Documenti di Didattica
Documenti di Professioni
Documenti di Cultura
Conversion Laparoscopy To Laparotomy For Total Hysterectomy
Caricato da
Iqra AnugerahTitolo originale
Copyright
Formati disponibili
Condividi questo documento
Condividi o incorpora il documento
Hai trovato utile questo documento?
Questo contenuto è inappropriato?
Segnala questo documentoCopyright:
Formati disponibili
Conversion Laparoscopy To Laparotomy For Total Hysterectomy
Caricato da
Iqra AnugerahCopyright:
Formati disponibili
Original Research
Risk Factors and Outcomes for Conversion to
Laparotomy of Laparoscopic Hysterectomy
in Benign Gynecology
Courtney S. Lim, MD, Erika L. Mowers, MD, Nichole Mahnert, MD, Bethany D. Skinner, MD,
Neil Kamdar, MA, Daniel M. Morgan, MD, and Sawsan As-Sanie, MD, MPH
OBJECTIVE: To estimate the incidence and factors for surgeons (adjusted OR 0.66, 95% CI 0.47–0.92) with
conversion to laparotomy in women scheduled for a predicted risk of conversion of 1.4% compared with
laparoscopic hysterectomy for benign gynecologic indi- 2.25% (P5.015). Conversion was associated with moder-
cations and to examine the effect of conversion on ate or severe adhesive disease and increasing specimen
patient outcomes. weight. Conversion was associated with increased rates
METHODS: A retrospective cohort study of a Michigan of surgical site infection, blood transfusion, severe sep-
multicenter prospective database was abstracted from sis, and reoperation.
January 1, 2013, through July 2, 2014. Participants were CONCLUSION: This analysis demonstrates that conver-
collected from an all-payer quality and safety database sion to laparotomy is associated with increased odds of
maintained by the Michigan Surgical Quality Collabora- postoperative morbidity, and robotic assistance and
tive. Women with a preoperative indication of cancer or surgeon volume are strongly associated with decreased
obstetric indications were excluded. A logistic regression odds of conversion.
model was used to calculate odds of conversion using (Obstet Gynecol 2016;128:1295–305)
patient preoperative and intraoperative attributes. DOI: 10.1097/AOG.0000000000001743
RESULTS: During the study period, 6,992 women
underwent an attempted laparoscopic hysterectomy
with 3.93% (n5275) converted to laparotomy. After ad-
justing for socioeconomic differences, hysterectomy
T he benefits of laparoscopic surgery are well known
and include shorter hospital stay, less postopera-
tive pain, quicker return to normal activities, fewer
indication, and intraoperative factors, there were wound infections, and decreased blood loss in com-
decreased odds of conversion to laparotomy with use parison with an abdominal approach.1 Given these
of robotic-assisted laparoscopy compared with tradi- clear benefits, the use of laparoscopy has increased
tional laparoscopy (adjusted odds ratio [OR] 0.14, 95% substantially and is the preferred approach when vag-
confidence interval [CI] 0.07–0.25) with a predicted risk inal hysterectomy is not feasible.2
of conversion of 0.8% compared with 5.4% (P,.001). Despite the increased utilization of laparoscopy
High-volume surgeons were less likely to convert to lap-
for hysterectomy, conversion to laparotomy (or “con-
arotomy compared with low- and medium-volume
version”) remains a risk and has been reported in 0–
19% of patients.3 Reported risk factors for conversion
From the Department of Obstetrics and Gynecology, University of Michigan, Ann
Arbor, Michigan.
include patient factors such as increasing age,3
increasing body mass index (BMI, calculated as
Presented at the 44th American Association of Gynecologic Laparoscopists Global
Congress on Minimally Invasive Gynecology, November 15–19, 2015, Las weight (kg)/[height (m)]2),3–5 history of abdominopel-
Vegas, Nevada. vic surgery,4 presence of adhesions,4–6 endometriosis
Corresponding author: Courtney S. Lim, MD, L4000 Women’s Hospital, 1500 E or leiomyomata,4 uterine weight3,5,6 as well as a less
Medical Center Drive, SPC 5276, Ann Arbor, MI 48109-5276; e-mail: experienced surgeon.3 However, these risk factors are
courtlim@med.umich.edu.
not consistently reported across all major studies,3–6
Financial Disclosure
The authors did not report any potential conflicts of interest.
and prior studies have not examined the effect of the
robotic surgical system. Furthermore, many of the
© 2016 by The American College of Obstetricians and Gynecologists. Published
by Wolters Kluwer Health, Inc. All rights reserved. prior studies are limited by small sample size and out-
ISSN: 0029-7844/16 comes from a single institution.
VOL. 128, NO. 6, DECEMBER 2016 OBSTETRICS & GYNECOLOGY 1295
Copyright ª by The American College of Obstetricians
and Gynecologists. Published by Wolters Kluwer Health, Inc.
Unauthorized reproduction of this article is prohibited.
The objective of this study was to evaluate the hysterectomy included traditional laparoscopy,
incidence and risk factors for conversion to laparot- robotic-assisted (or “robotic”), and laparoscopic-
omy for both traditional laparoscopic and robotic assisted vaginal approaches. Patients with a known
hysterectomy performed for benign indications using malignancy or obstetric indication were excluded
a statewide multicenter prospective database. Our from this analysis. Route of hysterectomy and conver-
secondary objective was to determine differences in sion to laparotomy were obtained from operative re-
30-day outcomes of women who had conversion to ports and intraoperative records. The objective of this
laparotomy. This information will enhance risk strat- study was to evaluate the incidence and risk factors for
ification and improve preoperative planning and conversion to laparotomy for both traditional laparo-
patient selection for hysterectomy. scopic and robotic-assisted laparoscopic hysterectomy
performed for benign gynecologic indications.
MATERIALS AND METHODS We evaluated patient preoperative and perioper-
All laparoscopic hysterectomies performed from ative characteristics. Patient demographics included
January 1, 2013, through July 2, 2014, in the Michigan age, parity, self-reported race (white or nonwhite), and
Surgical Quality Collaborative database were type of insurance at the time of surgery. The patient’s
included in this analysis. The selected timeframe insurance was classified as private, Medicaid, Medi-
reflected the most complete data set at the time of care, uninsured, or self-pay. Private insurance included
the analysis. The Michigan Surgical Quality Collab- Blue Cross Blue Shield of Michigan, Blue Care Net-
orative consists of 52 academic and community work, health maintenance organization plans, and
hospitals voluntarily participating in this collabora- other private insurance plans. Medicare included
tive. Sixty percentage are community-based. Funded Medicare only, Medicare with a supplemental plan
by Blue Cross and Blue Shield of Michigan/Blue Care such as Medigap insurance, or Medicare Advantage
Network, this represents approximately 30% of Mich- (Blue Cross Blue Shield or Blue Care Network of
igan hospitals, and it includes patients from all Michigan). Patients were considered to have Medicaid
insurance payers. At each participating hospital, if they had Medicaid or a health maintenance organi-
a trained, dedicated nurse researcher reviews the zation Medicaid plan. Uninsured and self-pay were
entire medical record and uses a standardized data reported but not considered for additional multivariate
collection instrument to abstract patient character- analysis as a result of small numbers.
