Potrebbero piacerti anche
- Endocrine SystemDocumento27 pagineEndocrine SystemAlen Vukosavljevic100% (2)
- Physiology of PubertyDocumento4 paginePhysiology of PubertyHakimah K. Suhaimi100% (3)
- A Case Based Guide To Clinical Endocrinology 3rd Edition 2022Documento528 pagineA Case Based Guide To Clinical Endocrinology 3rd Edition 2022Muhammad Ahmad bin makruf syammakuNessuna valutazione finora
- Thyroid Function TestsDocumento24 pagineThyroid Function Testspavani valluriNessuna valutazione finora
- Thyroid Function Tests ExplainedDocumento25 pagineThyroid Function Tests ExplainedEva SinghNessuna valutazione finora
- Thyroid Gland L-Thyroxine (T4) Vs Triiodothyronine (T3) : Follicular CellsDocumento7 pagineThyroid Gland L-Thyroxine (T4) Vs Triiodothyronine (T3) : Follicular CellsPrincess Noreen SavellanoNessuna valutazione finora
- Clinical Approach of Thyroid Disorders: Hypothyroidsm and HyperthyroidsmDocumento73 pagineClinical Approach of Thyroid Disorders: Hypothyroidsm and HyperthyroidsmdiniNessuna valutazione finora
- Thyroid DiseasesDocumento44 pagineThyroid DiseasesPLDT HOMENessuna valutazione finora
- Thyroid Function Tests: Drneha Mahajan MD PathologyDocumento71 pagineThyroid Function Tests: Drneha Mahajan MD PathologyMukesh Kumar ChaudharyNessuna valutazione finora
- Disorder of ThyroidDocumento9 pagineDisorder of ThyroidJoezer Gumangan VeranoNessuna valutazione finora
- Kuliah Hyper and Hypothyroid - 2014Documento66 pagineKuliah Hyper and Hypothyroid - 2014Clararida RiawanNessuna valutazione finora
- HIPERTIROIDDocumento30 pagineHIPERTIROIDNandaNessuna valutazione finora
- ThyroiditisDocumento47 pagineThyroiditisaryanmetkarnewNessuna valutazione finora
- Hypothyroid in Pregnancy Andi CakraDocumento32 pagineHypothyroid in Pregnancy Andi CakraCakraEkkyNessuna valutazione finora
- Thyroid Function Tests: Understanding the Hidden Health ProblemDocumento34 pagineThyroid Function Tests: Understanding the Hidden Health Problemvjanand07100% (1)
- Thyroid DisordersDocumento34 pagineThyroid DisordersAbdulhameed Mohamed100% (1)
- Endocrinology Board Review: Thyroid DisordersDocumento46 pagineEndocrinology Board Review: Thyroid DisordersDemuel Dee L. BertoNessuna valutazione finora
- Diagnosis and Evaluation of Thyroid DisordersDocumento21 pagineDiagnosis and Evaluation of Thyroid DisordersIvan AditamaNessuna valutazione finora
- Class 6 (19.07.2022)Documento70 pagineClass 6 (19.07.2022)Ãqûã FîggâNessuna valutazione finora
- Thyrotoxicosis & Hypothyroidism by Prof DR NK ChopraDocumento52 pagineThyrotoxicosis & Hypothyroidism by Prof DR NK ChopraAbdulsalam DostNessuna valutazione finora
- Thyroid DisordersDocumento67 pagineThyroid DisordersMA 09Nessuna valutazione finora
- Hypothalamus-Pituitary-Thyroid Axis: PRESENTERS: DR: Nyangaresi Justine DR: Mitchelle Facilitator: DRDocumento31 pagineHypothalamus-Pituitary-Thyroid Axis: PRESENTERS: DR: Nyangaresi Justine DR: Mitchelle Facilitator: DRJustine NyangaresiNessuna valutazione finora
- Disorders of Thyroid Gland - S.D Osuntoye-1Documento32 pagineDisorders of Thyroid Gland - S.D Osuntoye-1IiiNessuna valutazione finora
