Potrebbero piacerti anche
- Patrick Califia Speaking Sex To Power Perverts Freethinkers and The Politics of Sex The Politics of Pleasure and PerversityDocumento443 paginePatrick Califia Speaking Sex To Power Perverts Freethinkers and The Politics of Sex The Politics of Pleasure and PerversityStefanos PopofNessuna valutazione finora
- Application Form Clinical Laboratory PDFDocumento6 pagineApplication Form Clinical Laboratory PDFRhodora Benipayo100% (1)
- CS Form No. 6 Revised 2020 Application For Leave Fillable 1Documento2 pagineCS Form No. 6 Revised 2020 Application For Leave Fillable 1Leo Artemio PuertosNessuna valutazione finora
- PM PillarDocumento56 paginePM PillarNavneet Sharma75% (4)
- Soil Mechanics Lecture 1Documento86 pagineSoil Mechanics Lecture 1Ammar Ayub100% (2)
- 1 - Client ID and Clinical File Checklist9-10Documento1 pagina1 - Client ID and Clinical File Checklist9-10Rudy KolderNessuna valutazione finora
- On The Job Manual LLCCDocumento40 pagineOn The Job Manual LLCCRicson Bondad100% (1)
- Application For License To Operate A General Clinical LaboratoryDocumento6 pagineApplication For License To Operate A General Clinical LaboratoryJasper LimNessuna valutazione finora
- Soa PhilhealthDocumento1 paginaSoa PhilhealthDanicaNessuna valutazione finora
- Statement of Acoount For Animal Bite Treatment CenterDocumento1 paginaStatement of Acoount For Animal Bite Treatment CenterMHIEMHOI100% (1)
- CS Form No. 6 Revised 2020 Application For Leave FillableDocumento2 pagineCS Form No. 6 Revised 2020 Application For Leave FillableXJ Bhevz OlsNessuna valutazione finora
- MMCHD CS Form No 6, Revised 2020 (Application For Leave) (Fillable)Documento3 pagineMMCHD CS Form No 6, Revised 2020 (Application For Leave) (Fillable)Riza Montecillo TubatNessuna valutazione finora
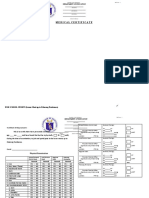
- Palaro 2009 Medical CertificateDocumento1 paginaPalaro 2009 Medical CertificateHari Ng Sablay100% (1)
- Form 6 LEAVE DeoganiDocumento2 pagineForm 6 LEAVE DeoganiDeogani GarguenaNessuna valutazione finora
- New Leave FormDocumento34 pagineNew Leave FormLyre-Ann HuervasNessuna valutazione finora
- New Leave Form 2020 ProgramDocumento2 pagineNew Leave Form 2020 ProgramMarife TremedalNessuna valutazione finora
- Statement of Account For TuberculosisDocumento1 paginaStatement of Account For TuberculosisMHIEMHOINessuna valutazione finora
- Medical CertificateDocumento1 paginaMedical CertificateJM Llameg IINessuna valutazione finora
- CS Form No. 6, Revised 2020 (Application For Leave) (Fillable) - 1Documento1 paginaCS Form No. 6, Revised 2020 (Application For Leave) (Fillable) - 1Acmad PangandamanNessuna valutazione finora
- Form-6 2023Documento2 pagineForm-6 2023Chaselle PortesNessuna valutazione finora
- Leave Form New 2021Documento2 pagineLeave Form New 2021DIVINE JES ALFEREZNessuna valutazione finora
- Form 6 Leave LJ EleccionDocumento2 pagineForm 6 Leave LJ EleccionDeogani GarguenaNessuna valutazione finora
- CS Form No. 6 Revised 2020 Application For Leave FillableDocumento2 pagineCS Form No. 6 Revised 2020 Application For Leave FillabledorisdeananeasNessuna valutazione finora
- C21 Listing Checklist - Blue SheetDocumento2 pagineC21 Listing Checklist - Blue SheetJana WhitlockNessuna valutazione finora
- All BFM 2002Documento12 pagineAll BFM 2002HEMATOLOGYCARE DR SK GUPTANessuna valutazione finora