istics, operative findings, complications, pathology Additional patient characteristics included med-
results, and 30-day postoperative outcomes. Data ical comorbidities (BMI, history of hypertension,
were abstracted from clinic and hospital notes, oper- deep vein thrombosis, preoperative blood transfu-
ative reports, and pathology reports. sion), American Society of Anesthesiologists physical
Cases collected in the Michigan Surgical Quality status classifications, surgical indications for hyster-
Collaborative database include general surgery pro- ectomy, and history of prior abdominal or pelvic
cedures (such as appendectomy, cholecystectomy, surgery. Surgical indications were determined based
colectomy) as well as hysterectomies. A standardized on the outpatient clinic notes, preoperative history,
data collection methodology is used to reduce sam- and physical or operative notes. These indications
pling bias. The year is divided into consecutive 8-day included abnormal uterine bleeding, leiomyomas,
cycles so that each cycle starts on a different day. The endometriosis, pelvic inflammatory disease, pelvic
intended effect is to promote surgeon sampling mass, chronic pelvic pain, and pelvic organ prolapse.
because it is common practice for surgeons to cluster Surgical indications were not mutually exclusive and
procedures on 1 or 2 days of the week. At each patients could have more than one indication. Intra-
hospital, the first 25 cases of a previously identified list operative information was based on operative notes
of Current Procedural Terminology codes of an 8-day and pathology notes. This included presence of
cycle are collected. The process of data abstraction abdominal or pelvic adhesions; presence of endome-
and methodology is routinely validated through triosis anywhere in the pelvis; presence of endome-
scheduled site visits, conference calls, and internal triosis on the uterus, ovaries, or fallopian tubes; type
audits. The University of Michigan institutional of hysterectomy performed (total compared with
review board provided “nonregulated” status to this supracervical); intraoperative complications; speci-
study (HUM00073978). men weight; estimated blood loss in milliliters; and
All benign hysterectomies that were initiated with procedure duration (incision to closure) in minutes.
laparoscopy during the study period within the The finding of unexpected malignancy, defined as
sample were included in this analysis. Laparoscopic hysterectomy performed for a benign indication and
1296 Lim et al Laparoscopic Hysterectomy and Conversion OBSTETRICS & GYNECOLOGY
Copyright ª by The American College of Obstetricians
and Gynecologists. Published by Wolters Kluwer Health, Inc.
Unauthorized reproduction of this article is prohibited.
final pathology identified a malignancy, was also the surgeons into equal volume-based tertiles of low,
included. Adhesions were classified as none or mild, medium, and high volume, as has previously been
moderate, or severe. None or mild adhesions were reported.7–9 The distribution of cases in each tertile
those that were not mentioned in the operative report can be seen in Table 1. The lowest volume tertile
or described as “few” or “limited.” Moderate adhe- contributed one to four hysterectomies in the 24-
sions were described as “some,” “multiple,” or month period, the intermediate-volume tertile
“many,” which may require lysis but do not impair contributed 5–17, and the high-volume tertile con-
the ability to do the operation. Severe adhesions were tributed 18 or more hysterectomies to the sample in
defined as “severe,” “dense,” “extensive,” “signifi- the prior 24 months. Given that the top tertile still
cant,” or “hostile”; taking an hour or more to lyse; included a low number of hysterectomies contrib-
or both. Severe adhesions were also defined as adhe- uted to the sample, we also examined ultrahigh-
sions prohibiting the planned procedure. volume surgeons by dividing the surgeons into those
Intraoperative complications included bowel, below the 75th percentile, 75th–89th percentile,
bladder, ureter, or vascular injury identified before 90th–94th percentile, 95th–98th percentile, and
completion of the hysterectomy. Specimen weight for 99th percentile or greater.
the uterus was measured in grams and classified as less Our secondary objective was to determine differ-
than 250, 250–499, 500–999 g, and greater than or ences in 30-day outcomes of women who had
equal to 1,000 g. Estimated blood loss was classified conversion to laparotomy, including the incidence of
as less than or equal to 100, 101–300, 301–500, 501– surgical site infection, postoperative transfusion,
1,000 mL, and greater than 1,000 mL. The duration of venous thromboembolism, readmission, and reopera-
surgery was split into 2-hour increments ranging from tion. This information was abstracted from hospital
less than 2 hours to greater than 6 hours. notes, office notes, laboratory results, radiology re-
Hospital characteristics included teaching status, sults, nursing notes, and emergency department
as defined by the 2012 American Hospital Association documentation. Surgical site infection definitions were
survey. Hospital bed size was defined as small (less based on definitions from the Centers for Disease
than 300 beds), medium (300–499 beds), and large Control and Prevention surveillance definition of
(500 beds or greater). health care-associated infections.10 Sepsis was defined
Surgeon volume was determined by the number as a recent history of new infection within 30 days
of all hysterectomies contributed to the Michigan postoperatively with any two of the following signs
Surgical Quality Collaborative sample in the prior and symptoms: temperature greater than 38.3°C or
24 months by each surgeon. This included abdom- less than 36°C, heart rate greater than 90 beats
inal, laparoscopic, and vaginal hysterectomies. This per minute, respiratory rate greater than 20 breaths
was used as a proxy for total surgeon volume per minute, white blood cell count greater than 12,000
because the Michigan Surgical Quality Collabora- cells per cubic millimeter or less than 4,000 cells per
tive does not capture every surgery performed at cubic millimeter, hyperglycemia (plasma glucose
each hospital, only the first 25 cases of each 8-day greater than 120 mg/dL) in the absence of diabetes,
data-capture cycle. Thus, a surgeon’s total annual or acutely altered mental status.11
caseload was not available and we considered this Distributions for continuous variables were
measure the best available proxy. We then exam- checked for normality looking at skew and kurtosis.
ined the distribution of surgeon volume and divided Continuous variables were examined and extreme
Table 1. Surgeon Volume by Equal Volume Tertiles Within the Michigan Surgical Quality Collaborative
Database
Tertile
Characteristic Low-Volume Middle-Volume High-Volume
No. of surgeons 284 301 303
No. of hysterectomies performed 615 2,184 9,323
Median no. of patients/surgeon 2 10 32
Lowest no. of cases/surgeon 1 5 18
Highest no. of cases/surgeon 4 17 258
VOL. 128, NO. 6, DECEMBER 2016 Lim et al Laparoscopic Hysterectomy and Conversion 1297
Copyright ª by The American College of Obstetricians
and Gynecologists. Published by Wolters Kluwer Health, Inc.
