Potrebbero piacerti anche
- KinderDocumento1 paginaKinderCynthia Candilosa RevillaNessuna valutazione finora
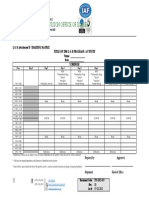
- FM HRD 005 Attachment D. Training MatrixDocumento1 paginaFM HRD 005 Attachment D. Training Matrixchrystal reignNessuna valutazione finora
- ACLC Department Faculty Plotting Form 2019 2020 FORMATDocumento14 pagineACLC Department Faculty Plotting Form 2019 2020 FORMATCathy GaveroNessuna valutazione finora
- Time LogDocumento2 pagineTime LogBhavya NathNessuna valutazione finora
- 5 FM-HRD-005-Attachment-D.-Training-MatrixDocumento1 pagina5 FM-HRD-005-Attachment-D.-Training-MatrixJoemar Vincent SerranoNessuna valutazione finora
- Ead536 NtipDocumento9 pagineEad536 Ntipapi-340158465Nessuna valutazione finora
- School Year Master ScheduleDocumento4 pagineSchool Year Master ScheduleMelanie AplacaNessuna valutazione finora
- Experiential Teambuilding ProgramDocumento27 pagineExperiential Teambuilding ProgramRizal de silvaNessuna valutazione finora
- Ssaa AdDocumento5 pagineSsaa AdJoshua AseritNessuna valutazione finora
- Narrative ReportDocumento2 pagineNarrative ReportMonique G. TagabanNessuna valutazione finora
- Jurnal Guru 2020-2021Documento2 pagineJurnal Guru 2020-2021bayu segoroNessuna valutazione finora
- Fa Q ParticipantDocumento6 pagineFa Q Participantrahulo280197Nessuna valutazione finora
- Training/meeting/workshop Title and Venue Logo (Image) : Start Date and Time Day Day 1, 2, 3 EtcDocumento2 pagineTraining/meeting/workshop Title and Venue Logo (Image) : Start Date and Time Day Day 1, 2, 3 EtcNega TewoldeNessuna valutazione finora
- Block Schedule UNCW HoursDocumento2 pagineBlock Schedule UNCW HoursFrancisco BrignoleNessuna valutazione finora
- Daily Behavior Chart: Choose Prize If You Only Get 1 in The A.M. Choose Prize If You Only Get 1 in The P.MDocumento2 pagineDaily Behavior Chart: Choose Prize If You Only Get 1 in The A.M. Choose Prize If You Only Get 1 in The P.MRRKATANessuna valutazione finora
- Student Spiritual Retreat CancelledDocumento4 pagineStudent Spiritual Retreat CancelledLuhut GultomNessuna valutazione finora
- Leadership Taining Project Proposal - 071224Documento5 pagineLeadership Taining Project Proposal - 071224Balleras Xykan FeridoNessuna valutazione finora
- Time Tracker Guide: Wih Nikki Kinzer, PCCDocumento7 pagineTime Tracker Guide: Wih Nikki Kinzer, PCCPsydocNessuna valutazione finora
- Instructor Subject Monitoring: Philippiine College of TechnologyDocumento2 pagineInstructor Subject Monitoring: Philippiine College of TechnologyRonald SuritaNessuna valutazione finora
- Activity Matrix On RPMS ReOrientation - DistrictDocumento2 pagineActivity Matrix On RPMS ReOrientation - Districtrey yuyNessuna valutazione finora
- Master Schedule 2017-2018Documento2 pagineMaster Schedule 2017-2018api-367711385Nessuna valutazione finora
- Bell Schedules, Sessions and Webinar Links 2nd Round of Training Webinars...Documento2 pagineBell Schedules, Sessions and Webinar Links 2nd Round of Training Webinars...Corey ColeNessuna valutazione finora
- Matrix 2d RPMS Re-EchoDocumento1 paginaMatrix 2d RPMS Re-EchoFhebe S. SelorioNessuna valutazione finora
- Ffad Program and Waiver 1Documento1 paginaFfad Program and Waiver 1Le Claire SanglayNessuna valutazione finora
- BGDES October 31 Accomplishment ReportDocumento2 pagineBGDES October 31 Accomplishment ReportralpdulayliboonNessuna valutazione finora
