Potrebbero piacerti anche
- A Laboratory Manual of Physical PharmaceuticsDa EverandA Laboratory Manual of Physical PharmaceuticsValutazione: 2.5 su 5 stelle2.5/5 (2)
- 2 - Practical Biochemistry Protein DetectionDocumento27 pagine2 - Practical Biochemistry Protein DetectionAMIRA HELAYELNessuna valutazione finora
- Total Proteins & Albumin AnalysisDocumento16 pagineTotal Proteins & Albumin AnalysisMustafa KhandgawiNessuna valutazione finora
- Amino Acids and Protein: DDC Medical Laboratory Science DepartmentDocumento32 pagineAmino Acids and Protein: DDC Medical Laboratory Science DepartmentMelody Jane PardilloNessuna valutazione finora
- Clinical Chemistry 1: Lipids and Lipoprotein - Methods in TestingDocumento5 pagineClinical Chemistry 1: Lipids and Lipoprotein - Methods in TestingBRYAN M. MOLDENessuna valutazione finora
- Kaplan: Clinical Chemistry, 5 Edition: Clinical References - Methods of AnalysisDocumento9 pagineKaplan: Clinical Chemistry, 5 Edition: Clinical References - Methods of AnalysispudjoNessuna valutazione finora
- Basic Principles of Clinical Chemistry, Glucose Pamphlet, BillirubinDocumento26 pagineBasic Principles of Clinical Chemistry, Glucose Pamphlet, BillirubinEslam NassarNessuna valutazione finora
- Dr. Weny Rinawati - Important and Novel Biomarker For HepatitisDocumento24 pagineDr. Weny Rinawati - Important and Novel Biomarker For Hepatitisiq_dianaNessuna valutazione finora
- Hemoglobin EstimationDocumento35 pagineHemoglobin EstimationAbhineet SalveNessuna valutazione finora
- Quantitative Estimation of Glucose BY Glucose Oxidase MethodDocumento60 pagineQuantitative Estimation of Glucose BY Glucose Oxidase MethodNihal100% (3)
- Basic Technique in HaematologyDocumento61 pagineBasic Technique in Haematologykiedd_04100% (26)
- Shrewsbury Presentation 011118Documento54 pagineShrewsbury Presentation 011118Amelie AvenidoNessuna valutazione finora
- TurbidimetryDocumento11 pagineTurbidimetryalexis mae IsonNessuna valutazione finora
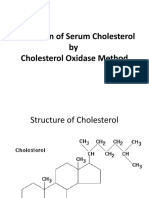
- Estimation of Serum CholesterolDocumento33 pagineEstimation of Serum CholesterolNihalNessuna valutazione finora
- Optimization of Biotinidase Assay: Dr. Faryal Husnain Resident Clinical ChemistryDocumento22 pagineOptimization of Biotinidase Assay: Dr. Faryal Husnain Resident Clinical ChemistrySaad KhanNessuna valutazione finora
- 2022 Clinical Biochemistry 2Documento27 pagine2022 Clinical Biochemistry 2Harvey MorrisNessuna valutazione finora
- Glycated Hemoglobin (Hba1C) : Prepared By: Basalingappa.B.G. 2 M.Sc. Medical Biochemistry JSS Medical College MysoreDocumento46 pagineGlycated Hemoglobin (Hba1C) : Prepared By: Basalingappa.B.G. 2 M.Sc. Medical Biochemistry JSS Medical College MysoreYuniati ValentinaNessuna valutazione finora
- UrinaryDocumento3 pagineUrinaryIYA LABAO100% (1)
- Proteins: M. Zaharna Ckin. Chem. 2009Documento28 pagineProteins: M. Zaharna Ckin. Chem. 2009Ahmed GaberNessuna valutazione finora
- Lecture-9 Blood Chemistry AnalyzerDocumento15 pagineLecture-9 Blood Chemistry AnalyzerCherinetNessuna valutazione finora
- Albumin: OSR6102 4 X 29 ML R1 OSR6202 4 X 54 ML R1 OSR6602 4 X 173 ML R1Documento2 pagineAlbumin: OSR6102 4 X 29 ML R1 OSR6202 4 X 54 ML R1 OSR6602 4 X 173 ML R1irwoons70Nessuna valutazione finora
- Cch10 Protein2Documento52 pagineCch10 Protein2Habtamu MollaNessuna valutazione finora
- Protein Determination Assays: Xin Li Scott Group 05/10/2005Documento28 pagineProtein Determination Assays: Xin Li Scott Group 05/10/2005hemanthv3Nessuna valutazione finora