Unauthorized reproduction of this article is prohibited.
outliers were identified and removed. Approximately exclusion of cases for surgical approach (2,832
normally distributed data were reported as mean- abdominal, 1,343 vaginal, and one not discernible as
6standard deviation and nonparametric data were a result of a lack of data), an absence of pathology data
reported as median (interquartile range). Wilson- (232), gynecologic cancer (719), and obstetric indica-
binomial 95% confidence intervals were calculated tions (3), there were 6,992 hysterectomies eligible for
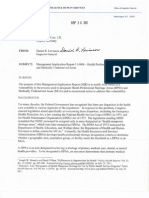
for proportions where appropriate. Descriptive anal- inclusion (Fig. 1). Of these, 6,717 were completed
ysis of categorical variables was conducted using x2 laparoscopically, and 275 were converted to an open
or Fisher exact test in the case of small cell sizes and procedure, for an overall rate of conversion of 3.93%.
Student t test or analysis of variance for continuous Seven of these cases were initiated emergently, and
variables as appropriate. none of those were converted to laparotomy.
Clinically relevant covariates were considered for Univariate analyses are shown in Tables 2 and 3.
multivariable logistic regression to examine likeli- Multiple preoperative characteristics (Table 2) were
hood of conversion from laparoscopy to laparotomy. associated with a significantly increased risk of conver-
Candidate covariates were assessed for missing data sion, including BMI greater than 30 and preoperative
and those with sufficient data for model development indication of leiomyomas, pelvic inflammatory dis-
were considered for analysis. Although parity and ease, or a pelvic mass. Factors that were associated
history of prior abdominal surgeries were clinically with decreased odds of conversion included previous
relevant covariates, they were excluded as a result of failure of an alternative treatment and preoperative
a significantly larger proportion of cases missing indication of pelvic organ prolapse. Compared with
compared with other covariates considered for bivar- moderate-volume surgeons, high-volume surgeons
iate and multivariate analyses. To account for clus- had lower odds of conversion in the univariate analy-
tering of patients within hospitals, Huber-White sis. In addition, the rate of conversion was significantly
robust standard errors were calculated for each of higher in traditional laparoscopy than robotic-assisted
the parameter estimates. For categorical variables laparoscopy (8.28% compared with 1.57%, P,.001).
with more than two categories, dummy variables Those who were self-pay or uninsured had an
were derived to measure direct effect sizes. Because increased odds of conversion compared with those
collinearity resulting from a significant correlation with private insurance (odds ratio [OR] 2.98, 95% con-
can dramatically affect parameter estimates and effect fidence interval [CI] 1.47–6.04). This was not included
sizes for the model, Spearman or Pearson correlation in the multivariate analysis as a result of small num-
matrices for all variables considered in a model were bers. Compared with those who underwent traditional
obtained. Iterative variable selection taking into laparoscopy, the group of patients undergoing robotic-
account collinearity and clinical relevance of selected assisted laparoscopic hysterectomy had characteristics
variables led to a reduced model with a strong C- associated with higher surgical complexity, with statis-
statistic (concordance). Final model diagnostics tically significantly higher BMIs and more frequent
included decile and quintile analysis comparing
observed and adjusted rates for conversion. Logistic
regression models were used to calculate the pre-
dicted incidence of conversion among robotic and
traditional laparoscopic cases adjusted for the varia-
bles included in the final model. A secondary analysis
was performed that fit the previously defined model
in addition to an interaction term. This interaction
term accounted for the relationship between surgical
approach (robotic-assisted laparoscopy compared
with traditional laparoscopy) and surgeon volume.
This was used to calculate the predicted risk of
conversion based on surgical approach across sur-
geon volume groups. Data analyses were performed
using Stata 14.0.
Fig. 1. Flow diagram of hysterectomies included in the
RESULTS analysis.
A total of 12,122 hysterectomies were available in the Lim. Laparoscopic Hysterectomy and Conversion. Obstet Gynecol
data set from January 1, 2013, to July 2, 2014. After 2016.
1298 Lim et al Laparoscopic Hysterectomy and Conversion OBSTETRICS & GYNECOLOGY
Copyright ª by The American College of Obstetricians
and Gynecologists. Published by Wolters Kluwer Health, Inc.
Unauthorized reproduction of this article is prohibited.
Table 2. Demographics and Preoperative Risk Factors and Risk of Conversion of Laparoscopic
Hysterectomy to Laparotomy
Total Completed Laparoscopically Conversion to Open Unadjusted OR
Characteristic (N56,992) (n56,717 [96.07]) (n5275 [3.93]) (95% CI) P
Age (y)
40 or younger 2,065 (29.53) 2,011 (97.38) 54 (2.62) Referent
Older than 40 and 4,271 (61.08) 4,074 (95.39) 197 (4.61) 1.80 (1.32–2.44) ,.001
60 or younger
Older than 60 656 (9.38) 632 (96.34) 24 (3.66) 1.41 (0.86–2.31) .165
Race
White 5,503 (78.70) 5,318 (96.64) 185 (3.36) Referent
Nonwhite 1,489 (21.30) 1,399 (93.96) 90 (6.04) 1.85 (1.43–2.40) ,.001
Insurance
Private 5,222 (79.37) 5,020 (96.13) 202 (3.87) Referent
Medicaid 676 (10.28) 650 (96.15) 26 (3.85) 0.99 (0.66–1.51) .978
Medicare 597 (9.07) 579 (96.98) 18 (3.02) 0.77 (0.47–1.26) .302
Uninsured or self- 84 (1.28) 75 (89.29) 9 (10.71) 2.98 (1.47–6.04) .002
pay
Missing 413 (5.91)
Use of robot
Traditional 2,464 (35.24) 2,260 (91.72) 204 (8.28) Referent
laparoscopic
Robotic 4,528 (64.76) 4,457 (98.43) 71 (1.57) 0.18 (0.13–0.23) ,.001
Prior pelvic surgery
No 2,701 (38.63) 2,601 (96.30) 100 (3.70) Referent
Yes 4,291 (61.37) 4,116 (95.92) 175 (4.08) 1.11 (0.86–1.42) .431
ASA class
1 761 (10.88) 739 (97.11) 22 (2.89) Referent
2 4,947 (70.75) 4,764 (96.30) 183 (3.70) 1.29 (0.82–2.02) .266
3 or greater 1,284 (18.36) 1,214 (94.55) 70 (5.45) 1.94 (1.19–3.15) .008
BMI (kg/m2)
Less than 25 1,711 (24.56) 1,666 (97.37) 45 (2.63) Referent
25 to less than 30 1,976 (28.36) 1,916 (96.96) 60 (3.04) 1.15 (0.78–1.71) .460
30 to less than 40 2,409 (34.57) 2,284 (94.81) 125 (5.19) 2.02 (1.43–2.87) ,.001
40 or greater 872 (12.51) 827 (94.84) 45 (5.16) 2.01 (1.32–3.07) .001
Missing 24 (0.34)
Prior alternative
treatment
No 2,893 (41.38) 2,757 (95.30) 136 (4.70) Referent
Yes 4,099 (58.62) 3,960 (96.61) 139 (3.39) 0.71 (0.56–0.91) .006
Indications for
hysterectomy
Abnormal uterine
bleeding
No 2,244 (32.09) 2,153 (95.94) 91 (4.06) Referent
Yes 4,748 (67.91) 4,564 (96.12) 184 (3.88) 0.95 (0.74–1.23) .718
Leiomyomas
No 4,297 (61.46) 4,168 (97.00) 129 (3.00) Referent
Yes 2,695 (38.54) 2,549 (94.58) 146 (5.42) 1.85 (1.45–2.36) ,.001
Endometriosis
No 6,012 (85.98) 5,775 (96.06) 237 (3.94) Referent
Yes 980 (14.02) 942 (96.12) 38 (3.88) 0.98 (0.69–1.39) .923
Pelvic inflammatory
disease
No 6,975 (99.76) 6,703 (96.10) 272 (3.90) Referent
Yes 17 (0.24) 14 (82.35) 3 (17.65) 5.28 (1.51–18.48) .009
Pelvic mass
No 6,514 (93.16) 6,267 (96.32) 247 (3.79) Referent
Yes 478 (6.84) 450 (94.14) 28 (5.86) 1.58 (1.06–2.36) .026
(continued )
VOL. 128, NO. 6, DECEMBER 2016 Lim et al Laparoscopic Hysterectomy and Conversion 1299
Copyright ª by The American College of Obstetricians
and Gynecologists. Published by Wolters Kluwer Health, Inc.