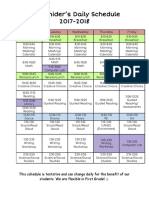
- Miss Dawson Schedule 2017-18Documento2 pagineMiss Dawson Schedule 2017-18api-299063948Nessuna valutazione finora
- Cream Brown Simple Aesthetic Paper BorderDocumento6 pagineCream Brown Simple Aesthetic Paper BorderNikka StellaNessuna valutazione finora
- Daily Planner Sheet Page 1Documento1 paginaDaily Planner Sheet Page 1Tina Carol EisenbraunNessuna valutazione finora
- Transform Your Life at LifePlugin's Personal Growth FestivalDocumento21 pagineTransform Your Life at LifePlugin's Personal Growth FestivalRohit KumarNessuna valutazione finora
- Boot Camp ProgramDocumento1 paginaBoot Camp ProgrambernardNessuna valutazione finora
- Pc101 Document w06ApplicationActivityTemplateDocumento4 paginePc101 Document w06ApplicationActivityTemplateLucas GomezNessuna valutazione finora
- Division Memorandum No. 80, S. 2022Documento9 pagineDivision Memorandum No. 80, S. 2022Aniver VergaraNessuna valutazione finora
- Training Design - SWA DRRM CampDocumento2 pagineTraining Design - SWA DRRM CampIsaias BigolNessuna valutazione finora
- WIS College Student HandbookDocumento16 pagineWIS College Student HandbookRyan Llona FernandezNessuna valutazione finora
- 31st Buklod Atenista Program (May 2014)Documento2 pagine31st Buklod Atenista Program (May 2014)Buklod AtenistaNessuna valutazione finora
- Ultimate Homeschool PlannerDocumento16 pagineUltimate Homeschool PlannerSilvana BocaNessuna valutazione finora
- Soal UAS RegresiDocumento22 pagineSoal UAS RegresialfianadewiNessuna valutazione finora
- 1b Guidelines in Conducting CCW OnlineDocumento5 pagine1b Guidelines in Conducting CCW OnlineSTEVE JHONSON LepasanaNessuna valutazione finora
- Proposed Time ScheduleDocumento1 paginaProposed Time ScheduleRoel P. Dolaypan Jr.Nessuna valutazione finora
- May 2019 Capacity Building Conference AgendaDocumento2 pagineMay 2019 Capacity Building Conference AgendaJanysse CalderonNessuna valutazione finora
- The City School: University Road CampusDocumento1 paginaThe City School: University Road CampusImama AamirNessuna valutazione finora
- Kindergarten Blocks of Time TemplateDocumento9 pagineKindergarten Blocks of Time TemplateFaye Dusayen - EsclamadoNessuna valutazione finora
- Sample of Marketing ProposalDocumento8 pagineSample of Marketing Proposalfaris fauziNessuna valutazione finora
- Jurnal PKLDocumento2 pagineJurnal PKLFerdinan Yuli SetiawanNessuna valutazione finora
- DTR March 2023Documento2 pagineDTR March 2023Sheila Mauricio GarciaNessuna valutazione finora
- CENTILE 2017 AgendaDocumento1 paginaCENTILE 2017 AgendacharliekonsorNessuna valutazione finora
- Daily Planner Template 12Documento1 paginaDaily Planner Template 12MurthyNessuna valutazione finora
- Teacher'S Daily Schedule: Grade: Sped Transition-Aquino Enrolment Male: 12 Female: 4 Total: 16 S.Y.: 2020 - 2021Documento2 pagineTeacher'S Daily Schedule: Grade: Sped Transition-Aquino Enrolment Male: 12 Female: 4 Total: 16 S.Y.: 2020 - 2021Gillian Bollozos-CabuguasNessuna valutazione finora
- Classroom Program SY 2022 2023 updatedMEWDocumento13 pagineClassroom Program SY 2022 2023 updatedMEWjenisaNessuna valutazione finora
- Civil Service Form No. 48 Daily Time Record Civil Service Form No. 48 Daily Time RecordDocumento2 pagineCivil Service Form No. 48 Daily Time Record Civil Service Form No. 48 Daily Time RecordClinth Jhon ColanceNessuna valutazione finora
