Potrebbero piacerti anche
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- Vocabulary Bank ActivityDocumento1 paginaVocabulary Bank ActivityTatis MontañezNessuna valutazione finora
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (399)
- Constellations Map Equ ZodiakDocumento1 paginaConstellations Map Equ ZodiakTatis MontañezNessuna valutazione finora
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Ba 2020 PDFDocumento104 pagineBa 2020 PDFTatis MontañezNessuna valutazione finora
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (894)
- Chapter 4 Selected Topics For Circuits and Systems: Poission's Equation: Laplace's EquationDocumento33 pagineChapter 4 Selected Topics For Circuits and Systems: Poission's Equation: Laplace's EquationArial96Nessuna valutazione finora
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- Vocabulary Bank ActivityDocumento1 paginaVocabulary Bank ActivityTatis MontañezNessuna valutazione finora
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- Chapter 9 R17Documento30 pagineChapter 9 R17Tatis MontañezNessuna valutazione finora
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- Ba 2020 PDFDocumento104 pagineBa 2020 PDFTatis MontañezNessuna valutazione finora
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Objetives:: Teacher: Vladimir Andrés Alarcón StudentDocumento7 pagineObjetives:: Teacher: Vladimir Andrés Alarcón StudentTatis MontañezNessuna valutazione finora
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (587)
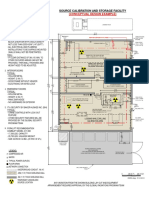
- Source Calibration and Storage FacilityDocumento1 paginaSource Calibration and Storage FacilityTatis MontañezNessuna valutazione finora
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (265)
- 4b Taller NuclearDocumento1 pagina4b Taller NuclearTatis MontañezNessuna valutazione finora
- Capacitance and DielectricsDocumento12 pagineCapacitance and DielectricsTatis MontañezNessuna valutazione finora
- Modern Statistical PhysicsDocumento12 pagineModern Statistical PhysicsVictor De Paula VilaNessuna valutazione finora
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- Redox Biology: Calina Betlazar, Ryan J. Middleton, Richard B. Banati, Guo-Jun LiuDocumento13 pagineRedox Biology: Calina Betlazar, Ryan J. Middleton, Richard B. Banati, Guo-Jun LiuTatis MontañezNessuna valutazione finora
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (73)
- Chapter 9 R17Documento30 pagineChapter 9 R17Tatis MontañezNessuna valutazione finora
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- Jackson E&M Solution Homework 2, #2 .Documento1 paginaJackson E&M Solution Homework 2, #2 .Tikhon Bernstam100% (5)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- ConstantsDocumento1 paginaConstantsTatis MontañezNessuna valutazione finora
- Jackson E&M Solution Homework 2, #2 .Documento1 paginaJackson E&M Solution Homework 2, #2 .Tikhon Bernstam100% (5)
- Lecture on Wave Functions and Uncertainty PrincipleDocumento28 pagineLecture on Wave Functions and Uncertainty PrincipleTatis MontañezNessuna valutazione finora
- Starting Out Strong - Physics WorldDocumento3 pagineStarting Out Strong - Physics WorldFernando ParraNessuna valutazione finora
- Physicists Aim to Classify All Phases of MatterDocumento10 paginePhysicists Aim to Classify All Phases of MatterTatis MontañezNessuna valutazione finora
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- Physicists Aim to Classify All Phases of MatterDocumento10 paginePhysicists Aim to Classify All Phases of MatterTatis MontañezNessuna valutazione finora
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2219)
- S. Rajasekar - Research MethodologyDocumento23 pagineS. Rajasekar - Research MethodologyFebri Priyoyudanto100% (3)
- PHYSICS FOR Diagnostic Radiology PDFDocumento693 paginePHYSICS FOR Diagnostic Radiology PDFTatis Montañez100% (1)
- Vised ManualDocumento113 pagineVised ManualTatis MontañezNessuna valutazione finora
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- Physicists Aim to Classify All Phases of MatterDocumento10 paginePhysicists Aim to Classify All Phases of MatterTatis MontañezNessuna valutazione finora
- Solution To Assignment 5Documento7 pagineSolution To Assignment 5Tatis MontañezNessuna valutazione finora
- S. Rajasekar - Research MethodologyDocumento23 pagineS. Rajasekar - Research MethodologyFebri Priyoyudanto100% (3)
- Campos Electromagneticos, Wangsness.Documento681 pagineCampos Electromagneticos, Wangsness.Itzel Reyna MoralesNessuna valutazione finora
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (119)
- ORA.007 Pharmaceutical Microbiology ManualDocumento92 pagineORA.007 Pharmaceutical Microbiology ManualNindyNessuna valutazione finora