Unauthorized reproduction of this article is prohibited.
Table 2. Demographics and Preoperative Risk Factors and Risk of Conversion of Laparoscopic
Hysterectomy to Laparotomy (continued )
Total Completed Laparoscopically Conversion to Open Unadjusted OR
Characteristic (N56,992) (n56,717 [96.07]) (n5275 [3.93]) (95% CI) P
Chronic pelvic pain
No 4,158 (59.47) 3,993 (96.03) 165 (3.97) Referent
Yes 2,834 (40.53) 2,724 (96.12) 110 (3.88) 0.98 (0.76–1.25) .855
Pelvic organ
prolapse
No 6,140 (87.81) 5,878 (95.73) 262 (4.27) Referent
Yes 852 (12.19) 839 (98.47) 13 (1.53) 0.35 (0.20–0.61) ,.001
Bed size
Less than 300 2,617 (38.0) 2,534 (96.83) 83 (3.17) Referent
300–499 3,103 (45.06) 2,979 (96.0) 124 (4.0) 1.27 (0.96–1.69) .097
500 or greater 1,167 (16.94) 1,102 (94.43) 65 (5.57) 1.80 (1.29–2.51) .001
Missing 105 (1.50)
Teaching hospital
No 2,534 (36.79) 2,430 (95.90) 104 (4.10) Referent
Yes 4,353 (63.21) 4,185 (96.14) 168 (3.86) 0.94 (0.73–1.20) .615
Missing 105 (1.50)
Surgeon volume by
tertile
Low volume 278 (3.98) 265 (95.32) 13 (4.68) 0.63 (0.31–1.14) .127
Middle volume 1,143 (16.35) 1,060 (92.74) 83 (7.26) Referent
High volume 5,571 (79.68) 5,392 (96.79) 179 (3.21) 0.42 (0.32–0.55) ,.001
OR, odds ratio; CI, confidence interval; ASA, American Society of Anesthesiologists; BMI, body mass index.
Data are n (%) unless otherwise specified.
removal of the cervix and presence of endometriosis. modeling were age older than 40 years and 60 years
There was no difference on other covariates including or younger, BMI greater than or equal to 30, preop-
specimen weight and adhesion severity. erative indications of pelvic mass, presence of moder-
As shown in Table 3, intraoperative factors that ate or severe adhesions, and specimen weight greater
were associated with an increased odds of conversion than 250 g. The factors most strongly associated with
included presence of either moderate or severe adhe- decreased odds of conversion in the multivariate
sions or unexpected malignancy. Presence of endome- model were having a robotic procedure and having
triosis on the uterus, ovaries, or fallopian tubes also a high-volume surgeon. Other factors that decreased
increased the risk of conversion. The risk of conver- the risk of conversion included having an alternative
sion was significantly higher with any complication treatment before hysterectomy or a preoperative indi-
including bowel, bladder, ureteral, or vascular injury. cation of pelvic organ prolapse. This model was then
Increasing specimen weight, blood loss, and operative used to estimate predicted means of conversion based
time all were associated with significantly increased on route of surgery and surgeon volume. After arriv-
odds of conversion. ing at a parsimonious model, the C-statistic was 0.85
Patients who underwent concurrent procedures and the Hosmer-Lemeshow test statistic was 8.60 with
such as oophorectomy or hernia repair were not at a P value of .38 for 10 groups. Using this model, the
increased odds of conversion (Table 3). Having con- predicted risk of conversion to laparotomy with tradi-
current bowel surgery (n55) was associated with con- tional laparoscopy compared with robotic-assisted
version in the bivariate analysis. However, on further laparoscopy was 5.4% compared with 0.8% (P,.001)
investigation of these cases, all of these bowel surger- after adjusting for all other variables in the model.
ies appeared to be initiated as a result of an intraoper- High-volume surgeons were less likely to convert to
ative bowel complication. This was reflected in the laparotomy compared with low- and medium-volume
documentation of bowel injury by Current Procedural surgeons with a predicted risk of conversion of 1.4%
Terminology codes. Therefore, this was not included compared with 2.25% (P5.015).
in the model. The high-volume tertile surgeons performed 18–
As shown in Table 4, the significant risk factors 258 hysterectomies captured within the 24-month
for conversion with multivariate logistic regression sample. We identified a significant correlation between
1300 Lim et al Laparoscopic Hysterectomy and Conversion OBSTETRICS & GYNECOLOGY
Copyright ª by The American College of Obstetricians
and Gynecologists. Published by Wolters Kluwer Health, Inc.
Unauthorized reproduction of this article is prohibited.