- Thyroid HormonesDocumento50 pagineThyroid Hormonesanulalparayil2003Nessuna valutazione finora
- Clinical Practice For The Evaluation and Treatment OF Hyperthyroidism and HypothyroidismDocumento69 pagineClinical Practice For The Evaluation and Treatment OF Hyperthyroidism and HypothyroidismTutde SedanaNessuna valutazione finora
- Hypothyroidism, Hyperthyroidism, Thyroid Nodules, and CancerDocumento77 pagineHypothyroidism, Hyperthyroidism, Thyroid Nodules, and CancerDann San AntonioNessuna valutazione finora
- 1656070457849442Documento161 pagine1656070457849442aldeeray01Nessuna valutazione finora
- Hypothyroidism: Bagian Penyakit Dalam FK Uisu MedanDocumento50 pagineHypothyroidism: Bagian Penyakit Dalam FK Uisu Medanindra saputraNessuna valutazione finora
- Thyroiddisorders PDFDocumento51 pagineThyroiddisorders PDFIslam ShoukryNessuna valutazione finora
- Thyroiddisease 190216062020Documento42 pagineThyroiddisease 190216062020Manikandan Vp100% (1)
- Hyperthyroidism 1Documento88 pagineHyperthyroidism 1Mamikie Vukeya100% (1)
- Thyroid Disorders: Types, Symptoms, and TreatmentsDocumento41 pagineThyroid Disorders: Types, Symptoms, and Treatmentssheila_kohNessuna valutazione finora
- Mbs127 Slide Hyperthyroidism 1Documento46 pagineMbs127 Slide Hyperthyroidism 1revita262Nessuna valutazione finora
- DR Ananta Thyroid SlideDocumento73 pagineDR Ananta Thyroid SlideRoshan Kumar PanditNessuna valutazione finora
- Thyroid Gland Pharmacology to Clinical PracticeDocumento24 pagineThyroid Gland Pharmacology to Clinical Practiceamaal ramadanNessuna valutazione finora
- Thyroid & Anti-thyroid Drugs: An Overview of Hypothyroidism and Hyperthyroidism TreatmentDocumento59 pagineThyroid & Anti-thyroid Drugs: An Overview of Hypothyroidism and Hyperthyroidism TreatmentNiranjanNessuna valutazione finora
- Hyperthyroidism: Prevalence Women 2% Men 0.2% 15% of Cases Occur in Patients Older Than 60 Years of AgeDocumento54 pagineHyperthyroidism: Prevalence Women 2% Men 0.2% 15% of Cases Occur in Patients Older Than 60 Years of AgeMegan MendozaNessuna valutazione finora
- Thyroid Function Tests and Goitre SV 24-4-21Documento51 pagineThyroid Function Tests and Goitre SV 24-4-21Lal KhanNessuna valutazione finora
- ThyrotoxicosisDocumento105 pagineThyrotoxicosisAli Murtaza Abbas100% (1)
- Kuliah HyperthyroidDocumento18 pagineKuliah HyperthyroidFreddyNessuna valutazione finora
- Thyroid ReportDocumento105 pagineThyroid ReportAARVNessuna valutazione finora
- Hyperthyroidism: Forms and Treatment OptionsDocumento52 pagineHyperthyroidism: Forms and Treatment OptionsMedyWedhanggaNessuna valutazione finora
- Thyroid HormonesDocumento63 pagineThyroid HormonesDr. M. Prasad NaiduNessuna valutazione finora
- Thyroid Disorders ExplainedDocumento28 pagineThyroid Disorders ExplainedMina RoxasNessuna valutazione finora
- '3'hyperthyroid and HypothyroidDocumento42 pagine'3'hyperthyroid and Hypothyroidafriskha bulawanNessuna valutazione finora
- Disorders of The Thyroid: OutlineDocumento9 pagineDisorders of The Thyroid: OutlineMelissa-Andreea Ardeleanu Carvajal OsorioNessuna valutazione finora
- HSP2 Topic 4 Part 3 (Thyroid Disorders)Documento56 pagineHSP2 Topic 4 Part 3 (Thyroid Disorders)gilliansong17Nessuna valutazione finora
