Potrebbero piacerti anche
- Community Health Nursing 1 NCM 104Documento4 pagineCommunity Health Nursing 1 NCM 104Sheila May Teope Santos100% (1)
- Public Health Management: Time For A New Start?Documento5 paginePublic Health Management: Time For A New Start?dwi rizkyNessuna valutazione finora
- CHN Module 1Documento34 pagineCHN Module 1Don Maur ValeteNessuna valutazione finora
- Atc Whitepaper 040616Documento12 pagineAtc Whitepaper 040616Teenu JobyNessuna valutazione finora
- NCM 113 - Lec Reviewer PrelimDocumento9 pagineNCM 113 - Lec Reviewer PrelimKylle AlimosaNessuna valutazione finora
- 14 Supporting Prevention and Chronic Condition Self-ManagementDocumento8 pagine14 Supporting Prevention and Chronic Condition Self-Managementilham apriadiNessuna valutazione finora
- Public Health Community Health Nursing: Goal: To Enable EveryDocumento10 paginePublic Health Community Health Nursing: Goal: To Enable Everyjamie carpioNessuna valutazione finora
- This Study Resource WasDocumento8 pagineThis Study Resource WasMae Ann BusicoNessuna valutazione finora
- CHN 1Documento10 pagineCHN 1keiemorayaNessuna valutazione finora
- Lesson 2Documento11 pagineLesson 2John Dave V. VillarmenteNessuna valutazione finora
- Primary Health Care and Family MedicineDocumento5 paginePrimary Health Care and Family MedicineCATHERINE HAYNESNessuna valutazione finora
- RP248 Health Systems, Management, and Organization in Low-And Middle Income CountriesDocumento15 pagineRP248 Health Systems, Management, and Organization in Low-And Middle Income CountriesBoyIPNessuna valutazione finora
- Chapter 4 - The Whole Health Process - 2018 - Integrative MedicineDocumento8 pagineChapter 4 - The Whole Health Process - 2018 - Integrative Medicineandre100% (1)
- Midterm Healthcare Delivery System Part IDocumento5 pagineMidterm Healthcare Delivery System Part IKrisha Jane De Los SantosNessuna valutazione finora
- History of Primary Health Care ExplainedDocumento8 pagineHistory of Primary Health Care ExplainedChrysadel BalabaNessuna valutazione finora
- Tan, Li Luren Raphaelle S. Date: May 7, 2019Documento5 pagineTan, Li Luren Raphaelle S. Date: May 7, 2019Li Luren Raphaelle TanNessuna valutazione finora
- Niveles de Atención, Prevencion Primaria en SaludDocumento4 pagineNiveles de Atención, Prevencion Primaria en SaludmARLENNessuna valutazione finora
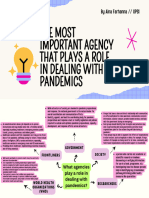
- Muet Task:: 18 Jan 2024Documento2 pagineMuet Task:: 18 Jan 2024ainafarhanna05Nessuna valutazione finora
- Name: Nick N. Polestico Section: BSMT 1-BDocumento2 pagineName: Nick N. Polestico Section: BSMT 1-BNick PolesticoNessuna valutazione finora
- Health Systems Strengthening, Universal Health Coverage, Health Security and ResilienceDocumento1 paginaHealth Systems Strengthening, Universal Health Coverage, Health Security and ResilienceCharles ChalimbaNessuna valutazione finora
- Das (2018) Universal Delivery of HealthcareDocumento5 pagineDas (2018) Universal Delivery of HealthcareWaqasRabbaniNessuna valutazione finora
- Functions and standards of a Public Health SystemDocumento20 pagineFunctions and standards of a Public Health SystemAlina ForrayNessuna valutazione finora
- Health PromotionDocumento7 pagineHealth PromotionSharmaine Mae BalmateroNessuna valutazione finora
- National Diabetes Plans Support Healthcare System ChangesDocumento3 pagineNational Diabetes Plans Support Healthcare System ChangesdewiNessuna valutazione finora
- CHN 1Documento12 pagineCHN 1Karl Gabriel BonifacioNessuna valutazione finora
- The Evolution of Public Health Emergency Ajph.2017.303947Documento8 pagineThe Evolution of Public Health Emergency Ajph.2017.303947Jack Yu-Tung ChangNessuna valutazione finora
- CHN Module 1Documento5 pagineCHN Module 1jaoNessuna valutazione finora