Table 3. Intraoperative Factors and Risk of Conversion of Laparoscopic Hysterectomy to Laparotomy
Completed Conversion to
Total Laparoscopically Laparotomy Unadjusted OR
Characteristic (N56,992) (n56,717 [96.07]) (n5275 [3.93]) (95% CI) P
Presence of adhesions
None or mild 5,251 (75.10) 5,138 (97.85) 113 (2.15) Referent
Moderate 931 (13.32) 884 (94.95) 47 (5.05) 2.42 (1.71–3.42) ,.001
Severe 810 (11.58) 695 (85.80) 115 (14.20) 7.52 (5.74–9.87) ,.001
Any endometriosis
No 5,877 (84.05) 5,652 (96.17) 225 (3.83) Referent
Yes 1,115 (15.95) 1,065 (95.52) 50 (4.48) 1.18 (0.86–1.61) .302
Endometriosis of uterus, fallopian
tubes, and ovaries
No 6,362 (90.99) 6,124 (91.17) 238 (3.74) Referent
Yes 630 (9.01) 593 (94.13) 37 (5.87) 1.61 (1.12–2.29) .009
Cervical preservation
Supracervical 1,095 (15.66) 1,032 (94.25) 63 (5.75) Referent
Total 5,897 (84.34) 5,685 (96.40) 212 (3.60) 0.61 (0.46–0.82) .001
Concurrent procedures
Oophorectomy
No 4,206 (62.69) 4,054 (96.39) 152 (3.61) Referent
Yes 2,503 (37.31) 2,392 (95.57) 111 (4.43) 1.24 (0.96–1.59) .094
Missing 283 (4.05)
Hernia repair
No 6,955 (99.47) 6,683 (96.09) 272 (3.91) Referent
Yes 37 (0.53) 34 (91.89) 3 (8.11) 2.16 (0.66–7.10) .201
Bowel surgery
No 6,987 (99.93) 6,715 (96.11) 272 (3.89) Referent
Yes 5 (0.07) 2 (40.00) 3 (60.00) 37.03 (6.16–222.53) ,.001
Intraoperative complications
No 6,808 (97.37) 6,572 (96.53) 236 (3.47) Referent
Yes 184 (2.63) 145 (78.80) 39 (21.20) 7.49 (5.14–10.92) ,.001
Bowel complications
No 6,950 (99.40) 6,686 (96.20) 264 (3.80) Referent
Yes 42 (0.60) 31 (73.81) 11 (26.19) 8.99 (4.47–18.07) ,.001
Bladder injury
No 6,941 (99.27) 6,678 (96.21) 263 (3.79) Referent
Yes 51 (0.73) 39 (76.47) 12 (23.53) 7.81 (4.04–15.10) ,.001
Ureteral injury
No 6,978 (99.80) 6,708 (96.13) 270 (3.87) Referent
Yes 14 (0.20) 9 (64.29) 5 (35.71) 13.80 (4.59–41.46) ,.001
Vascular injury
No 6,977 (99.79) 6,707 (96.13) 270 (3.87) Referent
Yes 15 (0.21) 10 (66.67) 5 (33.33) 12.42 (4.22–36.59) ,.001
Pathology
Benign 6,794 (97.20) 6,534 (96.17) 260 (3.83) Referent
Unexpected malignancy 196 (2.80) 181 (92.35) 15 (7.65) 2.08 (1.21–3.58) .008
Missing 2 (0.03)
Specimen weight (g)
Less than 250 5,697 (82.78) 5,535 (97.16) 162 (2.84) Referent
250–499 857 (12.45) 790 (92.18) 67 (7.82) 2.90 (2.16–3.89) ,.001
500–999 268 (3.89) 240 (89.55) 28 (10.45) 3.99 (2.62–6.08) ,.001
1,000 or greater 60 (0.87) 50 (83.33) 10 (16.67) 6.83 (3.40–13.72) ,.001
Missing 110 (1.57)
EBL (mL)
100 or less 4,842 (70.95) 4,800 (99.13) 42 (0.87) Referent
More than 100 to 300 1,479 (21.67) 1,376 (93.04) 103 (6.96) 8.55 (5.95–12.31) ,.001
More than 300 to 500 317 (4.64) 250 (78.86) 67 (21.14) 30.63 (20.40–45.97) ,.001
(continued )
VOL. 128, NO. 6, DECEMBER 2016 Lim et al Laparoscopic Hysterectomy and Conversion 1301
Copyright ª by The American College of Obstetricians
and Gynecologists. Published by Wolters Kluwer Health, Inc.
Unauthorized reproduction of this article is prohibited.
Table 3. Intraoperative Factors and Risk of Conversion of Laparoscopic Hysterectomy to Laparotomy
(continued )
Completed Conversion to
Total Laparoscopically Laparotomy Unadjusted OR
Characteristic (N56,992) (n56,717 [96.07]) (n5275 [3.93]) (95% CI) P
More than 500 to 1,000 147 (2.15) 99 (67.35) 48 (32.65) 55.41 (35.0–87.73) ,.001
Greater than 1,000 40 (0.59) 26 (65.00) 14 (35.00) 61.54 (30.04–126.08) ,.001
Missing 167 (2.39)
Operating room time (min)
120 or less 3,319 (47.48) 3,260 (98.22) 59 (1.78) Referent
More than 120 to 240 3,258 (46.61) 3,085 (94.69) 173 (5.31) 3.10 (2.30–4.18) ,.001
More than 240 to 360 359 (5.14) 325 (90.53) 34 (9.47) 5.78 (3.73–8.95) ,.001
More than 360 54 (0.77) 45 (83.33) 9 (16.67) 11.05 (5.17–23.64) ,.001
Missing 2 (0.03)
OR, odds ratio; CI, confidence interval; EBL, estimated blood loss.
Data are n (%) unless otherwise specified.
use of robotic surgery and surgical volume with a sig- transfusion, postoperative severe sepsis (sepsis with
nificantly greater proportion of high-volume surgeons organ dysfunction), and need for reoperation within
using the robotic platform (72.02%) compared with the 30 days. There was no difference in rates of postop-
low-volume surgeons (49.09%, P,.001). Given some erative organ space surgical site infection, pulmo-
collinearity between the use of the robotic surgical nary embolism or deep vein thrombosis, sepsis, or
platform and high-volume surgeons, we then per- readmission within 30 days. We found that intrao-
formed a subanalysis of high-volume surgeons to perative complications, which may have influenced
examine the effect of robotic use in high-volume sur- the decision to convert to laparotomy, occurred in
geons. Even among high-volume surgeons, the odds of less than 20% of those who had a postoperative com-
conversion was lower with the robotic procedure plication. Therefore, the association between conver-
(7.54% compared with 1.46%, P,.001; adjusted OR sion and postoperative complications was not
0.13, 95% CI 0.06–0.27), even when controlling for entirely related to the prior occurrence of an intra-
other factors including uterine weight and adhesive operative complication.
disease.
To further examine the relationship among high- DISCUSSION
surgeon volume, use of robotic surgery, and the effect In this regional collaborative of 52 hospitals, there was
on conversion, a secondary analysis was conducted a sevenfold reduction in the odds of conversion to
among ultrahigh-volume surgeons. We divided sur- laparotomy with use of robotic-assisted laparoscopy
geon volume into those below the 75th percentile, compared with traditional laparoscopy. The avoid-
75th–89th percentile, 90th–94th percentile, 95th–98th ance of conversion in our cohort of patients had
percentile, and 99th percentile or greater. The num- important clinical repercussions. Patients who had
ber of hysterectomies contributed to the sample in 24 conversion were more likely to experience surgical
months in each group was 1–23, 24–41, 42–60, 61– site infection, blood transfusion, severe sepsis, and
127, and 128–258, respectively. After adjusting for reoperation even when no prior intraoperative com-
patient risk factors, surgical approach (robotic-assisted plication occurred. Similar results were seen in the
laparoscopy compared with traditional laparoscopy), colorectal surgery literature with poorer outcomes in
surgeon volume categories, and significant interaction morbidity, mortality, blood transfusion, and postop-
between approach and volume, we calculated the erative hospital stay.12,13
adjusted predicted risk of conversion with the robotic A wide range of conversion rates for hysterectomy
surgical system compared with traditional laparos- has been reported, ranging from 0% to 19%.3 The
copy (Fig. 2). This demonstrated that there remained 2014 Cochrane Review, which pooled the outcomes
a benefit of use of robotics even among ultrahigh- from four randomized controlled studies, did not find
volume surgeons. a difference in conversion rates of robotic and tradi-
Complications after conversion were examined tional laparoscopies (3.55% compared with 2.98%).
