Potrebbero piacerti anche
- AMI Case ReportDocumento19 pagineAMI Case ReportTimothy TanNessuna valutazione finora
- History Taking SampleDocumento7 pagineHistory Taking SampleJem QuintoNessuna valutazione finora
- Hamstring InjuriesDocumento6 pagineHamstring InjuriesIlian GeorgievNessuna valutazione finora
- Actual Practice On The Maagement of Care AnginaDocumento96 pagineActual Practice On The Maagement of Care AnginaJaymica Laggui DacquilNessuna valutazione finora
- Pathological Conditions of Nervous System 1Documento40 paginePathological Conditions of Nervous System 1Fia bianca ColibaoNessuna valutazione finora
- DSCI8309 Clinical Nutrition Fall 2012 08Documento7 pagineDSCI8309 Clinical Nutrition Fall 2012 08lliioNessuna valutazione finora
- Dr. Vinod K. Ravaliya, MPT Cardiothoracic Physiotherapy Shree Krishna Hospital KMPIP, KaramsadDocumento54 pagineDr. Vinod K. Ravaliya, MPT Cardiothoracic Physiotherapy Shree Krishna Hospital KMPIP, KaramsadEvangelin Melvin100% (1)
- Cardiac Rehabilitation QuizzesDocumento7 pagineCardiac Rehabilitation QuizzesMarly Atef Shoukry AzizNessuna valutazione finora
- Cardiovascular System: Presented byDocumento76 pagineCardiovascular System: Presented bySoma Al-mutairiNessuna valutazione finora
- Cardiac PPT SeminarDocumento129 pagineCardiac PPT SeminarjoashannNessuna valutazione finora
- HypermagnesemiaDocumento5 pagineHypermagnesemiaNader Smadi100% (1)
- Cardiac Rehab: ND RD TH NDDocumento3 pagineCardiac Rehab: ND RD TH NDDoodsDiagoNessuna valutazione finora
- CVDDocumento22 pagineCVDvijaymusic88100% (1)
- VLC Christian Studies Scope and Sequence 2015Documento3 pagineVLC Christian Studies Scope and Sequence 2015api-335947977Nessuna valutazione finora
- High Altitude Sickness, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsDa EverandHigh Altitude Sickness, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNessuna valutazione finora
- Cardiogenic ShockDocumento5 pagineCardiogenic ShockAttilio Del RossoNessuna valutazione finora
- Tamara Case StudyDocumento6 pagineTamara Case Studymike0% (1)
- CPD For Nurses Udp081010Documento27 pagineCPD For Nurses Udp081010Faiq Fuat100% (2)
- Chapter 52 Endocrine Disorders Unit 1Documento55 pagineChapter 52 Endocrine Disorders Unit 1Glory Mimi100% (1)
- Chapter 1-10 Answer HelpDocumento224 pagineChapter 1-10 Answer HelplilsssNessuna valutazione finora
- ACS - Clinical Review 2015Documento11 pagineACS - Clinical Review 2015Purwoko SugengNessuna valutazione finora
- Hypertension and ExerciseDocumento8 pagineHypertension and ExercisemeyqiNessuna valutazione finora
- Research Paper - DiabetesDocumento9 pagineResearch Paper - Diabetesapi-281590163Nessuna valutazione finora
- New York Heart Association (NYHA) Functional ClassificationDocumento1 paginaNew York Heart Association (NYHA) Functional ClassificationEjanZulqadMaulanaNessuna valutazione finora
- Angina Pectoris PDFDocumento22 pagineAngina Pectoris PDFHaSan Z. MustafaNessuna valutazione finora
- Mid Term Exam For Assessment RehabilitationDocumento11 pagineMid Term Exam For Assessment RehabilitationchardeaNessuna valutazione finora
- Joint, Connective Tissue, and Bone Disorders and ManagementDocumento47 pagineJoint, Connective Tissue, and Bone Disorders and ManagementAmbreen TariqNessuna valutazione finora
- An Insight On Poverty Reduction and Health Inequalities in The Philippines: Social Determinants, Constraints, and OpportunitiesDocumento84 pagineAn Insight On Poverty Reduction and Health Inequalities in The Philippines: Social Determinants, Constraints, and OpportunitiesJohn Vincent Pagaddu100% (1)