- Mole Airlines, Emp. Form. ExcerciseDocumento2 pagineMole Airlines, Emp. Form. ExcerciseKamariah IsmailNessuna valutazione finora
- Obstetrics Case Proforma TemplateDocumento4 pagineObstetrics Case Proforma TemplateSwapneelShah100% (1)
- ACIDITY REMEDIESDocumento3 pagineACIDITY REMEDIESYasmeen JafferNessuna valutazione finora
- Middle Childhood Physical Development (6-11 YearsDocumento13 pagineMiddle Childhood Physical Development (6-11 YearsAngela YlaganNessuna valutazione finora
- Single/ Exam Zone Centre DetailsDocumento5 pagineSingle/ Exam Zone Centre DetailsHarsh AroraNessuna valutazione finora
- READING ON Tick-Borne DiseasesDocumento3 pagineREADING ON Tick-Borne DiseasesMonique LeonardoNessuna valutazione finora
- Planning and Design of A Cell and Tissue Culture Laboratory: Christopher B. MorrisDocumento2 paginePlanning and Design of A Cell and Tissue Culture Laboratory: Christopher B. MorrisSubaNessuna valutazione finora
- Reflective Essay: Writing in The Genetics DiscourseDocumento5 pagineReflective Essay: Writing in The Genetics DiscourseAnonymous AY6XDZHBxPNessuna valutazione finora
- Paragraph TypesDocumento4 pagineParagraph TypesZayb EhmadNessuna valutazione finora
- Referral Letter: Client Personal Details Client Identity DetailsDocumento2 pagineReferral Letter: Client Personal Details Client Identity DetailsFlorence LinNessuna valutazione finora
- Training Session Evaluation Form InstructionsDocumento8 pagineTraining Session Evaluation Form Instructionsaaronjules100% (1)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- Introduction To Environmental Health LectureDocumento41 pagineIntroduction To Environmental Health LectureJudy OuNessuna valutazione finora
- Safe Food Handlers Course NotesDocumento13 pagineSafe Food Handlers Course NotesJinky PradoNessuna valutazione finora
- FrostbiteDocumento17 pagineFrostbiteIsabel Barredo Del Mundo100% (2)
- Young Schema TheoryDocumento14 pagineYoung Schema TheoryMike F MartelliNessuna valutazione finora
- Education Solutions, Edunsol@gmail - Com, 09996522162Documento170 pagineEducation Solutions, Edunsol@gmail - Com, 09996522162edphrNessuna valutazione finora
- Week 1 Day 1Documento2 pagineWeek 1 Day 1arens100% (1)
- The Ultimate Guide To Anxiety DisordersDocumento66 pagineThe Ultimate Guide To Anxiety Disordersnajaxx100% (2)
- Commissioning Federal Facilities Chiller (PQ)Documento19 pagineCommissioning Federal Facilities Chiller (PQ)Yu-Chih PuNessuna valutazione finora
- Colegiul National SF - Sava Catedra de Limba Engleza Prof. Speteanu Alexandra GabrielaDocumento3 pagineColegiul National SF - Sava Catedra de Limba Engleza Prof. Speteanu Alexandra Gabrielaannem29Nessuna valutazione finora
- Penicillin: Weird RPG Zine Issue 1 F A L L 2 0 1 9Documento16 paginePenicillin: Weird RPG Zine Issue 1 F A L L 2 0 1 9iNessuna valutazione finora
- "Classic" Technique Guide: Niti Rotary Instrumentation SystemDocumento12 pagine"Classic" Technique Guide: Niti Rotary Instrumentation SystemdrnikhilbobadeNessuna valutazione finora
- 2016 3 23 9 12 47tapchi-Dhdn-So12 (97) .2015-Color-WebDocumento128 pagine2016 3 23 9 12 47tapchi-Dhdn-So12 (97) .2015-Color-WebThọ Nguyễn Văn100% (1)
- MRNA Vaccines - Day - 04.14.20 PDFDocumento259 pagineMRNA Vaccines - Day - 04.14.20 PDFTammy G100% (1)
- Annex 2 7d PEMAPS QuestionnaireDocumento5 pagineAnnex 2 7d PEMAPS QuestionnaireAlma PustaNessuna valutazione finora
- Exercise Chart: Warm UpDocumento1 paginaExercise Chart: Warm UpJeremy van der MerweNessuna valutazione finora
- Ingles: Estudiante Harold Andrés Bonett SánchezDocumento8 pagineIngles: Estudiante Harold Andrés Bonett SánchezAndrès BonettNessuna valutazione finora
- Aiapget 2020 QPDocumento29 pagineAiapget 2020 QPGanesh RadhakrishnanNessuna valutazione finora
- By hkdsegayau: 通識科 IES 滿分 Sample (樣本)Documento10 pagineBy hkdsegayau: 通識科 IES 滿分 Sample (樣本)Chi Shing HoNessuna valutazione finora
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionDa EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionValutazione: 4 su 5 stelle4/5 (402)
- Why We Die: The New Science of Aging and the Quest for ImmortalityDa EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityValutazione: 3.5 su 5 stelle3.5/5 (2)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisDa EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisValutazione: 4 su 5 stelle4/5 (1)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedDa EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedValutazione: 5 su 5 stelle5/5 (78)
- The Age of Magical Overthinking: Notes on Modern IrrationalityDa EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityValutazione: 4 su 5 stelle4/5 (13)