(Table 5), and those who had a conversion had That analysis involved 337 patients with 11 conver-
increased risk of incisional infections, postoperative sions.15 This small sample size may have insufficient
1302 Lim et al Laparoscopic Hysterectomy and Conversion OBSTETRICS & GYNECOLOGY
Copyright ª by The American College of Obstetricians
and Gynecologists. Published by Wolters Kluwer Health, Inc.
Unauthorized reproduction of this article is prohibited.
Table 4. Multivariable Logistic Regression of Risk Factors for Conversion of Laparoscopic Hysterectomy to
Laparotomy*
Characteristic Unadjusted OR (95% CI) P Adjusted OR (95% CI) P
Age (y)
40 or younger Referent Referent
Older than 40 and 60 or younger 1.80 (1.33–2.44) ,.001 1.55 (1.03–2.31) .034
Older than 60 1.41 (0.87–2.31) .165 1.83 (1.00–3.35) .050
Nonwhite vs white 1.85 (1.43–2.40) ,.001 1.07 (0.76–1.52) .694
Surgeon volume
Lower two tertiles Referent Referent
Top tertile 0.46 (0.36–.59) ,.001 0.66 (0.47–0.92) .015
Robotics vs traditional laparoscopy 0.18 (0.13–0.23) ,.001 0.14 (0.07–0.25) ,.001
BMI (kg/m2)
Less than 30 Referent Referent
30 or greater 1.86 (1.45–2.39) ,.001 1.62 (1.24–2.13) ,.001
Alternative treatment before hysterectomy vs none 0.71 (0.56–0.91) .006 0.63 (0.42–0.96) .031
Indications for hysterectomy
Pelvic inflammatory disease
No Referent Referent
Yes 5.28 (1.51–18.48) .009 3.53 (0.75–16.65) .110
Pelvic mass
No Referent Referent
Yes 1.58 (1.06–2.36) .026 1.64 (1.00–2.69) .050
Pelvic organ prolapse
No Referent Referent
Yes 0.35 (0.20–0.61) ,.001 0.40 (0.19–0.83) .015
Adhesions
None or mild Referent Referent
Moderate 2.42 (1.71–3.42) ,.001 2.49 (1.58–3.92) ,.001
Severe 7.52 (5.74–9.87) ,.001 8.07 (5.60–11.62) ,.001
Endometriosis of uterus, fallopian tubes, and ovaries vs none 1.61 (1.12–2.29) .009 1.32 (0.88–1.97) .174
Total vs supracervical hysterectomy 0.61 (0.46–0.82) .001 1.47 (0.92–2.31) .100
Cancer on final pathology vs none 2.08 (1.21–3.58) .008 1.47 (0.76–2.82) .255
Specimen weight (g)
Less than 250 Referent Referent
250–499 2.90 (2.16–3.89) ,.001 2.97 (2.12–4.16) ,.001
500–999 3.99 (2.62–6.08) ,.001 4.88 (2.78–8.58) ,.001
1,000 or greater 6.83 (3.40–13.72) ,.001 5.15 (2.15–12.36) ,.001
OR, odds ratio; CI, confidence interval; BMI, body mass index.
* All covariates listed were included in the multivariable model with accounting for clustering by site using robust standard errors.
power to detect a difference between the approaches. BMI, adhesive disease, and increasing uterine weight
Furthermore, this analysis only included surgeries per- were all found to be associated with increased odds of
formed by 13 high-volume surgeons from four tertiary conversion.3,4,6,20
care centers. In contrast, our analysis involved 6,992 Strengths of this analysis are a large sample of
hysterectomies from a sample of 638 surgeons at com- hysterectomies from a statewide database that in-
munity and tertiary academic hospitals with bed size cludes all payer groups, academic, and community
ranging from less than 100 to greater than 1,000. The hospitals. However, we do not know the indication
larger, diverse sample size in our study may explain for conversion and cannot differentiate between
why we found a difference where authors of the Co- conversions as a result of an adverse, emergent event
chrane Review did not. This lower conversion rate and those without complication and related to
using the robotic surgical system has also been seen surgeon judgment.21 The indication for conversion
in other surgical specialties with decreased rates of has been associated with different risks of complica-
conversion using robotics for prostatectomy and sur- tions and length of hospital stay.3 There is also an
gery for colorectal cancer.13,15–17 Consistent with prior inherent limitation of the sampling methodology,
studies, surgeon volume was found to be associated which captures a random sample of patients at each
with lower odds of conversion,3,18,19 and increasing institution and not every patient for each surgeon.
VOL. 128, NO. 6, DECEMBER 2016 Lim et al Laparoscopic Hysterectomy and Conversion 1303
Copyright ª by The American College of Obstetricians
and Gynecologists. Published by Wolters Kluwer Health, Inc.
Unauthorized reproduction of this article is prohibited.
tice patterns in Michigan may not be applicable to
other geographic regions.
In summary, our study showed that more than
96% of all hysterectomies for benign indications
initiated laparoscopically are completed laparoscopi-
cally. Use of the robotic platform and higher surgeon
volume were both significantly and independently
associated with decreased odds of conversion. Fur-
thermore, conversion to laparotomy is associated with
increased risk of morbidity. Although previous stud-
ies22 including the Cochrane Review have demon-
strated no benefit and higher cost to robotic surgery
compared with traditional laparoscopy, many studies
were limited by smaller samples and single high-
volume institutions and prior cost data do not account
for the potential increased morbidity and cost associ-
Fig. 2. Predicted risk of conversion to laparotomy of ated with conversion.23 Indeed, this study demon-
robotic-assisted laparoscopy compared with traditional
laparoscopy across surgeon volume. strates a potential advantage of robotic surgery in
Lim. Laparoscopic Hysterectomy and Conversion. Obstet Gynecol a generalizable population. Although the relationship
2016. between the use of the robotic surgical platform and
surgeon volume is complex and interrelated, there
appears to be a sustained lower predicted risk of con-
Although our surgeon volume variable likely reflects version in robotic hysterectomy across surgeon vol-
the relative range of surgical experience, surgeon umes, including high-volume surgeons. Future
skill and decision-making cannot be ascertained from research should further examine the association
a surgical database, and this analysis is limited to the among surgical volume, surgical approach, morbidity,
available variables and cases included in the Michi- and cost associated with conversion to laparotomy.