- 3a - Overview of The Physiology of Pain and Systemic Causes of PainDocumento61 pagine3a - Overview of The Physiology of Pain and Systemic Causes of PainNafisa GulNessuna valutazione finora
- BPT Syllabus PDFDocumento116 pagineBPT Syllabus PDFAnup Cee Key100% (1)
- Diabetic FootDocumento104 pagineDiabetic FootadibeuutNessuna valutazione finora
- Geriatrics Sir ZahidDocumento575 pagineGeriatrics Sir ZahidSheeraz ShahzadNessuna valutazione finora
- CHOLESTROLDocumento16 pagineCHOLESTROLalirifan2100% (1)
- Case Study: MYXEDEMATOUS COMADocumento5 pagineCase Study: MYXEDEMATOUS COMAjisooNessuna valutazione finora
- Cardiac RehabilitationDocumento2 pagineCardiac RehabilitationMarilou Sadsad VillalobosNessuna valutazione finora
- Anatomy and Physiology Unit 10 Test Review KEYDocumento7 pagineAnatomy and Physiology Unit 10 Test Review KEYsenjicsNessuna valutazione finora
- ASSESMENT Cardiorespiratory FitnessDocumento40 pagineASSESMENT Cardiorespiratory Fitnessmsalungin1313Nessuna valutazione finora
- Recreation Pertains To Activities Done For Leisure To Promote A Person's Well-Being and Growth. It Brings About A Sense ofDocumento2 pagineRecreation Pertains To Activities Done For Leisure To Promote A Person's Well-Being and Growth. It Brings About A Sense ofJee En BeeNessuna valutazione finora
- Hypomagnesemia Mcqs PDFDocumento7 pagineHypomagnesemia Mcqs PDFSyed Ali AkbarNessuna valutazione finora
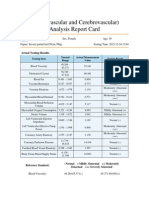
- Cardiovascular and CerebrovascularDocumento6 pagineCardiovascular and CerebrovascularJoshelle B. Bancilo0% (1)
- Health and Wellness 2 Roll No 5Documento16 pagineHealth and Wellness 2 Roll No 5Ansa MalikNessuna valutazione finora
- HEC Recognized Curriculum For DOctor of Physdiotherapy 2010Documento196 pagineHEC Recognized Curriculum For DOctor of Physdiotherapy 2010Faisal QureshiNessuna valutazione finora
- Lec 3 Pain Type and Viscrogenic Pain Pattern 3Documento68 pagineLec 3 Pain Type and Viscrogenic Pain Pattern 3Hina AnwarNessuna valutazione finora
- 2nd Periodical TestDocumento17 pagine2nd Periodical TestJhuvzCLunaNessuna valutazione finora
- Case 12 Stroke Rev'd ShorterDocumento3 pagineCase 12 Stroke Rev'd Shorterng100% (1)
- Drugs and Doping in SportDocumento39 pagineDrugs and Doping in SportAbhijit Sharma100% (1)
- Epidemiology of Coronary Heart Disease and Acute Coronary SyndromeDocumento6 pagineEpidemiology of Coronary Heart Disease and Acute Coronary SyndromeAnonymous GpgioaDAbNessuna valutazione finora
- ICM Syllabus Spring Semester-FinalDocumento21 pagineICM Syllabus Spring Semester-FinalRahman AkinlusiNessuna valutazione finora
- AFPMC V. Luna General Hospital: Case StudyDocumento27 pagineAFPMC V. Luna General Hospital: Case StudyLemuel GuevarraNessuna valutazione finora
- 3-Introduction To The Interviewing ProcessDocumento23 pagine3-Introduction To The Interviewing Processkashmala afzalNessuna valutazione finora
- Leadership Discussion Board Mod 4Documento1 paginaLeadership Discussion Board Mod 4api-396919069Nessuna valutazione finora
- New Patient Assessment FormDocumento2 pagineNew Patient Assessment Formapi-353132602Nessuna valutazione finora
- Cardiac Rehab GuidelinesDocumento265 pagineCardiac Rehab Guidelinesdorothy_put100% (1)
- Unstable AnginaDocumento5 pagineUnstable AnginaAria AlysisNessuna valutazione finora
- Cardiovascular 4416Documento5 pagineCardiovascular 4416api-3703191Nessuna valutazione finora