- Weekly Home Learning Plan 0208 0212Documento4 pagineWeekly Home Learning Plan 0208 0212April Joy LascuñaNessuna valutazione finora
- LDBD Labor Day Virtual Camp Permission Slip 2020Documento5 pagineLDBD Labor Day Virtual Camp Permission Slip 2020EvelynNessuna valutazione finora
- ReportffsfsDocumento4 pagineReportffsfshemantpandyanbhNessuna valutazione finora
- Sample CPD Plan For SchoolsDocumento8 pagineSample CPD Plan For SchoolsShamsil ArifeenNessuna valutazione finora
- 1a Guidelines in Conducting COW OnlineDocumento6 pagine1a Guidelines in Conducting COW OnlineEricaNessuna valutazione finora
- Non Verbal and Use of AVADocumento34 pagineNon Verbal and Use of AVAefa yustinaNessuna valutazione finora
- Updated 2020-2021 Foothill High School Remote Learning Bell ScheduleDocumento2 pagineUpdated 2020-2021 Foothill High School Remote Learning Bell ScheduleMatthew TahirNessuna valutazione finora
- Class ProgramDocumento1 paginaClass ProgramMaridel Stephanie QuirosNessuna valutazione finora
- Lincoln Portfolio Autumn Bybee ED 434:01 April 3, 2017Documento28 pagineLincoln Portfolio Autumn Bybee ED 434:01 April 3, 2017api-360778580Nessuna valutazione finora
- Kolk-2006-Annals of The New York Academy of SciencesDocumento17 pagineKolk-2006-Annals of The New York Academy of Sciencesapi-420206789Nessuna valutazione finora
- Practitioners GuideDocumento5 paginePractitioners GuideNarina Avi SeptiyantiNessuna valutazione finora
- CrisisassessmentformsDocumento6 pagineCrisisassessmentformsapi-420206789Nessuna valutazione finora
- cns739 QuicktipshandoutDocumento1 paginacns739 Quicktipshandoutapi-420206789Nessuna valutazione finora
- Do A Client MapDocumento1 paginaDo A Client Mapapi-420206789Nessuna valutazione finora
- Maddie Sell ResumeDocumento2 pagineMaddie Sell Resumeapi-420206789Nessuna valutazione finora
- Adult Standard Biopsychosocial TemplateDocumento11 pagineAdult Standard Biopsychosocial Templateapi-404660807Nessuna valutazione finora
- Madeline Sell PdsDocumento2 pagineMadeline Sell Pdsapi-420206789Nessuna valutazione finora
- S32 Design Studio 3.1: NXP SemiconductorsDocumento9 pagineS32 Design Studio 3.1: NXP SemiconductorsThành Chu BáNessuna valutazione finora
- 1 PDFDocumento14 pagine1 PDFPM JFNessuna valutazione finora
- Vocabulary Prefixes ExercisesDocumento2 pagineVocabulary Prefixes ExercisesMarina García CarrascoNessuna valutazione finora
- Upsized To 12 Gallon Still On A 36"x56" Sheet: Pint O Shine's 6 Gallon Pot Still Design and TemplateDocumento50 pagineUpsized To 12 Gallon Still On A 36"x56" Sheet: Pint O Shine's 6 Gallon Pot Still Design and TemplateyamyrulesNessuna valutazione finora
- Advance Control Systems LabDocumento2 pagineAdvance Control Systems Labpadmajasiva100% (1)
- Group 7 Scope StatementDocumento17 pagineGroup 7 Scope Statementapi-335995226100% (4)
- English Class Language DevicesDocumento56 pagineEnglish Class Language DevicesKAREN GREGANDANessuna valutazione finora
- Outgoing Call Block BroadcastReceiver ExampleDocumento3 pagineOutgoing Call Block BroadcastReceiver ExampleZainUlAbidinNessuna valutazione finora
- STAR Worksheet Interviewing SkillsDocumento1 paginaSTAR Worksheet Interviewing SkillsCharity WacekeNessuna valutazione finora