- Diagnosis of HemoglobinopathiesDocumento18 pagineDiagnosis of HemoglobinopathiesTshwarelo LegodiNessuna valutazione finora
- Non Invasive Methods of Estimating Pharmacokinetic Parameters2Documento31 pagineNon Invasive Methods of Estimating Pharmacokinetic Parameters2Thilak Chandra50% (2)
- Biuret Protein Assay Lab Powerpoint.Documento22 pagineBiuret Protein Assay Lab Powerpoint.ishanNessuna valutazione finora
- Protein Characterization-2020Documento79 pagineProtein Characterization-2020Gia Hoàng100% (1)
- Pengkajian Status Gizi Atlit Secara BiokimiaDocumento31 paginePengkajian Status Gizi Atlit Secara Biokimiatrioni widyastutiNessuna valutazione finora
- 10.1515 cclm.2008.079Documento5 pagine10.1515 cclm.2008.079sdaaNessuna valutazione finora
- Clinical Tray PPT Batch B (Final) - 1Documento92 pagineClinical Tray PPT Batch B (Final) - 1Archna AgarwalNessuna valutazione finora
- Laboratory Quality ControlDocumento52 pagineLaboratory Quality ControlSimon HafeniNessuna valutazione finora
- Spectro Presentation1Documento25 pagineSpectro Presentation1Ahmad AzmiNessuna valutazione finora
- Albumin: N.S. Bio-TecDocumento2 pagineAlbumin: N.S. Bio-Tecكن مع اللهNessuna valutazione finora
- 1593983660haemoglobin Estimation MethodsDocumento24 pagine1593983660haemoglobin Estimation MethodsJune VasquezNessuna valutazione finora
- Bradford Assay Prelab PDFDocumento19 pagineBradford Assay Prelab PDFMaila EscuderoNessuna valutazione finora
- Albumin: Intended Use MethodDocumento2 pagineAlbumin: Intended Use MethodForhadur RezaNessuna valutazione finora
- Lipid and Glucose Methodology PDFDocumento16 pagineLipid and Glucose Methodology PDFJezzah Mae CañeteNessuna valutazione finora
- Javma-Javma 2000 216 198Documento5 pagineJavma-Javma 2000 216 198jv56cz8cxqNessuna valutazione finora
- Chapter 8Documento2 pagineChapter 8eduar2308doNessuna valutazione finora
- Hematology Presentation 2Documento57 pagineHematology Presentation 2lemmabekeleNessuna valutazione finora
- 12a Diabetic Emergencies DKA Case StudiesDocumento13 pagine12a Diabetic Emergencies DKA Case StudiesAnonymous yTdBi7100% (1)
- Clinical Bio. Ch1Documento51 pagineClinical Bio. Ch1ellaNessuna valutazione finora
- 5-Alkaline PhosphataseDocumento7 pagine5-Alkaline PhosphataseAzhar Clinical Laboratory TubeNessuna valutazione finora
- MLS 111B LABORATORY ENDTERM Very FinalDocumento6 pagineMLS 111B LABORATORY ENDTERM Very FinalJohanna MarieNessuna valutazione finora
- Protein Purification and Characterization TechniquesDocumento19 pagineProtein Purification and Characterization Techniqueskanti priya KondalaNessuna valutazione finora
- CSF PresentationDocumento17 pagineCSF PresentationJaime GaviolaNessuna valutazione finora
- Lab Activity No. 1 - Slide PresentationDocumento27 pagineLab Activity No. 1 - Slide PresentationChelsea Padilla Delos ReyesNessuna valutazione finora
- Renal Function Test Amcj 8Documento42 pagineRenal Function Test Amcj 8Md. Saifur Rahman SunnyNessuna valutazione finora
- Management of Lab & Interpretation of ResultsDocumento30 pagineManagement of Lab & Interpretation of ResultsArthur Derman Sith-leeNessuna valutazione finora
- High Performance Liquid Chromatography: Heavenlight ChristopherDocumento17 pagineHigh Performance Liquid Chromatography: Heavenlight ChristopherHussein AbduNessuna valutazione finora
- Antibody and Soluble Antigen Precipitation Reactions PrecipitinsDocumento25 pagineAntibody and Soluble Antigen Precipitation Reactions PrecipitinsRakin Bin RaihanNessuna valutazione finora
