Potrebbero piacerti anche
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (120)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (73)
- Medical Design GuideDocumento650 pagineMedical Design GuideStipe VučetićNessuna valutazione finora
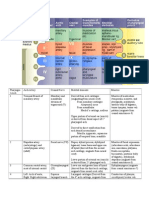
- Pharyngeal Arch Derivatives Chart!Documento5 paginePharyngeal Arch Derivatives Chart!Suphadetch Leung100% (1)
- Health Care AgenciesDocumento15 pagineHealth Care AgencieshemihemaNessuna valutazione finora
- Breech PresentationDocumento15 pagineBreech Presentationapi-3705046100% (2)
- Schwartz UrologyDocumento10 pagineSchwartz UrologyRem Alfelor100% (1)
- Transurethral Resection of The ProstateDocumento48 pagineTransurethral Resection of The Prostateralf_dolanNessuna valutazione finora
- BIR Tin Application (Form 1902)Documento2 pagineBIR Tin Application (Form 1902)Mara Martinez74% (27)
- Essential Newborn CareDocumento8 pagineEssential Newborn CareAnnapurna Dangeti100% (1)
- Breech DeliveryDocumento6 pagineBreech DeliveryNyoman TapayanaNessuna valutazione finora
- Set1 - Final FRCA Viva Qs - June 2009 PDFDocumento25 pagineSet1 - Final FRCA Viva Qs - June 2009 PDFAdham SalemNessuna valutazione finora
- Great Plan PDFDocumento136 pagineGreat Plan PDFLucy PevensieNessuna valutazione finora
- Staffing PatternDocumento19 pagineStaffing PatternJenny-Ann Baliday100% (3)
- Blood and Blood Components-LectureDocumento13 pagineBlood and Blood Components-LectureMelissa GinesNessuna valutazione finora
- Neonatal Jaundice ThresholdsDocumento9 pagineNeonatal Jaundice ThresholdsMariemma TipianiNessuna valutazione finora
- Hyatt Vs Goldstar ElevatorsDocumento4 pagineHyatt Vs Goldstar ElevatorsMjay GuintoNessuna valutazione finora
- Somportex Limited v. Philadelphia Chewing Gum Corporation, Appellant, v. Brewster, Leeds & Co., Inc. and M. S. International, Inc.Documento15 pagineSomportex Limited v. Philadelphia Chewing Gum Corporation, Appellant, v. Brewster, Leeds & Co., Inc. and M. S. International, Inc.Mjay GuintoNessuna valutazione finora
- Philippine Aluminum Wheels vs. FASGI EnterprisesDocumento6 paginePhilippine Aluminum Wheels vs. FASGI EnterprisesMjay GuintoNessuna valutazione finora
- Roehr Vs RodriguezDocumento4 pagineRoehr Vs RodriguezMjay GuintoNessuna valutazione finora
- Melton v. Stephens, 13 N.E.3d 533 (2014)Documento11 pagineMelton v. Stephens, 13 N.E.3d 533 (2014)Mjay GuintoNessuna valutazione finora
- Saudi Arabian Airlines Vs CADocumento3 pagineSaudi Arabian Airlines Vs CAMjay GuintoNessuna valutazione finora
- Bohanan vs. BohananDocumento2 pagineBohanan vs. BohananMjay GuintoNessuna valutazione finora
- Fujiki Vs MarinayDocumento5 pagineFujiki Vs MarinayMjay GuintoNessuna valutazione finora
- Hasegawa vs. KitamuraDocumento3 pagineHasegawa vs. KitamuraMjay GuintoNessuna valutazione finora
- Dowis v. Mud Slingers, Inc.Documento7 pagineDowis v. Mud Slingers, Inc.Mjay GuintoNessuna valutazione finora
- First National Bank Vs RostekDocumento10 pagineFirst National Bank Vs RostekMjay GuintoNessuna valutazione finora
- Safari - 25 Mar 2019 at 3:45 PMDocumento1 paginaSafari - 25 Mar 2019 at 3:45 PMCollen Mitzi BaguilodNessuna valutazione finora
- Futureselect V. Tremont Group Holdings: View Case Cited Cases Citing CaseDocumento8 pagineFutureselect V. Tremont Group Holdings: View Case Cited Cases Citing CaseMjay GuintoNessuna valutazione finora
- Cargill Inc v. Intra StrataDocumento3 pagineCargill Inc v. Intra StrataMjay GuintoNessuna valutazione finora
- Sistoza vs. DisiertoDocumento10 pagineSistoza vs. DisiertoMjay GuintoNessuna valutazione finora
- Castilex Case - G.R. No. 132266 PDFDocumento6 pagineCastilex Case - G.R. No. 132266 PDFMjay GuintoNessuna valutazione finora
