Potrebbero piacerti anche
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5795)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (74)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- Decoding The Flu: Modified From A Case Study byDocumento7 pagineDecoding The Flu: Modified From A Case Study byStanleyWu0% (1)
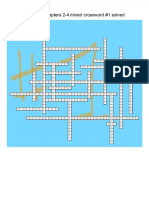
- CHAPTERS 2-4 CROSSWORD #1 SolvedDocumento4 pagineCHAPTERS 2-4 CROSSWORD #1 SolvedYu LucyNessuna valutazione finora
- Chapter 15Documento15 pagineChapter 15nfnf otupyooorefnNessuna valutazione finora
- Otagiri, 2016. Albumin in Medicine. EBOOKDocumento279 pagineOtagiri, 2016. Albumin in Medicine. EBOOKFinda Istiqomah100% (1)
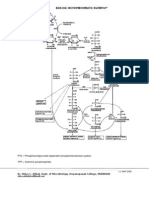
- Hexose Monophosphate Pathway PathwayDocumento3 pagineHexose Monophosphate Pathway PathwayShiva100% (6)
- BIOL2262 Assignment Sheet 2 - 2013Documento2 pagineBIOL2262 Assignment Sheet 2 - 2013Melissa T100% (1)
- General Biology Lab Manual - F2016 PDFDocumento114 pagineGeneral Biology Lab Manual - F2016 PDFDuncan ComptonNessuna valutazione finora
- AFLP Manual InvitrogenDocumento24 pagineAFLP Manual InvitrogenJanani SNessuna valutazione finora
- 1 s2.0 S0022282816302176 MainDocumento85 pagine1 s2.0 S0022282816302176 MainNia Rukman100% (1)
- Natural Science. Level 6. Unit 3. ReproductionDocumento3 pagineNatural Science. Level 6. Unit 3. ReproductionAna Rosa Camacho Cornejo50% (2)
- Pablo Borbon Main II Batangas City: Republic of The Philippines Batangas State UniversityDocumento5 paginePablo Borbon Main II Batangas City: Republic of The Philippines Batangas State UniversityChichiri NomiNessuna valutazione finora
- Circadian Rhythm NEJMDocumento12 pagineCircadian Rhythm NEJMtjelongNessuna valutazione finora
- Hatching and BroodingDocumento22 pagineHatching and BroodingToha PutraNessuna valutazione finora
- HURDCO International School: Subject-Biology Chapter 3: Diffusion, Osmosis and Surface Area: Volume RatioDocumento26 pagineHURDCO International School: Subject-Biology Chapter 3: Diffusion, Osmosis and Surface Area: Volume RatioMahin IslamNessuna valutazione finora
- Dna ExtractionDocumento5 pagineDna ExtractionYsabel Francesca AbadNessuna valutazione finora
- Department of Animal Husbandry and Dairy Science Mahatma Phule Krishi Vidyapeeth Rahuri-413 722, Dist. Ahmednagar (MS)Documento20 pagineDepartment of Animal Husbandry and Dairy Science Mahatma Phule Krishi Vidyapeeth Rahuri-413 722, Dist. Ahmednagar (MS)dahiphale1100% (1)
- Human - Influences - On - Ecosystems - 4 QPDocumento5 pagineHuman - Influences - On - Ecosystems - 4 QPkatise1794Nessuna valutazione finora
- Artículo: Marzolo Et Al. (1997) PNASDocumento6 pagineArtículo: Marzolo Et Al. (1997) PNASConsue HAPPYNessuna valutazione finora
- Crop LifeDocumento7 pagineCrop Life유가연[학생](생명과학대학 유전생명공학과)Nessuna valutazione finora
- HACCPtestDocumento13 pagineHACCPtestDianne Faye ManabatNessuna valutazione finora
- Cacti Biology and Uses (2003) BBSDocumento291 pagineCacti Biology and Uses (2003) BBSAadolfo MUNessuna valutazione finora
- CV Margaret Durdan 17-18Documento3 pagineCV Margaret Durdan 17-18api-428498175Nessuna valutazione finora
- Pre 2010 Part 2Documento527 paginePre 2010 Part 2Fábio CostaNessuna valutazione finora
- Project Manager Biotech Pharmaceutical Healthcare in Boston MA Resume Katinka SteniusDocumento3 pagineProject Manager Biotech Pharmaceutical Healthcare in Boston MA Resume Katinka SteniusKatinkaSteniusNessuna valutazione finora
- Exome Sequencing AnalysisDocumento7 pagineExome Sequencing AnalysisSalman khanNessuna valutazione finora
- Tryptic Soy Agar (7100) : Formula May Be Adjusted And/or Supplemented As Required To Meet Performance SpecificationsDocumento3 pagineTryptic Soy Agar (7100) : Formula May Be Adjusted And/or Supplemented As Required To Meet Performance SpecificationsMulyani Dwi YantiNessuna valutazione finora
- The Past, Present and Future of NeuroplasticityDocumento13 pagineThe Past, Present and Future of NeuroplasticityMaxime Goovaerts100% (3)
- Experiment 3 Bio300Documento5 pagineExperiment 3 Bio300ellymanisNessuna valutazione finora
- Gen Bio Ref1 PDFDocumento25 pagineGen Bio Ref1 PDFGexel Cecilio78% (9)
- OCD Mast Cell Herbal ProtocolDocumento5 pagineOCD Mast Cell Herbal ProtocolIvana CiricNessuna valutazione finora