- Role of Institutions in Public Health EducationDocumento5 pagineRole of Institutions in Public Health EducationDeepakNessuna valutazione finora
- Div Class Title Primary Care Provider Approaches To Preventive Health Delivery A Qualitative Study DivDocumento11 pagineDiv Class Title Primary Care Provider Approaches To Preventive Health Delivery A Qualitative Study DivlucaswbmNessuna valutazione finora
- CP - Building Resilient Health Systems A Propos1Documento9 pagineCP - Building Resilient Health Systems A Propos1Claudia CortesNessuna valutazione finora
- Driving Public Health and Health PromotionDocumento75 pagineDriving Public Health and Health Promotionflameglitter21Nessuna valutazione finora
- CPH Lec ReviewrDocumento24 pagineCPH Lec ReviewrCresma Santa Rayjane DesamparoNessuna valutazione finora
- Emergency Health Education and Communication: A Primer For Health EducatorsDocumento4 pagineEmergency Health Education and Communication: A Primer For Health EducatorsJJoliat100% (1)
- Medical Genetics India ArticleDocumento11 pagineMedical Genetics India ArticleyarleyNessuna valutazione finora
- Goals of Primary Health Care in Less Than 150 WordsDocumento4 pagineGoals of Primary Health Care in Less Than 150 WordsAlyssa PicarNessuna valutazione finora
- Thesis - Prevention of Nosocomial Infections As Percieved by Staff NursesDocumento31 pagineThesis - Prevention of Nosocomial Infections As Percieved by Staff NursesShine Lyn92% (12)
- Health Care SystemDocumento3 pagineHealth Care SystemERESTALL SENNDI GRACE OLIVERASNessuna valutazione finora
- Quality Assurance Framework - Print - 06 Sept 2022Documento56 pagineQuality Assurance Framework - Print - 06 Sept 2022RaNa MBNessuna valutazione finora
- Pendidikan KesehatanDocumento22 paginePendidikan KesehatanAGIL ADHITIA GUNAWANNessuna valutazione finora
- (1998) Chronic Disease Management What Will It Take To Improve Care For Chronic IllnessDocumento3 pagine(1998) Chronic Disease Management What Will It Take To Improve Care For Chronic IllnessDaniel MeloNessuna valutazione finora
- SIKL - Canada - State, 2007-1Documento44 pagineSIKL - Canada - State, 2007-1valentino febryandyNessuna valutazione finora
- MT102 ReviewerDocumento5 pagineMT102 ReviewerLuke Aaron GoticoNessuna valutazione finora
- Cbabddd 273 B 3 A 6 e 024 e 5Documento8 pagineCbabddd 273 B 3 A 6 e 024 e 5api-620025002Nessuna valutazione finora
- Dental Public Health 2Documento11 pagineDental Public Health 2El BeeNessuna valutazione finora
- 6-Hnd-713 - Motivating Behavioural Change To Promote Public HealthDocumento8 pagine6-Hnd-713 - Motivating Behavioural Change To Promote Public HealthSaira JabeenNessuna valutazione finora
- The role of patient care teams in chronic disease managementDocumento4 pagineThe role of patient care teams in chronic disease managementIndah SundariNessuna valutazione finora
- Community Health Nursing Review NotesDocumento5 pagineCommunity Health Nursing Review NotesMaria Ana AguilarNessuna valutazione finora
- Occupational Therapy and Management of Multiple Chronic Conditions in The Context of Health Care ReformDocumento6 pagineOccupational Therapy and Management of Multiple Chronic Conditions in The Context of Health Care ReformNataliaNessuna valutazione finora
- FPHP GlossaryDocumento4 pagineFPHP GlossaryArjun Singh ChoudharyNessuna valutazione finora
- 1 s2.0 S2213076418300654 MainDocumento5 pagine1 s2.0 S2213076418300654 MaindaytdeenNessuna valutazione finora
- Health Services DeliveryDocumento13 pagineHealth Services DeliveryRonit ChandNessuna valutazione finora
- Improving Health in Saudi Arabia: Through Population Health ManagementDocumento27 pagineImproving Health in Saudi Arabia: Through Population Health Managementiyad.alsabiNessuna valutazione finora