- CS Form No. 6 Revised 2020 Application For Leave Fillable Final2021Documento2 pagineCS Form No. 6 Revised 2020 Application For Leave Fillable Final2021Riezl BachillerNessuna valutazione finora
- Clinic 5Documento1 paginaClinic 5nandyanuaNessuna valutazione finora
- Leave FormDocumento1 paginaLeave FormBfp MapanasNessuna valutazione finora
- RRT Evaluation FormDocumento1 paginaRRT Evaluation FormNurul IkmaliyahNessuna valutazione finora
- Application For LeaveDocumento2 pagineApplication For LeaveChristine Joy LozaresNessuna valutazione finora
- New Form 6 Leave Form TEACHERSDocumento2 pagineNew Form 6 Leave Form TEACHERSmarites mercedNessuna valutazione finora
- CS Form No. 6 Revised 2020 Application For Leave2021Documento2 pagineCS Form No. 6 Revised 2020 Application For Leave2021Jo Baraquiel100% (2)
- Maternity Leave FormDocumento2 pagineMaternity Leave FormElein Rosinas GantonNessuna valutazione finora
- Application For Leave: Philippine Statistics AuthorityDocumento1 paginaApplication For Leave: Philippine Statistics AuthorityNah ReeNessuna valutazione finora
- Ipsg Goal 2Documento1 paginaIpsg Goal 2Jl ANessuna valutazione finora
- New Format Form 6Documento2 pagineNew Format Form 6rosette UngabNessuna valutazione finora
- CS Form No. 6 Revised 2020 Application For Leave Fillable 1Documento4 pagineCS Form No. 6 Revised 2020 Application For Leave Fillable 1Joevan VillaflorNessuna valutazione finora
- Medical Certificate Form PalaroDocumento1 paginaMedical Certificate Form PalaroLeslie CastilloNessuna valutazione finora
- Medical Certificate 2010 PalaroDocumento1 paginaMedical Certificate 2010 PalaroJeoffrey Lance UsabalNessuna valutazione finora
- Medical Certificate 2010 PalaroDocumento1 paginaMedical Certificate 2010 PalaroJeoffrey Lance Usabal0% (1)
- Medical Certificate 2010 PalaroDocumento1 paginaMedical Certificate 2010 PalaroJeoffrey Lance UsabalNessuna valutazione finora
- Application For Leave Revised 2020Documento6 pagineApplication For Leave Revised 2020URIKA MARIE ISIDNessuna valutazione finora
- CS Form No. 6 Revised 2020 Application For Leave Fillable 1Documento4 pagineCS Form No. 6 Revised 2020 Application For Leave Fillable 1Kiven ArdenoNessuna valutazione finora
- Aor Reporting FormDocumento2 pagineAor Reporting FormPaidiHasanNessuna valutazione finora
- CS Form No. 6, Revised 2020 (Application For Leave) (Secured)Documento3 pagineCS Form No. 6, Revised 2020 (Application For Leave) (Secured)Lemmy Constantino DulnuanNessuna valutazione finora
- Leave Application FormDocumento2 pagineLeave Application FormAntolin Bongcawel (Anton)Nessuna valutazione finora
- CS Form No. 6 Revised 2023Documento2 pagineCS Form No. 6 Revised 2023ANA CELLA MARZONessuna valutazione finora
- Patient Treatment Record (White Card)Documento6 paginePatient Treatment Record (White Card)Srinu MakkenaNessuna valutazione finora
- Leave Form For SH or Principal (1 Day-60 Days)Documento3 pagineLeave Form For SH or Principal (1 Day-60 Days)mark joseph quichoNessuna valutazione finora
- 2 CopiesDocumento1 pagina2 CopiesBency MendozaNessuna valutazione finora
- MTLBE Assignments NBS, Water Ana & Organ DonDocumento2 pagineMTLBE Assignments NBS, Water Ana & Organ DonFait HeeNessuna valutazione finora
- BLANK CS Form No. 6, Revised 2020 (Application For Leave)Documento1 paginaBLANK CS Form No. 6, Revised 2020 (Application For Leave)vimNessuna valutazione finora