- Hba Standardisation: History, Science and Politics: CommentaryDocumento6 pagineHba Standardisation: History, Science and Politics: CommentaryTakaNessuna valutazione finora
- Hepatitis B 5 ParametersDocumento16 pagineHepatitis B 5 ParametersAKINYEMI OLUBUNMINessuna valutazione finora
- Liver Assessment of Liver FunctionDocumento25 pagineLiver Assessment of Liver FunctionReman A. AlingasaNessuna valutazione finora
- Clearance and GFR: Major DR Arabinda Mohan Bhattarai Lecturer (Biochemistry), NAIHSDocumento25 pagineClearance and GFR: Major DR Arabinda Mohan Bhattarai Lecturer (Biochemistry), NAIHSChandan SahNessuna valutazione finora
- Newsletter10-1 SebiaDocumento4 pagineNewsletter10-1 SebiaNidiam2100% (1)
- Guía Lab. 2 BC1Documento8 pagineGuía Lab. 2 BC1Cristiana Auxiliadora Fonseca MayorgaNessuna valutazione finora
- Complementary and Alternative Medical Lab Testing Part 6: Liver and GallbladderDa EverandComplementary and Alternative Medical Lab Testing Part 6: Liver and GallbladderNessuna valutazione finora
- Caffeine BronchodilatorDocumento30 pagineCaffeine Bronchodilatormonday125Nessuna valutazione finora
- Clinical Guideline For Anticoagulant Use in AdultsDocumento108 pagineClinical Guideline For Anticoagulant Use in Adultsmonday125Nessuna valutazione finora
- ADMA 2010 BlackboardDocumento41 pagineADMA 2010 Blackboardmonday125Nessuna valutazione finora
- Uric AcidDocumento6 pagineUric Acidmonday125100% (1)
- Karen Smith Duty Biochemist ScenariosDocumento43 pagineKaren Smith Duty Biochemist Scenariosmonday125100% (2)
- Pleasing Her Husband's Boss (Hot Wife and Her Cuckold 2) by Michaels DeanaDocumento29 paginePleasing Her Husband's Boss (Hot Wife and Her Cuckold 2) by Michaels Deanamonday12560% (10)
- 2010 - Zhang - EAP For AR Review PDFDocumento8 pagine2010 - Zhang - EAP For AR Review PDFmonday125Nessuna valutazione finora
- OspeDocumento29 pagineOspemonday125Nessuna valutazione finora
- Bible 2018Documento183 pagineBible 2018monday125Nessuna valutazione finora
- FRCPath OSPE 25042014Documento11 pagineFRCPath OSPE 25042014monday125Nessuna valutazione finora
- ST Agnes Catholic Primary SchoolDocumento12 pagineST Agnes Catholic Primary Schoolmonday125Nessuna valutazione finora
- ICP-MS Talk ACBDocumento31 pagineICP-MS Talk ACBmonday125Nessuna valutazione finora
- FOCUS SAS Training Day Leeds Dr. Joanna Sheldon Protein Reference Unit, St. George'sDocumento19 pagineFOCUS SAS Training Day Leeds Dr. Joanna Sheldon Protein Reference Unit, St. George'smonday125Nessuna valutazione finora
- Critical Appraisal: DR A C J Hutchesson Chair of Examiners' Panel, Frcpath (Clinical Biochemistry)Documento10 pagineCritical Appraisal: DR A C J Hutchesson Chair of Examiners' Panel, Frcpath (Clinical Biochemistry)monday125Nessuna valutazione finora
- FRCPath Cases 1Documento36 pagineFRCPath Cases 1monday125100% (1)
- FRCPath Chemical Pathology CurriculumDocumento109 pagineFRCPath Chemical Pathology Curriculummonday125Nessuna valutazione finora
- Model Albumin AnswerDocumento13 pagineModel Albumin Answermonday125Nessuna valutazione finora
- Writing An Abstract: Sally - Benton@bartshealth - Nhs.ukDocumento7 pagineWriting An Abstract: Sally - Benton@bartshealth - Nhs.ukmonday125Nessuna valutazione finora
- Master Sheet: 1. Irregular ClotDocumento20 pagineMaster Sheet: 1. Irregular Clotmonday125Nessuna valutazione finora
- Bill Bartlett - 1 1 1Documento68 pagineBill Bartlett - 1 1 1monday125Nessuna valutazione finora
- Abaxis Piccolo Analyzer - User ManualDocumento67 pagineAbaxis Piccolo Analyzer - User ManualАндрей ДубровинNessuna valutazione finora