- Diabetes: Causes, Symptoms and TreatmentsDocumento4 pagineDiabetes: Causes, Symptoms and TreatmentsAbdullah BazryNessuna valutazione finora
- Arrhythmias Teacher GuideDocumento12 pagineArrhythmias Teacher GuideMayer Rosenberg100% (3)
- Reading Sub-Test - Question Paper: Part CDocumento10 pagineReading Sub-Test - Question Paper: Part CSarah Jane PetalioNessuna valutazione finora
- Aha Manejo Iam en Cirugia No Cardiaca 2021Documento19 pagineAha Manejo Iam en Cirugia No Cardiaca 2021dullzineaaNessuna valutazione finora
- Acute Coronary SyndromeDocumento18 pagineAcute Coronary SyndromeKartika RahmawatiNessuna valutazione finora
- Philippine Eagles HymnDocumento2 paginePhilippine Eagles Hymndanny17ph100% (8)
- Rehab in The Time of Drug WarDocumento5 pagineRehab in The Time of Drug Wardanny17phNessuna valutazione finora
- The Ongoing Evolution of Rotaract Is Redefining Its Place Within RotaryDocumento6 pagineThe Ongoing Evolution of Rotaract Is Redefining Its Place Within Rotarydanny17phNessuna valutazione finora
- Hormone Replacement Therapy The Right Choice For Your PatientDocumento9 pagineHormone Replacement Therapy The Right Choice For Your Patientdanny17phNessuna valutazione finora
- Bond Investing Guide 1 To 3Documento4 pagineBond Investing Guide 1 To 3danny17phNessuna valutazione finora
- Molave Hotel: Carlitos HostelDocumento2 pagineMolave Hotel: Carlitos Hosteldanny17phNessuna valutazione finora
- How Should We Diagnose and Treat Osteoarthritis of The KneeDocumento3 pagineHow Should We Diagnose and Treat Osteoarthritis of The Kneedanny17phNessuna valutazione finora
- Foreign Body in The Eye: Unit No. 3ADocumento2 pagineForeign Body in The Eye: Unit No. 3Adanny17phNessuna valutazione finora
- Neck Mass How Would You TreatDocumento5 pagineNeck Mass How Would You Treatdanny17phNessuna valutazione finora
- Dyspnea, PancytopeniaDocumento4 pagineDyspnea, Pancytopeniadanny17phNessuna valutazione finora
- Facilitators Meeting Agenda For The Training On The ImplementationDocumento1 paginaFacilitators Meeting Agenda For The Training On The Implementationdanny17phNessuna valutazione finora
- How Should We Evaluate Constipation in Infants and ChildrenDocumento3 pagineHow Should We Evaluate Constipation in Infants and Childrendanny17phNessuna valutazione finora
- Correlation Between Glycated Haemoglobin and GlucoseDocumento6 pagineCorrelation Between Glycated Haemoglobin and Glucosedanny17phNessuna valutazione finora
- The Pharmacotherapy of Chronic Obstructive Pulmonary Disease in The ElderlyDocumento14 pagineThe Pharmacotherapy of Chronic Obstructive Pulmonary Disease in The Elderlydanny17phNessuna valutazione finora
- Rosa History RevisedDocumento2 pagineRosa History Reviseddanny17ph100% (1)
- Order Set: Abdominal Pain OrdersDocumento3 pagineOrder Set: Abdominal Pain Ordersdanny17phNessuna valutazione finora
- Rosa AwardeesDocumento1 paginaRosa Awardeesdanny17phNessuna valutazione finora
- Diverticular Disease: Diverticulitis, Bleeding, and FistulaDocumento8 pagineDiverticular Disease: Diverticulitis, Bleeding, and FistulaakashkumarpanwarNessuna valutazione finora
- 12 Lead Ecg Placements The HeartDocumento9 pagine12 Lead Ecg Placements The HeartFalusi Blessing OlaideNessuna valutazione finora
- Rift Valley FeverDocumento9 pagineRift Valley Feverapi-390015550Nessuna valutazione finora
- Lab Manual 11102016 PDFDocumento239 pagineLab Manual 11102016 PDFDesyAyu DzulfaAry EomutNessuna valutazione finora
- Imogene King PPT CompleteDocumento21 pagineImogene King PPT CompleteAllayna Marie Fernandez100% (2)