- CS Form No. 6 Revised 2020 Application For Leave Fillable 1Documento4 pagineCS Form No. 6 Revised 2020 Application For Leave Fillable 1Gabriel De Los ReyesNessuna valutazione finora
- PDF Programming Manual Fundamentals SiemensDocumento612 paginePDF Programming Manual Fundamentals SiemensPat CarpaNessuna valutazione finora
- 1leave Atty. SumatraDocumento5 pagine1leave Atty. SumatraRobee Camille SumatraNessuna valutazione finora
- CS Form No. 6, Revised 2020 (Application For Leave) - UPVDocumento2 pagineCS Form No. 6, Revised 2020 (Application For Leave) - UPVEmaylyn Villegas100% (1)
- CS Form No. 6 Revised 2020 Application For Leave Fillable 1Documento2 pagineCS Form No. 6 Revised 2020 Application For Leave Fillable 1LaoMedranoNessuna valutazione finora
- Application For Leave: Division of Ozamiz CityDocumento2 pagineApplication For Leave: Division of Ozamiz CityShemae ObniNessuna valutazione finora
- CS Form No. 6, Revised 2020 (Application For Leave) (Fillable)Documento2 pagineCS Form No. 6, Revised 2020 (Application For Leave) (Fillable)JOANNA ROSE DELLOMAS-JAVILLONARNessuna valutazione finora
- Division of Cagayan de Oro City: Application For LeaveDocumento2 pagineDivision of Cagayan de Oro City: Application For LeaveGraceyNessuna valutazione finora
- Medical Certificate: Department of EducationDocumento2 pagineMedical Certificate: Department of EducationSerLem WellNessuna valutazione finora
- CS Form No. 6 Revised 2020 Application For Leave FillableDocumento3 pagineCS Form No. 6 Revised 2020 Application For Leave FillableYelhsa RamosNessuna valutazione finora
- Asset-backed Securitization and the Financial Crisis: The Product and Market Functions of Asset-backed Securitization: Retrospect and ProspectDa EverandAsset-backed Securitization and the Financial Crisis: The Product and Market Functions of Asset-backed Securitization: Retrospect and ProspectNessuna valutazione finora
- Top 10 Best Jazz Songs - TheTopTens®Documento5 pagineTop 10 Best Jazz Songs - TheTopTens®Rudy KolderNessuna valutazione finora
- Top Ten Best Instrumental Songs - TheTopTens®Documento5 pagineTop Ten Best Instrumental Songs - TheTopTens®Rudy KolderNessuna valutazione finora
- Psychology 101 Semester ProjectDocumento1 paginaPsychology 101 Semester ProjectRudy KolderNessuna valutazione finora
- What Damages Can You Get If Your Employer Retaliates Against YouDocumento5 pagineWhat Damages Can You Get If Your Employer Retaliates Against YouRudy KolderNessuna valutazione finora
- Research Opportunities Based On Your Unreported Genetics - 23andmeDocumento2 pagineResearch Opportunities Based On Your Unreported Genetics - 23andmeRudy KolderNessuna valutazione finora
- Top Ten Best Country Songs of All Time - TheTopTens®Documento7 pagineTop Ten Best Country Songs of All Time - TheTopTens®Rudy KolderNessuna valutazione finora
- The Mid-Engine Corvette C8.R Wants To Take The Racing World by StormDocumento12 pagineThe Mid-Engine Corvette C8.R Wants To Take The Racing World by StormRudy KolderNessuna valutazione finora
- GENERIC RADIO WORKSHOP OTR SCRIPT The BickersonsDocumento7 pagineGENERIC RADIO WORKSHOP OTR SCRIPT The BickersonsRudy Kolder100% (1)
- The Senate GOP Tax Bill, Explained - The Washington PostDocumento6 pagineThe Senate GOP Tax Bill, Explained - The Washington PostRudy KolderNessuna valutazione finora