- Community Health - Chapter 2Documento21 pagineCommunity Health - Chapter 2Kyla MoretoNessuna valutazione finora
- Cientific Dental Research Journal (CDRJ)Documento6 pagineCientific Dental Research Journal (CDRJ)Gita RizkiNessuna valutazione finora
- Patient Care Management 1 and 2Documento128 paginePatient Care Management 1 and 2Lantana MedikaNessuna valutazione finora
- Community Health Nursing ConceptsDocumento10 pagineCommunity Health Nursing ConceptsJacqueline S. PunoNessuna valutazione finora
- Guidance For The Ethical Allocation of Scarce ResourcesDocumento21 pagineGuidance For The Ethical Allocation of Scarce ResourcesUSA TODAY NetworkNessuna valutazione finora
- Transformative Healthcare - DNP's Role in Improving Chronic Disease ManagementDocumento8 pagineTransformative Healthcare - DNP's Role in Improving Chronic Disease ManagementSam GitongaNessuna valutazione finora
- Stachtchenko 1990Documento8 pagineStachtchenko 1990Marco A. BeltránNessuna valutazione finora
- Int. J. Production Economics: Lauren B. Davis, Funda Samanlioglu, Xiuli Qu, Sarah RootDocumento13 pagineInt. J. Production Economics: Lauren B. Davis, Funda Samanlioglu, Xiuli Qu, Sarah RootAnonymous dVcPCxF4eJNessuna valutazione finora
- Report Eefit Sumatra Indonesia 20190816Documento85 pagineReport Eefit Sumatra Indonesia 20190816Anonymous dVcPCxF4eJNessuna valutazione finora
- Sri Lanka - Economic Crisis - BBC NewsDocumento11 pagineSri Lanka - Economic Crisis - BBC NewsAnonymous dVcPCxF4eJNessuna valutazione finora
- 2017 Calendar TemplateDocumento12 pagine2017 Calendar TemplatemeliabudiNessuna valutazione finora
- Disaster Risk Management for Health FacilitiesDocumento2 pagineDisaster Risk Management for Health FacilitiesAnonymous dVcPCxF4eJNessuna valutazione finora
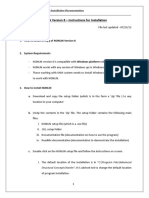
- NONLIN ReadMe PDFDocumento8 pagineNONLIN ReadMe PDFAnonymous dVcPCxF4eJNessuna valutazione finora
- Poljan-Ek Et Al-2012-Earthquake Engineering & Structural Dynamics PDFDocumento19 paginePoljan-Ek Et Al-2012-Earthquake Engineering & Structural Dynamics PDFAnonymous dVcPCxF4eJNessuna valutazione finora
- Decision Making Under Uncertainty for Seismic Risk ManagementDocumento17 pagineDecision Making Under Uncertainty for Seismic Risk ManagementAnonymous dVcPCxF4eJNessuna valutazione finora
- Disaster Risk Management for Health FacilitiesDocumento2 pagineDisaster Risk Management for Health FacilitiesAnonymous dVcPCxF4eJNessuna valutazione finora
- Lawson, Zero, 2013Documento7 pagineLawson, Zero, 2013Anonymous dVcPCxF4eJNessuna valutazione finora
- Prioritization of Bridges in EQ Risk Mitigation Using MCDA Lisbon-Paper (Bana-E-Costa 2006)Documento9 paginePrioritization of Bridges in EQ Risk Mitigation Using MCDA Lisbon-Paper (Bana-E-Costa 2006)Anonymous dVcPCxF4eJNessuna valutazione finora
- INSS Program 2014 OnlineDocumento14 pagineINSS Program 2014 OnlineAnonymous dVcPCxF4eJNessuna valutazione finora
- MICHAEL FARDIS - Seismic - Isolation - Principles - and - Practice PDFDocumento69 pagineMICHAEL FARDIS - Seismic - Isolation - Principles - and - Practice PDFAnonymous dVcPCxF4eJNessuna valutazione finora
- Article1380115495 - Islam Et Al PDFDocumento19 pagineArticle1380115495 - Islam Et Al PDFSelene Duno AlvarezNessuna valutazione finora
- Knoeri Et Al 2014 Enhancing Recycling of Construction Materials - IpadDocumento13 pagineKnoeri Et Al 2014 Enhancing Recycling of Construction Materials - IpadAnonymous dVcPCxF4eJNessuna valutazione finora
- Assessment of Tiie Seismic Vlflnerability of Existing BuildingsDocumento8 pagineAssessment of Tiie Seismic Vlflnerability of Existing BuildingsAnonymous dVcPCxF4eJNessuna valutazione finora
- Performance Based Seismic DesignDocumento550 paginePerformance Based Seismic Designijump12100% (9)