gan Surgical Quality Collaborative database. We Although the findings of this study suggest
were also unable to determine the patient distribu- a significant relationship among the robotic platform,
tion of surgical approach by any given surgeon. Also, high-volume surgeons, and lower odds of conversion
many complications are rare events after hysterec- to laparotomy, these results are not intended to define
tomy and even larger samples may be necessary to medical policies or surgical privileging. Indeed, the
detect a difference in rare outcomes such as venous balance between high-quality surgical care and access
thromboembolism. Lastly, the population and prac- to quality care is complex. Our specialty needs to
Table 5. Thirty-Day Postoperative Outcomes After Conversion of Laparoscopic Hysterectomy to
Laparotomy
Total Completed Laparoscopically Conversion to Open
Outcome (N56,992) (n56,717 [96.07]) (n5275 [3.93]) P
Incisional surgical site infection 48 (0.69) 40 (0.60) 8 (2.91) ,.001
Deep or organ space surgical site 55 (0.79) 53 (0.79) 2 (0.73) 1.000*
infections
Postoperative transfusion 71 (1.02) 47 (0.70) 24 (8.73) ,.001
Postoperative pulmonary 8 (0.11) 8 (0.12) 0 (0) 1.000*
embolism
Postoperative deep vein 5 (0.07) 5 (0.07) 0 (0) 1.000*
thrombosis
Postoperative severe sepsis 5 (0.07) 3 (0.04) 2 (0.73) .014*
Postoperative readmission 209 (3.10) 193 (3.03) 13 (4.81) .098
Need for reoperation 117 (1.74) 107 (1.65) 10 (3.70) .012
Any complication 308 (4.41) 270 (4.02) 38 (13.82) ,.001
Data are n (%) unless otherwise specified.
* Calculated with Fisher exact test owing to low cell size.
1304 Lim et al Laparoscopic Hysterectomy and Conversion OBSTETRICS & GYNECOLOGY
Copyright ª by The American College of Obstetricians
and Gynecologists. Published by Wolters Kluwer Health, Inc.
Unauthorized reproduction of this article is prohibited.
further address the effect of decreased surgical train- 11. Dellinger RP, Levy MM, Rhodes A, Annane D, Gerlach H,
Opal SM, et al. Surviving Sepsis Campaign: international
ing, increased skill required to offer minimally inva- guidelines for management of severe sepsis and septic shock.
sive options to patients with complex pelvic Intensive Care Med 2013;39:165–228.
pathology, and clinical practices with low surgical 12. Marusch F, Gastinger I, Schneider C, Scheidbach H, Konradt J,
volume on quality of care. Bruch HP, et al. Importance of conversion for results obtained
with laparoscopic colorectal surgery. Dis Colon Rectum 2001;
44:207–14.
REFERENCES
13. Tanis PJ, Buskens CJ, Bemelman WA. Laparoscopy for colo-
1. Nieboer TE, Johnson N, Lethaby A, Tavender E, Curr E, Garry R, rectal cancer. Best Pract Res Clin Gastroenterol 2014;28:29–39.
et al. Surgical approach to hysterectomy for benign gynaeco-
logical disease. The Cochrane Database of Systematic Reviews 14. Liu H, Lawrie TA, Lu D, Song H, Wang L, Shi G. Robot-assisted
2009, Issue 3. Art. No.: CD003677. DOI: 10.1002/14651858. surgery in gynaecology. The Cochrane Database of Systematic
CD003677.pub4. Reviews 2014, Issue 12. Art. No.: CD011422. DOI: 10.
1002/14651858.CD011422.
2. Choosing the route of hysterectomy for benign disease. ACOG
Committee Opinion No. 444. American College of Obstetri- 15. Finkelstein J, Eckersberger E, Sadri H, Taneja SS, Lepor H,
cians and Gynecologists. Obstet Gynecol 2009;114:1156–8. Djavan B. Open versus laparoscopic versus robot-assisted lap-
aroscopic prostatectomy: the European and US experience.
3. Twijnstra AR, Blikkendaal MD, van Zwet EW, Jansen FW. Rev Urol 2010;12:35–43.
Clinical relevance of conversion rate and its evaluation in lap-
aroscopic hysterectomy. J Minim Invasive Gynecol 2013;20: 16. Trastulli S, Farinella E, Cirocchi R, Cavaliere D, Avenia N,
64–72. Sciannameo F, et al. Robotic resection compared with lapa-
roscopic rectal resection for cancer: systematic review and
4. Leonard F, Chopin N, Borghese B, Fotso A, Foulot H, Coste J, meta-analysis of short-term outcome. Colorectal Dis 2012;
et al. Total laparoscopic hysterectomy: preoperative risk factors 14:e134–56.
for conversion to laparotomy. J Minim Invasive Gynecol 2005;
12:312–7. 17. Ahlering TE. Robotic versus laparoscopic radical prostatec-
tomy. Nat Clin Pract Urol 2004;1:58–9.
5. Song T, Kim TJ, Kang H, Lee YY, Choi CH, Lee JW, et al.
Factors associated with complications and conversion to lapa- 18. Doll KM, Milad MP, Gossett DR. Surgeon volume and out-
rotomy in women undergoing laparoscopically assisted vaginal comes in benign hysterectomy. J Minim Invasive Gynecol
hysterectomy. Acta Obstet Gynecol Scand 2012;91:620–4. 2013;20:554–61.
6. Park SH, Cho HY, Kim HB. Factors determining conversion to 19. Twijnstra AR, Blikkendaal MD, van Zwet EW, van Kesteren PJ,
laparotomy in patients undergoing total laparoscopic hysterec- de Kroon CD, Jansen FW. Predictors of successful surgical out-
tomy. Gynecol Obstet Invest 2011;71:193–7. come in laparoscopic hysterectomy. Obstet Gynecol 2012;119:
700–8.
7. Wallenstein MR, Ananth CV, Kim JH, Burke WM, Hershman
DL, Lewin SN, et al. Effect of surgical volume on outcomes for 20. Sokol AI, Chuang K, Milad MP. Risk factors for conversion to
laparoscopic hysterectomy for benign indications. Obstet laparotomy during gynecologic laparoscopy. J Am Assoc
Gynecol 2012;119:709–16. Gynecol Laparosc 2003;10:469–73.
8. Wright JD, Lewin SN, Deutsch I, Burke WM, Sun X, Herzog 21. Blikkendaal MD, Twijnstra AR, Stiggelbout AM, Beerlage HP,
TJ. Effect of surgical volume on morbidity and mortality of Bemelman WA, Jansen FW. Achieving consensus on the defi-
abdominal hysterectomy for endometrial cancer. Obstet Gynecol nition of conversion to laparotomy: a Delphi study among gen-
2011;117:1051–9. eral surgeons, gynecologists, and urologists. Surg Endosc 2013;
27:4631–9.