- Top Ten Best Instrumental Songs - TheTopTens®Documento5 pagineTop Ten Best Instrumental Songs - TheTopTens®Rudy KolderNessuna valutazione finora
- Things Ain't What They Used To Be - Jim HallDocumento3 pagineThings Ain't What They Used To Be - Jim HallmabbagliatiNessuna valutazione finora
- Top Ten Best Country Songs of All Time - TheTopTens®Documento7 pagineTop Ten Best Country Songs of All Time - TheTopTens®Rudy KolderNessuna valutazione finora
- Thank You - Medicare Info - Medicare InfoDocumento4 pagineThank You - Medicare Info - Medicare InfoRudy KolderNessuna valutazione finora
- Pentagon Security MeasuresDocumento1 paginaPentagon Security MeasuresRudy KolderNessuna valutazione finora
- Misty - Chord Melody & Solo Studies (With Backing Track)Documento51 pagineMisty - Chord Melody & Solo Studies (With Backing Track)Rudy Kolder80% (5)
- Your Cheating HeartDocumento1 paginaYour Cheating HeartRudy KolderNessuna valutazione finora
- Legislature Chooses Savings Over Rights in Prison Contract - News Columns - WyoFile6-6-17Documento8 pagineLegislature Chooses Savings Over Rights in Prison Contract - News Columns - WyoFile6-6-17Rudy KolderNessuna valutazione finora
- Fibber's Christmas TreeDocumento15 pagineFibber's Christmas TreeRudy KolderNessuna valutazione finora
- How Much Income Will $100,000 Portfolio Pay MeDocumento10 pagineHow Much Income Will $100,000 Portfolio Pay MeRudy KolderNessuna valutazione finora
- Jazzguitar - Be Giant StepsDocumento23 pagineJazzguitar - Be Giant StepsRudy Kolder100% (1)
- Your Cheating HeartDocumento1 paginaYour Cheating HeartRudy KolderNessuna valutazione finora
- Cannonball Adderley Mercy Mercy MercyDocumento1 paginaCannonball Adderley Mercy Mercy MercyRudy KolderNessuna valutazione finora
- What Damages Can You Get If Your Employer Retaliates Against YouDocumento5 pagineWhat Damages Can You Get If Your Employer Retaliates Against YouRudy KolderNessuna valutazione finora
- How To Make Homemade Veggie Burgers Like A Pro - EatingWellDocumento5 pagineHow To Make Homemade Veggie Burgers Like A Pro - EatingWellRudy KolderNessuna valutazione finora
- Best Chet Atkins Songs - Top Ten List - TheTopTens®Documento2 pagineBest Chet Atkins Songs - Top Ten List - TheTopTens®Rudy KolderNessuna valutazione finora
- Mercymercy PDFDocumento3 pagineMercymercy PDF稲田貴士Nessuna valutazione finora
- 15-Minute HIIT Workout To Beat Belly Fat - Shape MagazineDocumento17 pagine15-Minute HIIT Workout To Beat Belly Fat - Shape MagazineRudy KolderNessuna valutazione finora
- Groundbreaking New Study Sheds Doubt On Many Heart ProceduresDocumento16 pagineGroundbreaking New Study Sheds Doubt On Many Heart ProceduresRudy KolderNessuna valutazione finora
- Aortic Valve Repair and Aortic Valve Replacement - Mayo ClinicDocumento13 pagineAortic Valve Repair and Aortic Valve Replacement - Mayo ClinicRudy KolderNessuna valutazione finora
- Img 20191015 0002 PDFDocumento1 paginaImg 20191015 0002 PDFRudy KolderNessuna valutazione finora
- DR - Vyshnavi Ts ResumeDocumento2 pagineDR - Vyshnavi Ts ResumeSuraj SingriNessuna valutazione finora
- Soc5352 1331Documento4 pagineSoc5352 1331ChinNessuna valutazione finora
- 327 - Mil-C-15074Documento2 pagine327 - Mil-C-15074Bianca MoraisNessuna valutazione finora
- BPT Notes Applied PsychologyDocumento36 pagineBPT Notes Applied PsychologyVivek Chandra0% (1)