- FEMA P58: Next-Generation Building Seismic Performance Assessment MethodologyDocumento10 pagineFEMA P58: Next-Generation Building Seismic Performance Assessment MethodologyAnonymous dVcPCxF4eJNessuna valutazione finora
- KDIGO Diabetes 2022 Guideline Slide SetDocumento68 pagineKDIGO Diabetes 2022 Guideline Slide SetBigPharma HealtcareNessuna valutazione finora
- Additional Information For The Review of Related Literature - Study On OfW ChildrenDocumento4 pagineAdditional Information For The Review of Related Literature - Study On OfW Childrencarollangcay67% (3)
- Definisi Gagal JantungDocumento12 pagineDefinisi Gagal JantungyudhistiraNessuna valutazione finora
- Healthcare Adminstration SyllabusDocumento1 paginaHealthcare Adminstration Syllabuspankaj DevrariNessuna valutazione finora
- CJN 079Documento199 pagineCJN 079SelvaArockiamNessuna valutazione finora
- The Truth About EtawahDocumento4 pagineThe Truth About EtawahPoojaDasgupta100% (1)
- Abhinava ChintamaniDocumento7 pagineAbhinava ChintamaniBrad Yantzer50% (2)
- Chemical Injuries of Oral CavityDocumento58 pagineChemical Injuries of Oral CavityShalini SoniNessuna valutazione finora
- Viral Load SopDocumento18 pagineViral Load SopzamadulaNessuna valutazione finora
- Sal Rosada Inves FinalDocumento26 pagineSal Rosada Inves Finalbrigida100% (2)
- Chapter 12 Social Welfare MeasuresDocumento44 pagineChapter 12 Social Welfare MeasuresChandan ChanduNessuna valutazione finora
- English - Argumentative EssayDocumento3 pagineEnglish - Argumentative EssayRicci ChingNessuna valutazione finora
- NUR5020-James AxisaDocumento204 pagineNUR5020-James AxisaVicky Torina ShilohNessuna valutazione finora
- BX2051 - Assessment One InformationDocumento4 pagineBX2051 - Assessment One InformationVais VaishnavNessuna valutazione finora
- P504 Work PackDocumento16 pagineP504 Work PackFernando SantosNessuna valutazione finora
- Controversial Fat LossDocumento30 pagineControversial Fat LossAnthony Davis100% (5)
- United States Foreign AidDocumento10 pagineUnited States Foreign AidDearsaNessuna valutazione finora
- Statement of Purpose AuburnDocumento2 pagineStatement of Purpose AuburnSakibur Rahman ShuvoNessuna valutazione finora
- WhatsApp Chat About University Classes and Subject RegistrationDocumento114 pagineWhatsApp Chat About University Classes and Subject RegistrationRana HanzlaNessuna valutazione finora
- Nelmilian Melendez-Garcia 761091 0 1Documento6 pagineNelmilian Melendez-Garcia 761091 0 1api-533670449Nessuna valutazione finora
- Bank OleDocumento7 pagineBank OlezumyNessuna valutazione finora
- By: Muhammad Farouk A. Jajurie, JRDocumento20 pagineBy: Muhammad Farouk A. Jajurie, JRpengkobabesNessuna valutazione finora
- The Placebo EffectDocumento2 pagineThe Placebo EffectMeshack RutoNessuna valutazione finora
- Uma Kita.: Skylite Musicals 2019 Visual AtmosphereDocumento14 pagineUma Kita.: Skylite Musicals 2019 Visual AtmosphereJasmine AyuNessuna valutazione finora
- Pilocarpine Eye DropDocumento3 paginePilocarpine Eye DropSidahmed SiDo BouchenakNessuna valutazione finora
- Occlusal Adjustment For Treating and Preventing Temporomandibular Joint Disorders ReviewDocumento25 pagineOcclusal Adjustment For Treating and Preventing Temporomandibular Joint Disorders ReviewMostafa HassanNessuna valutazione finora
- Removal of CatheterDocumento2 pagineRemoval of CatheterMargaret ArellanoNessuna valutazione finora
- SRSG A 74 259 EnglishDocumento16 pagineSRSG A 74 259 EnglishsofiabloemNessuna valutazione finora
- Albion Metal ChelationDocumento6 pagineAlbion Metal ChelationI. Murali KrishnaNessuna valutazione finora
- Every Child Matters PDF 2003Documento2 pagineEvery Child Matters PDF 2003AshleyNessuna valutazione finora