- Evidence Legal Ethics Civil ProcedureDocumento1 paginaEvidence Legal Ethics Civil ProcedureMjay GuintoNessuna valutazione finora
- What's New: iOS 13 Dark Side UpdateDocumento5 pagineWhat's New: iOS 13 Dark Side Updatedias nurul windiNessuna valutazione finora
- G.R. No. 165338 and 179375 - Mahinay v. Lee GakoDocumento27 pagineG.R. No. 165338 and 179375 - Mahinay v. Lee GakoMjay GuintoNessuna valutazione finora
- 21st ANAK PUP Congress ProgrammeDocumento2 pagine21st ANAK PUP Congress ProgrammeMjay GuintoNessuna valutazione finora
- Stand Up Lts Letter For OrgsDocumento2 pagineStand Up Lts Letter For OrgsMjay GuintoNessuna valutazione finora
- Civ Pro CasesDocumento14 pagineCiv Pro CasesMjay GuintoNessuna valutazione finora
- G.R. No. 223399 - Fuerto v. EnsomoDocumento10 pagineG.R. No. 223399 - Fuerto v. EnsomoMjay GuintoNessuna valutazione finora
- Where There Is No MotionDocumento1 paginaWhere There Is No MotionMjay GuintoNessuna valutazione finora
- Safari - 16 May 2019 at 12:17 PMDocumento1 paginaSafari - 16 May 2019 at 12:17 PMMjay GuintoNessuna valutazione finora
- Safari - 31 May 2019 at 12:16 AMDocumento1 paginaSafari - 31 May 2019 at 12:16 AMMjay GuintoNessuna valutazione finora
- Safari - 25 Mar 2019 at 8:06 PMDocumento1 paginaSafari - 25 Mar 2019 at 8:06 PMMjay GuintoNessuna valutazione finora
- Case Digest Agra: DownloadDocumento1 paginaCase Digest Agra: DownloadMjay GuintoNessuna valutazione finora
- Agrarian Law Digests: DownloadDocumento1 paginaAgrarian Law Digests: DownloadMjay GuintoNessuna valutazione finora
- Third - Schedule Notified PDFDocumento144 pagineThird - Schedule Notified PDFinam khanNessuna valutazione finora
- Internship ReportDocumento39 pagineInternship ReportHappy Sunshine50% (2)
- Hdi BDDocumento22 pagineHdi BDAjker PaychalNessuna valutazione finora
- Terapi Pijat English PDFDocumento6 pagineTerapi Pijat English PDFari dwiNessuna valutazione finora
- Company ProfileDocumento3 pagineCompany ProfileMichael Dimayuga100% (2)
- CIS Self-Study Lesson Plans: Surgical Instrumentation For Gynecological ProceduresDocumento3 pagineCIS Self-Study Lesson Plans: Surgical Instrumentation For Gynecological Proceduresjerimiah_manzonNessuna valutazione finora
- Brier Ley 2020Documento8 pagineBrier Ley 2020kemoNessuna valutazione finora
- Application For Registration Licence Renewal of Registration and Licence Under Sections 7 and 8 of The Sikkim Clinical Establishments Act. 1995Documento2 pagineApplication For Registration Licence Renewal of Registration and Licence Under Sections 7 and 8 of The Sikkim Clinical Establishments Act. 1995kabuldasNessuna valutazione finora
- Acute Angle-Closure Glaucoma (AACG)Documento11 pagineAcute Angle-Closure Glaucoma (AACG)Intan AliNessuna valutazione finora
- Facts and Definition of EclampsiaDocumento5 pagineFacts and Definition of EclampsiaChoi Gong JuNessuna valutazione finora
- StainsDocumento4 pagineStainsManikanta Chaitanya LokanadhamNessuna valutazione finora
- Case Study 55-3Documento5 pagineCase Study 55-3jillNessuna valutazione finora
- Medschool AnestheticsDocumento4 pagineMedschool AnestheticsJustin HulinNessuna valutazione finora
- Makalah Plendis Blok 24Documento23 pagineMakalah Plendis Blok 24Alvian RamadyaNessuna valutazione finora
- Hordeolum and Chalazion TreatmentDocumento3 pagineHordeolum and Chalazion TreatmentJessica AngelinaNessuna valutazione finora
- National Vital Statistics ReportsDocumento15 pagineNational Vital Statistics ReportssunnewsNessuna valutazione finora
- Croatian Society of Radiology (1928-2008)Documento12 pagineCroatian Society of Radiology (1928-2008)Anonymous 9QxPDpNessuna valutazione finora