- Thyrotoxicosis Weight Loss and Energy LevelsDocumento7 pagineThyrotoxicosis Weight Loss and Energy LevelshappyhappylandNessuna valutazione finora
- Thyroid Disorders Guide: Causes, Symptoms & TreatmentsDocumento81 pagineThyroid Disorders Guide: Causes, Symptoms & Treatmentschetankumarbhumireddy50% (2)
- Thyroid Gland An Diseases of Thyroid D Gland: Omc LectureDocumento59 pagineThyroid Gland An Diseases of Thyroid D Gland: Omc LectureEdward MakemboNessuna valutazione finora
- Thyroid Disease in GeriatricsDocumento26 pagineThyroid Disease in GeriatricsTusvendran PillaiNessuna valutazione finora
- Hypo and Hyperthyroidism 2023Documento113 pagineHypo and Hyperthyroidism 2023Cristina Georgiana SerbanNessuna valutazione finora
- Anesthesia management for thyroid surgeryDocumento60 pagineAnesthesia management for thyroid surgeryyeabsraNessuna valutazione finora
- Diseases of The Thyroid Gland PDFDocumento72 pagineDiseases of The Thyroid Gland PDFKay BristolNessuna valutazione finora
- Thyroid Function: Clinical Chemistry IiiDocumento20 pagineThyroid Function: Clinical Chemistry IiiJannica Dominique ClarosNessuna valutazione finora
- Thyroid Function TestDocumento21 pagineThyroid Function TestPat JacintoNessuna valutazione finora
- Hyperthyroid DisordersDocumento49 pagineHyperthyroid Disordersayu permata dewiNessuna valutazione finora
- Hypothyroidism in PregnancyDocumento32 pagineHypothyroidism in PregnancyNicks KumarNessuna valutazione finora
- HyperthyroidismDocumento33 pagineHyperthyroidismNavin AdhikariNessuna valutazione finora
- Thyrotoxicosis: Presenter: Emiacu Kenneth Facilitator: Dr. Freddie KibengoDocumento35 pagineThyrotoxicosis: Presenter: Emiacu Kenneth Facilitator: Dr. Freddie KibengoNinaNessuna valutazione finora
- Thiroid DisordersDocumento11 pagineThiroid Disordersرعد النميريNessuna valutazione finora
- Thyroid Diet: How to improve and cure thyroid disorders, lose weight, and improve metabolism with the help of food!Da EverandThyroid Diet: How to improve and cure thyroid disorders, lose weight, and improve metabolism with the help of food!Nessuna valutazione finora
- Group 4 - Cardioactive Drugs and Antibiotics CC3Documento15 pagineGroup 4 - Cardioactive Drugs and Antibiotics CC3mayabangkurtipotNessuna valutazione finora
- Essential Kitchen Utensils ListDocumento8 pagineEssential Kitchen Utensils Listmayabangkurtipot73% (11)
- (Oxidation) Oxidatively Coupled WDocumento1 pagina(Oxidation) Oxidatively Coupled WmayabangkurtipotNessuna valutazione finora
- Editorial of InterDocumento2 pagineEditorial of IntermayabangkurtipotNessuna valutazione finora
- RicaDocumento2 pagineRicamayabangkurtipotNessuna valutazione finora
- EXPOSITORY ESSAY DiabetesDocumento1 paginaEXPOSITORY ESSAY DiabetesSaida BallesteroNessuna valutazione finora
- Chapter 15 - Hormones & Endocrine GlandsDocumento17 pagineChapter 15 - Hormones & Endocrine Glandsapi-3728508100% (1)
- Hyperthyroidism 1Documento34 pagineHyperthyroidism 1mussavir100% (2)
- Hypothyroidism - StatPearls - NCBI BookshelfDocumento10 pagineHypothyroidism - StatPearls - NCBI BookshelfKarla CordobaNessuna valutazione finora