9. Rogo-Gupta LJ, Lewin SN, Kim JH, Burke WM, Sun X,
Herzog TJ, et al. The effect of surgeon volume on outcomes 22. Wright JD, Ananth CV, Lewin SN, Burke WM, Lu YS, Neugut
and resource use for vaginal hysterectomy. Obstet Gynecol AI, et al. Robotically assisted vs laparoscopic hysterectomy
2010;116:1341–7. among women with benign gynecologic disease. JAMA 2013;
309:689–98.
10. Horan TC, Andrus M, Dudeck MA. CDC/NHSN surveillance
definition of health care-associated infection and criteria for 23. Healy MA, Mullard AJ, Campbell DA Jr, Dimick JB. Hospital
specific types of infections in the acute care setting. Am J Infect and payer costs associated with surgical complications. JAMA
Control 2008;36:309–32. Surg 2016 May 11 [Epub ahead of print].
VOL. 128, NO. 6, DECEMBER 2016 Lim et al Laparoscopic Hysterectomy and Conversion 1305
Copyright ª by The American College of Obstetricians
and Gynecologists. Published by Wolters Kluwer Health, Inc.
Unauthorized reproduction of this article is prohibited.
Potrebbero piacerti anche
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- Effect Sugar On ChildrenDocumento5 pagineEffect Sugar On ChildrenIqra AnugerahNessuna valutazione finora
- The Syndromic Management of Vaginal Discharge Using Single-Dose Treatments: A Randomized Controlled Trial in West AfricaDocumento10 pagineThe Syndromic Management of Vaginal Discharge Using Single-Dose Treatments: A Randomized Controlled Trial in West AfricaIqra AnugerahNessuna valutazione finora
- Trichomoniasis and Bacterial Vaginosis in Pregnancy: Inadequately Managed With The Syndromic ApproachDocumento10 pagineTrichomoniasis and Bacterial Vaginosis in Pregnancy: Inadequately Managed With The Syndromic ApproachIqra AnugerahNessuna valutazione finora
- PSP MPC Topic-06Documento13 paginePSP MPC Topic-06Iqra Anugerah100% (1)
- Laparoscopic Removal of Translocated Retroperitoneal IUD: K.K. Roy, N. Banerjee, A. SinhaDocumento3 pagineLaparoscopic Removal of Translocated Retroperitoneal IUD: K.K. Roy, N. Banerjee, A. SinhaIqra AnugerahNessuna valutazione finora
- Brown - 2014 - Endometriosis - An Overview of Cochrane Reviews (Review)Documento44 pagineBrown - 2014 - Endometriosis - An Overview of Cochrane Reviews (Review)Iqra AnugerahNessuna valutazione finora
- Technical Update On Physiology Amniotic FluidDocumento7 pagineTechnical Update On Physiology Amniotic FluidIqra AnugerahNessuna valutazione finora
- Guideline On The Management of Anogenita WartsDocumento9 pagineGuideline On The Management of Anogenita WartsIqra AnugerahNessuna valutazione finora
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (74)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- Admission To HospitalDocumento12 pagineAdmission To HospitalM SulistiawanNessuna valutazione finora
- Electronic PrescribingDocumento5 pagineElectronic PrescribingWally RedsNessuna valutazione finora
- NI Lecture Part IIDocumento40 pagineNI Lecture Part IIFilamae Jayahr Caday100% (1)
- Culture Change in Elder Care (Excerpt)Documento10 pagineCulture Change in Elder Care (Excerpt)Health Professions Press, an imprint of Paul H. Brookes Publishing Co., Inc.Nessuna valutazione finora
- HMODocumento5 pagineHMOdocaisaNessuna valutazione finora
- Walgreens Pharmacy & Physician InfoDocumento2 pagineWalgreens Pharmacy & Physician Infodlgille100% (1)
- Stages For Partial Denture Construction - Student GuideDocumento2 pagineStages For Partial Denture Construction - Student Guidemusy9999Nessuna valutazione finora
- Hidalgo HPSA MemoDocumento4 pagineHidalgo HPSA MemoT.L. LangfordNessuna valutazione finora
- Jennifer Adeli Win Biz ProposalsDocumento3 pagineJennifer Adeli Win Biz Proposalsjma616Nessuna valutazione finora
- Apollo HospitalsDocumento9 pagineApollo HospitalsAnisha SapraNessuna valutazione finora
- Life Safety Code Survey Process (For Hospitals) Design Standards Unit Rules and RegulationsDocumento28 pagineLife Safety Code Survey Process (For Hospitals) Design Standards Unit Rules and RegulationsLaisattrooklai PhisitNessuna valutazione finora
- Payer Enrollment - New Provider Onboarding FormDocumento4 paginePayer Enrollment - New Provider Onboarding Formapi-550911975Nessuna valutazione finora
- CDT 2011 Chapter5Documento45 pagineCDT 2011 Chapter5Asadulla KhanNessuna valutazione finora
- Osei Cassandra CVDocumento2 pagineOsei Cassandra CVCassieOseiNessuna valutazione finora
- NHS CHC Public Information Leaflet FinalDocumento16 pagineNHS CHC Public Information Leaflet FinalSlowfingerNessuna valutazione finora
- 2017 Beyond ABC ReportDocumento102 pagine2017 Beyond ABC ReportKERANewsNessuna valutazione finora
- USACS 2022 Employee Benefits Guide UpdatedDocumento44 pagineUSACS 2022 Employee Benefits Guide UpdatedBen Quigley100% (1)
- BA4 E2 D 01Documento154 pagineBA4 E2 D 01Murtaza OzdemirNessuna valutazione finora
- Periodicity DentalGuideDocumento52 paginePeriodicity DentalGuideSalam BataienehNessuna valutazione finora
- NORTH (Responses) - Form ResponsesDocumento7 pagineNORTH (Responses) - Form ResponsesRichard SonsingNessuna valutazione finora
- Content ServerDocumento9 pagineContent ServerG. Araya MoraNessuna valutazione finora
- BT 2023106Documento2 pagineBT 2023106Indiana Family to FamilyNessuna valutazione finora
- Advanced Care Planning Critical Issue BriefDocumento24 pagineAdvanced Care Planning Critical Issue BriefZekel HealthcareNessuna valutazione finora
- SFGH MapDocumento1 paginaSFGH Mapcloudman81Nessuna valutazione finora
- A Study On Work Life Questionnaire Personal DetailsDocumento3 pagineA Study On Work Life Questionnaire Personal DetailsananthakumarNessuna valutazione finora
- Language For Acute Stroke Online 2016 InitialDocumento2 pagineLanguage For Acute Stroke Online 2016 InitialpcmundotNessuna valutazione finora
- Ethical Dilemmas in The Practice of NursingDocumento15 pagineEthical Dilemmas in The Practice of Nursingestudiant9Nessuna valutazione finora
- Dharma Patel Resume 1Documento1 paginaDharma Patel Resume 1api-474249179Nessuna valutazione finora
- Medicare Claims Processing ManualDocumento206 pagineMedicare Claims Processing ManualRyan Hogan100% (1)
- PRMB PDFDocumento13 paginePRMB PDFkshitijsaxenaNessuna valutazione finora