- Photodynamic Effects of Thuja OccidentalisDocumento155 paginePhotodynamic Effects of Thuja OccidentalisCat SkullNessuna valutazione finora
- 2 Oral Drug Products-Product Quality TestsDocumento5 pagine2 Oral Drug Products-Product Quality TestssofianesedkaouiNessuna valutazione finora
- Flinders University Statement of Assessment Methods - 2020: Student Academic Integrity PolicyDocumento5 pagineFlinders University Statement of Assessment Methods - 2020: Student Academic Integrity PolicyEmilieNessuna valutazione finora
- Package Insert - Procleix Ultrio Elite Assay PDFDocumento50 paginePackage Insert - Procleix Ultrio Elite Assay PDFmooooooooodyNessuna valutazione finora
- 2017-05-01 Final Nystatin Notice To Customer Letter PDFDocumento2 pagine2017-05-01 Final Nystatin Notice To Customer Letter PDFsaidvaretNessuna valutazione finora
- Laboratory Procedure Manual: Triglycerides SerumDocumento22 pagineLaboratory Procedure Manual: Triglycerides SerumTarunNessuna valutazione finora
- 01 Glucose G71245R04Documento7 pagine01 Glucose G71245R04chem.rajavithiNessuna valutazione finora
- FDA OOS Guideline Out of SpecificationDocumento17 pagineFDA OOS Guideline Out of SpecificationGabriel Bianco100% (1)
- Inserto Control Idg PDFDocumento3 pagineInserto Control Idg PDFLoren Orozco0% (1)
- Ash Well 1957Documento33 pagineAsh Well 1957Eko Isro RiyantoNessuna valutazione finora
- Drill ProtocolsDocumento9 pagineDrill ProtocolsBrata NaibahoNessuna valutazione finora
- MDCG 2021-22 enDocumento6 pagineMDCG 2021-22 eneliNessuna valutazione finora
- Adaltis Catalogue 2015 PDFDocumento78 pagineAdaltis Catalogue 2015 PDFSantiagoAF50% (2)
- Inteliq Ethanol/Ammonia Control Levels 1, 2 and 3Documento2 pagineInteliq Ethanol/Ammonia Control Levels 1, 2 and 3jnyng222Nessuna valutazione finora
- Quality Control in Low Budget LaboratoriesDocumento42 pagineQuality Control in Low Budget Laboratorieszahraa aliNessuna valutazione finora
- MPN User ManualDocumento41 pagineMPN User ManualsarajevinaNessuna valutazione finora
- Vancomycin ARCDocumento7 pagineVancomycin ARCtesteteee testtesteteNessuna valutazione finora
- Alb enDocumento10 pagineAlb enMARICENessuna valutazione finora
- Centrifugal Analyzer (Clinical Chemistry)Documento16 pagineCentrifugal Analyzer (Clinical Chemistry)Lois Danielle33% (3)
- User Manual: Name: Alegria Code: ORG 300-00Documento60 pagineUser Manual: Name: Alegria Code: ORG 300-00Charlie Channels100% (1)
- Key Comparison CCQM-K34 Assay of Potassium Hydrogen PhthalateDocumento12 pagineKey Comparison CCQM-K34 Assay of Potassium Hydrogen PhthalatemariassyNessuna valutazione finora
- Drug Substance S: 1 General Information S 1.1 NomenclatureDocumento5 pagineDrug Substance S: 1 General Information S 1.1 NomenclatureMajesty YmanaNessuna valutazione finora
- Nutrient in SoilDocumento3 pagineNutrient in SoilSontu BardhanNessuna valutazione finora
- F3089-14 Standard Guide For Characterization and StandDocumento17 pagineF3089-14 Standard Guide For Characterization and Standastewayb_964354182Nessuna valutazione finora
- Waters Method DevelopmentDocumento50 pagineWaters Method DevelopmentSouradipta GangulyNessuna valutazione finora
- Calculation of System Suitability ParametersDocumento10 pagineCalculation of System Suitability ParametersMubarak Patel100% (1)
- AAGP2 enDocumento3 pagineAAGP2 enLince WijoyoNessuna valutazione finora
- Alb BiosDocumento2 pagineAlb BiosrichardNessuna valutazione finora
- DX IRMDocumento340 pagineDX IRMsantoshNessuna valutazione finora