- Thyroid Function Test PDFDocumento2 pagineThyroid Function Test PDFAlizaPinkyNessuna valutazione finora
- Sub: Price List of Minividas Reagents and ConsumablesDocumento3 pagineSub: Price List of Minividas Reagents and ConsumablesChemudupati BharaniNessuna valutazione finora
- Jurnal Grave DiseaseDocumento10 pagineJurnal Grave DiseasePutri Alfira ElfNessuna valutazione finora
- Rethinking Menopausal Hormone Therapy - For Whom, What, When, and How Long - CirculationDocumento19 pagineRethinking Menopausal Hormone Therapy - For Whom, What, When, and How Long - CirculationRodrigoNessuna valutazione finora
- Group 1 TCM Assigment 1Documento4 pagineGroup 1 TCM Assigment 1mayaNessuna valutazione finora
- This Study Resource Was: Case Study 52: Cushing Syndrome Sara SauersDocumento2 pagineThis Study Resource Was: Case Study 52: Cushing Syndrome Sara SauersJoshua del PozoNessuna valutazione finora
- THYROID Nodules PPT June 2013Documento56 pagineTHYROID Nodules PPT June 2013GaryNessuna valutazione finora
- Hypothyroidism in Context: Where We've Been and Where We're GoingDocumento12 pagineHypothyroidism in Context: Where We've Been and Where We're Going1130017003 AIMMATUL CHANIFAHNessuna valutazione finora
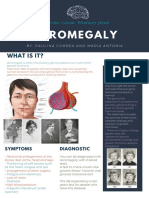
- Acromegaly: What Is It?Documento1 paginaAcromegaly: What Is It?Paulina CorreaaNessuna valutazione finora
- NCLEX EndocrineDocumento21 pagineNCLEX EndocrineChristopher Harris100% (7)
- List Ebook Kedokteran: Chat Me: 5457C343 / 08111506072 (Sms Only)Documento30 pagineList Ebook Kedokteran: Chat Me: 5457C343 / 08111506072 (Sms Only)Avian KrispratamaNessuna valutazione finora
- FAMILY KNOWLEDGE ABOUT DIABETES COMPLICATIONSDocumento10 pagineFAMILY KNOWLEDGE ABOUT DIABETES COMPLICATIONSEga ApriliaNessuna valutazione finora
- Oral Diabetic MedicationDocumento26 pagineOral Diabetic MedicationTaimoor BaigNessuna valutazione finora
- Background: Congenital Hypothyroidism Pediatric HypothyroidismDocumento1 paginaBackground: Congenital Hypothyroidism Pediatric HypothyroidismNiddy Rohim FebriadiNessuna valutazione finora
- Hypopituitarism PDFDocumento2 pagineHypopituitarism PDFcedricNessuna valutazione finora
- HypopituitarismDocumento2 pagineHypopituitarismGerardLum100% (2)
- Adrenal Function TestsDocumento103 pagineAdrenal Function TestsPriyanshu MandalNessuna valutazione finora
- Endocrine System PointersDocumento2 pagineEndocrine System PointersAlthea ValenzuelaNessuna valutazione finora
- Gestational Diabetes Mellitus (GDM)Documento24 pagineGestational Diabetes Mellitus (GDM)asyrafali93Nessuna valutazione finora
- Testosterone Levels in Healthy Men and The Relation To Behavioural and Physical Characteristics: Facts and ConstructsDocumento15 pagineTestosterone Levels in Healthy Men and The Relation To Behavioural and Physical Characteristics: Facts and ConstructsTUẤN TRẦN MINHNessuna valutazione finora
- Dec OI 2009Documento56 pagineDec OI 2009danbell6035100% (1)
- Type 2 Diabetes MellitusDocumento29 pagineType 2 Diabetes MellitusHuong NguyenNessuna valutazione finora
- Endocrine SystemDocumento3 pagineEndocrine SystemAnne Jillian83% (6)