
- MCQ Pead MockDocumento8 pagineMCQ Pead MocknoblefxNessuna valutazione finora
- 2018121184950 - نشرة الخريجين 2017777 PDFDocumento389 pagine2018121184950 - نشرة الخريجين 2017777 PDFIslam ElnabaNessuna valutazione finora
- Sri Lanka NMRA GazetteDocumento9 pagineSri Lanka NMRA GazetteSanjeev JayaratnaNessuna valutazione finora
- Tracheostomy Tube Brochure - 086034Documento4 pagineTracheostomy Tube Brochure - 086034adelin litanNessuna valutazione finora