- Factors That Affect Information and Communication Technology Usage: A Case Study in Management EducationDocumento20 pagineFactors That Affect Information and Communication Technology Usage: A Case Study in Management EducationTrần Huy Anh ĐứcNessuna valutazione finora
- Radical Candor: Fully Revised and Updated Edition: How To Get What You Want by Saying What You Mean - Kim ScottDocumento5 pagineRadical Candor: Fully Revised and Updated Edition: How To Get What You Want by Saying What You Mean - Kim Scottzafytuwa17% (12)
- Fluorescent sensors for detection of heavy metalsDocumento36 pagineFluorescent sensors for detection of heavy metalskawtherahmedNessuna valutazione finora
- Sublime QR CodeDocumento6 pagineSublime QR Codejeff_sauserNessuna valutazione finora
- Risk Assessment For Modification of Phase 1 Existing Building GPR TankDocumento15 pagineRisk Assessment For Modification of Phase 1 Existing Building GPR TankAnandu Ashokan100% (1)
- A Personality Trait-Based Interactionist Model of Job PerformanceDocumento18 pagineA Personality Trait-Based Interactionist Model of Job PerformanceAlvina AhmedNessuna valutazione finora
- Design Theory: Boo Virk Simon Andrews Boo - Virk@babraham - Ac.uk Simon - Andrews@babraham - Ac.ukDocumento33 pagineDesign Theory: Boo Virk Simon Andrews Boo - Virk@babraham - Ac.uk Simon - Andrews@babraham - Ac.ukuzma munirNessuna valutazione finora
- NAVMC 3500.35A (Food Services)Documento88 pagineNAVMC 3500.35A (Food Services)Alexander HawkNessuna valutazione finora
- Grillage Method Applied to the Planning of Ship Docking 150-157 - JAROE - 2016-017 - JangHyunLee - - 최종Documento8 pagineGrillage Method Applied to the Planning of Ship Docking 150-157 - JAROE - 2016-017 - JangHyunLee - - 최종tyuNessuna valutazione finora
- Subject and Power - FoucaultDocumento10 pagineSubject and Power - FoucaultEduardo EspíndolaNessuna valutazione finora
- NX569J User ManualDocumento61 pagineNX569J User ManualHenry Orozco EscobarNessuna valutazione finora
- Reich Web ADocumento34 pagineReich Web Ak1nj3Nessuna valutazione finora
- Modal Analysis of Honeycomb Structure With Variation of Cell SizeDocumento3 pagineModal Analysis of Honeycomb Structure With Variation of Cell Sizeprateekg92Nessuna valutazione finora
- Charny - Mathematical Models of Bioheat TransferDocumento137 pagineCharny - Mathematical Models of Bioheat TransferMadalena PanNessuna valutazione finora
- Philippine Electronics & Communication Institute of TechnologyDocumento3 paginePhilippine Electronics & Communication Institute of TechnologyAngela MontonNessuna valutazione finora
- Tiger Facts: Physical Characteristics of the Largest CatDocumento14 pagineTiger Facts: Physical Characteristics of the Largest CatNagina ChawlaNessuna valutazione finora
- Mitchell 1986Documento34 pagineMitchell 1986Sara Veronica Florentin CuencaNessuna valutazione finora
- McKinsey & Co - Nonprofit Board Self-Assessment Tool Short FormDocumento6 pagineMcKinsey & Co - Nonprofit Board Self-Assessment Tool Short Formmoctapka088100% (1)
- Royal DSMDocumento16 pagineRoyal DSMSree100% (2)
- Saline Water Intrusion in Coastal Aquifers: A Case Study From BangladeshDocumento6 pagineSaline Water Intrusion in Coastal Aquifers: A Case Study From BangladeshIOSRJEN : hard copy, certificates, Call for Papers 2013, publishing of journalNessuna valutazione finora
- Lesson Rubric Team Group (Lesson Plan 1)Documento2 pagineLesson Rubric Team Group (Lesson Plan 1)Yodalis VazquezNessuna valutazione finora