Potrebbero piacerti anche
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5795)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1091)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
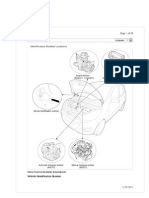
- I10 Workshop Manual - ADocumento292 pagineI10 Workshop Manual - ANorthstartechnology Company82% (11)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (74)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- Hypochondriasis and Health Anxiety - A Guide For Clinicians (PDFDrive)Documento289 pagineHypochondriasis and Health Anxiety - A Guide For Clinicians (PDFDrive)Fernanda SilvaNessuna valutazione finora
- Amendment No. 2 To AS 2047-2014 Windows and External Glazed Doors in BuildingsDocumento2 pagineAmendment No. 2 To AS 2047-2014 Windows and External Glazed Doors in BuildingsTommy AndersNessuna valutazione finora
- PDF Download Before You Say I Do A Marriage Preparation Manual For CouplesDocumento2 paginePDF Download Before You Say I Do A Marriage Preparation Manual For CouplesKevin EdroNessuna valutazione finora
- Fagor CNC 8025 - 8030Documento255 pagineFagor CNC 8025 - 8030alvhann_1Nessuna valutazione finora
- 6.m.tech-Ece-Vlsi, Vlsi Systems, Vlsi System Design (Vlsi, Vlsis, Vlsisd) r17 Course Structure & SyllabiDocumento35 pagine6.m.tech-Ece-Vlsi, Vlsi Systems, Vlsi System Design (Vlsi, Vlsis, Vlsisd) r17 Course Structure & SyllabiravibabukancharlaNessuna valutazione finora
- Case Study Oil and Gas - PowerpointDocumento8 pagineCase Study Oil and Gas - PowerpointYaxssNessuna valutazione finora
- s1042368008000053 PDFDocumento14 pagines1042368008000053 PDFKevin EdroNessuna valutazione finora
- Magnetic Resonance Imaging of Meningiomas: A Pictorial ReviewDocumento10 pagineMagnetic Resonance Imaging of Meningiomas: A Pictorial ReviewKevin EdroNessuna valutazione finora
- s104236800800003x PDFDocumento21 pagines104236800800003x PDFKevin EdroNessuna valutazione finora
- Decoding The Epigenetic Code For Cardiovascular RegeneratioDocumento1 paginaDecoding The Epigenetic Code For Cardiovascular RegeneratioKevin EdroNessuna valutazione finora
- Tinea BarbaeDocumento4 pagineTinea BarbaeKevin EdroNessuna valutazione finora
- Tatalaksana ACS HUT Harkit 2015 - 1 PDFDocumento35 pagineTatalaksana ACS HUT Harkit 2015 - 1 PDFKevin EdroNessuna valutazione finora
- INFORMATION SHEET No. 1.1.1Documento7 pagineINFORMATION SHEET No. 1.1.1Sandre Walden-SCSCNessuna valutazione finora
- MultiCrystallineDataSheet - EN - SilikenDocumento4 pagineMultiCrystallineDataSheet - EN - Silikensydneyaus2005Nessuna valutazione finora
- MCQ Rewriting 1Documento10 pagineMCQ Rewriting 1Quỳnh Anh NguyễnNessuna valutazione finora
- Run Omega Run Lunar Omegaverse Book 5 Shyla Colt All ChapterDocumento52 pagineRun Omega Run Lunar Omegaverse Book 5 Shyla Colt All Chapterkate.brown975100% (6)
- Critical Thinking and It's Importance in Education: I. Lenin Assistant Professor Auce KaraikudiDocumento5 pagineCritical Thinking and It's Importance in Education: I. Lenin Assistant Professor Auce KaraikudiPABLO RAMIRO AGUILAR GONZALEZNessuna valutazione finora
- Afm Udc A320-500Documento600 pagineAfm Udc A320-500melitiyaprorok100% (1)
- Design, Fabrication and Analysis of Fibonacci TurbineDocumento5 pagineDesign, Fabrication and Analysis of Fibonacci TurbinearcaldartNessuna valutazione finora
- Foods 09 01560 PDFDocumento10 pagineFoods 09 01560 PDFkim cheNessuna valutazione finora
- hw10 PDFDocumento10 paginehw10 PDFTahok24Nessuna valutazione finora
- The CyclotronDocumento10 pagineThe CyclotronSupriya DuttaNessuna valutazione finora
- Kyocera 1800Documento2 pagineKyocera 1800gendoetzNessuna valutazione finora
- Devi Narayaneeyam - Dasakam 9 Bhuvaneswari Darsanam - Seeing of BhuvaneswariDocumento7 pagineDevi Narayaneeyam - Dasakam 9 Bhuvaneswari Darsanam - Seeing of BhuvaneswaribrindaNessuna valutazione finora
- 1-Theory of Metal Cutting PDFDocumento144 pagine1-Theory of Metal Cutting PDFNithinArvindNessuna valutazione finora
- The Physiology of Potassium in Crop Production PDFDocumento31 pagineThe Physiology of Potassium in Crop Production PDFFelipe R. Parada100% (1)
- Asms 02 0033Documento6 pagineAsms 02 0033Delfia AkiharyNessuna valutazione finora
- SpiralsDocumento12 pagineSpiralskkglobalNessuna valutazione finora
- Divine Child International School, Adalaj Revision Worksheet Grade 6, Maths Choose The Correct OptionDocumento2 pagineDivine Child International School, Adalaj Revision Worksheet Grade 6, Maths Choose The Correct OptionNatasha VidhaniNessuna valutazione finora
- Animal Whisperer PDFDocumento4 pagineAnimal Whisperer PDFKevinPriestmanNessuna valutazione finora
- Manual Placa Mae Ga 945gcmx-s2 6.6Documento72 pagineManual Placa Mae Ga 945gcmx-s2 6.6luisb3toNessuna valutazione finora
- Geo-Technical Investigation On Black Cotton Soils: GeotechnicalinvestigationonblackcottonsoilsDocumento5 pagineGeo-Technical Investigation On Black Cotton Soils: GeotechnicalinvestigationonblackcottonsoilsDevendrasinh PadhiyarNessuna valutazione finora
- Gen Math DianaDocumento5 pagineGen Math DianaDon Marlon BuquisNessuna valutazione finora
- Material Control Procedure - TemplateDocumento5 pagineMaterial Control Procedure - TemplateHernandito Rahmat KusumaNessuna valutazione finora
- Vol 2 No S12022 Actasdela XVIIConferencia Mundialsobre CineantropometraDocumento185 pagineVol 2 No S12022 Actasdela XVIIConferencia Mundialsobre CineantropometraAye JaimeNessuna valutazione finora
- Catálogo DP InglêsDocumento20 pagineCatálogo DP Inglêsjf2003Nessuna valutazione finora