- Antibiotic Grouping by MechanismDocumento11 pagineAntibiotic Grouping by MechanismalterNessuna valutazione finora
- Developmental Dysplasia of The Hip: Dr. Bassel El-Osta SPR Trauma & OrthopaedicsDocumento71 pagineDevelopmental Dysplasia of The Hip: Dr. Bassel El-Osta SPR Trauma & OrthopaedicsvadimmadanNessuna valutazione finora
- SL Report-278574812Documento2 pagineSL Report-278574812SiddharthNessuna valutazione finora
- KASP Package RateDocumento502 pagineKASP Package RateAnoop VijayakumarNessuna valutazione finora
- Hubungan Temuan MRI Dengan Klinis Nyeri Pasien Herniasi Nukleus Pulposus LumbalDocumento13 pagineHubungan Temuan MRI Dengan Klinis Nyeri Pasien Herniasi Nukleus Pulposus LumbalHendrawanDianAgungWicaksanaNessuna valutazione finora
- Anaphy BipoDocumento3 pagineAnaphy BipoRhea RaveloNessuna valutazione finora
- Thesis Setup Error PelvicDocumento43 pagineThesis Setup Error PelvichandiaviNessuna valutazione finora
- Wrist / Fingers Injuries: DR - Shafaq Shahid Lecturer DPT, Ms-OmptDocumento59 pagineWrist / Fingers Injuries: DR - Shafaq Shahid Lecturer DPT, Ms-OmptNabiha AjmalNessuna valutazione finora
- Movement DisordersDocumento18 pagineMovement DisordersFaisal BudisasmitaNessuna valutazione finora
- PisaDocumento2 paginePisaMrMoezesNessuna valutazione finora
- Presentor: DR - Kumar Moderator: DR - VamsidharDocumento71 paginePresentor: DR - Kumar Moderator: DR - VamsidharJayaprakash KuppusamyNessuna valutazione finora
- Chapter 1. History and Physical Examination - Art and ScienceDocumento3 pagineChapter 1. History and Physical Examination - Art and SciencecarolineNessuna valutazione finora
- Behavior TherapyDocumento9 pagineBehavior TherapyHamika VijanNessuna valutazione finora
- Drama Script From Group 3Documento5 pagineDrama Script From Group 3Rani NadyaNessuna valutazione finora
- Clinical Manifestations and Diagnosis of Intraventricular Hemorrhage in The NewbornDocumento12 pagineClinical Manifestations and Diagnosis of Intraventricular Hemorrhage in The NewbornAnonymous Xmb6QQvRNessuna valutazione finora
- Colloidal Silver, Scarlet Fever and Streptococcus Pyogenes - A New Plague Begins To SpreadDocumento8 pagineColloidal Silver, Scarlet Fever and Streptococcus Pyogenes - A New Plague Begins To SpreaddropsyNessuna valutazione finora
- Pregnancy CKDDocumento6 paginePregnancy CKDRajiv MedankiNessuna valutazione finora
- Proses Persalinan Normal Eb1Documento43 pagineProses Persalinan Normal Eb1Cici RahmaNessuna valutazione finora
- Birth TraumaDocumento44 pagineBirth TraumasreekalaNessuna valutazione finora
- Micu MedsDocumento3 pagineMicu MedsanreilegardeNessuna valutazione finora
- Assessment of Knowledge of Public On Coronary Artery Disease, Hypertension and Diabetes MellitusDocumento5 pagineAssessment of Knowledge of Public On Coronary Artery Disease, Hypertension and Diabetes MellitusMythili MuthappaNessuna valutazione finora
- Volunteering and Health Literature ReviewDocumento38 pagineVolunteering and Health Literature ReviewNCVO100% (1)
- Regional Sales Manager Medical Devices in Dallas FT Worth TX Resume James MooreDocumento2 pagineRegional Sales Manager Medical Devices in Dallas FT Worth TX Resume James MooreJamesMoore2Nessuna valutazione finora
- Vancomycin Dosing and Monitoring in AdultsDocumento1 paginaVancomycin Dosing and Monitoring in AdultsjulialeoNessuna valutazione finora
- Health Cloud DatasheetDocumento2 pagineHealth Cloud DatasheetMadhuri MalayathiNessuna valutazione finora