- Techno LabDocumento3 pagineTechno LabA M FaisalNessuna valutazione finora
- Instructions For Assembling Your Owners ManualDocumento8 pagineInstructions For Assembling Your Owners ManualJim PowersNessuna valutazione finora
- Home Composting Brochure - Connecticut USADocumento2 pagineHome Composting Brochure - Connecticut USAPennsylvania Association for Sustainable AgricultureNessuna valutazione finora
- Transmission Line BOQ VIMPDocumento72 pagineTransmission Line BOQ VIMPkajale_shrikant2325Nessuna valutazione finora
- New Microsoft Office Word DocumentDocumento3 pagineNew Microsoft Office Word DocumentSunija SelvamNessuna valutazione finora
- TZ150-03 Service Manual - ChopperDocumento42 pagineTZ150-03 Service Manual - ChopperMax Dean Araújo FernandesNessuna valutazione finora
- Autodrill Satellite ManualDocumento37 pagineAutodrill Satellite ManualmiguelNessuna valutazione finora
- Curriculum Guide: Exploratory Course On Household ServicesDocumento5 pagineCurriculum Guide: Exploratory Course On Household ServicesJovanni Mancao PodadorNessuna valutazione finora
- Denon DHT-T100 Ver 3 PDFDocumento34 pagineDenon DHT-T100 Ver 3 PDFboroda241083% (6)
- Valerie Tillard Murder: Probable CauseDocumento11 pagineValerie Tillard Murder: Probable CauseLeigh EganNessuna valutazione finora
- Industrial Diesel Generator Set - 50 HZ: General Specifications KOHLER Premium QualityDocumento7 pagineIndustrial Diesel Generator Set - 50 HZ: General Specifications KOHLER Premium QualityABCD123655Nessuna valutazione finora
- Industrialisation by InvitationDocumento10 pagineIndustrialisation by InvitationkimberlyNessuna valutazione finora
- Selection and Ranking of Rail Vehicle Components For Optimal Lightweighting Using Composite MaterialsDocumento14 pagineSelection and Ranking of Rail Vehicle Components For Optimal Lightweighting Using Composite MaterialsAwan AJaNessuna valutazione finora
- Plumbing Engineering Design Handbook, Vol 1 ASPEDocumento422 paginePlumbing Engineering Design Handbook, Vol 1 ASPEMichelle NataliNessuna valutazione finora
- Northern NVProvider DirectoryDocumento82 pagineNorthern NVProvider DirectoryGuru NandeshwarNessuna valutazione finora
- Civil EngineeringDocumento13 pagineCivil EngineeringMahmoud OuryemchiNessuna valutazione finora
- Leon County Sheriff'S Office Daily Booking Report 18-Oct-2020 Page 1 of 3Documento3 pagineLeon County Sheriff'S Office Daily Booking Report 18-Oct-2020 Page 1 of 3WCTV Digital TeamNessuna valutazione finora
- Carbonyl Compounds: Unit 4 Rates, Equilibria and Further Organic ChemistryDocumento5 pagineCarbonyl Compounds: Unit 4 Rates, Equilibria and Further Organic ChemistryKirusaanth SathiyathasanNessuna valutazione finora
- 21 Day Level Up Challenge My PathDocumento52 pagine21 Day Level Up Challenge My PathDavid Stark100% (1)
- Construction of Genomic and cDNA Libraries-AmitDocumento10 pagineConstruction of Genomic and cDNA Libraries-AmitPrashant BajpaiNessuna valutazione finora
- Why Is ICS Important For Schools?Documento8 pagineWhy Is ICS Important For Schools?Spit FireNessuna valutazione finora
- Lean Six Sigma Green BeltDocumento7 pagineLean Six Sigma Green Beltmulpuru sai snehaNessuna valutazione finora
- An Assestment of The Trinidad and Tobago Health Care SystemDocumento4 pagineAn Assestment of The Trinidad and Tobago Health Care SystemMarli MoiseNessuna valutazione finora