Potrebbero piacerti anche
- April 2022 OriginalDocumento348 pagineApril 2022 OriginalEmirhan llkhanNessuna valutazione finora
- Case Presentation and Discussion: Pulmonary TuberculosisDocumento6 pagineCase Presentation and Discussion: Pulmonary TuberculosisCalingalan Hussin CaluangNessuna valutazione finora
- Ward Duty Report Wednesday, 15/02/2017: GP On Duty: Dr. AnanitaDocumento23 pagineWard Duty Report Wednesday, 15/02/2017: GP On Duty: Dr. AnanitaFarella KartikaNessuna valutazione finora
- USMLE 2020 Recall MR MurphyDocumento42 pagineUSMLE 2020 Recall MR MurphyChurschmann Spiral100% (9)
- Pomr ShockDocumento8 paginePomr Shockphyna27Nessuna valutazione finora
- SMLE 2019 EXTRA AUGUST Melody Blue CollectionDocumento82 pagineSMLE 2019 EXTRA AUGUST Melody Blue CollectiondrhirasalmanNessuna valutazione finora
- TB Case Study: Drug-Induced HepatitisDocumento4 pagineTB Case Study: Drug-Induced HepatitisRahmawatifNessuna valutazione finora
- LMS: View Results: No Question Type Weightage Questions Associate Answers Score StatusDocumento5 pagineLMS: View Results: No Question Type Weightage Questions Associate Answers Score StatusRaja SolaimalaiNessuna valutazione finora
- 4 6030444038488853198 PDFDocumento110 pagine4 6030444038488853198 PDFSyeda Seri RazaNessuna valutazione finora
- Syphilis STI (25 May)Documento3 pagineSyphilis STI (25 May)Nicky Wei WeiNessuna valutazione finora
- Guidelines Adult Filipino TB Diagnosis TreatmentDocumento23 pagineGuidelines Adult Filipino TB Diagnosis TreatmentJolaine ValloNessuna valutazione finora
- OSCE Melb11Nov06Documento7 pagineOSCE Melb11Nov06janaka1022Nessuna valutazione finora
- Chapter 3Documento13 pagineChapter 3Stanley AnadiNessuna valutazione finora
- COVID-19 Related Acute Necrotizing Encephalopathy Presenting in The Early Postoperative PeriodDocumento8 pagineCOVID-19 Related Acute Necrotizing Encephalopathy Presenting in The Early Postoperative PeriodElli SymeonidouNessuna valutazione finora
- Article Koskina ArchDocumento8 pagineArticle Koskina ArchElli SymeonidouNessuna valutazione finora
- Hayats ResponsesDocumento18 pagineHayats Responsesyacineone01Nessuna valutazione finora
- Low TSH, low T4, low T3 in the ICU setting is likely centralhypothyroidism. A high TSH would help confirm the diagnosis as centralhypothyroidismDocumento126 pagineLow TSH, low T4, low T3 in the ICU setting is likely centralhypothyroidism. A high TSH would help confirm the diagnosis as centralhypothyroidismmaimoona suleman0% (1)
- Exercise 3 RCTDocumento6 pagineExercise 3 RCTועד מדעי החייםNessuna valutazione finora
- General Medicine Exam Part One ReviewDocumento62 pagineGeneral Medicine Exam Part One ReviewWondimu Koy100% (1)
- A Previously Healthy 3 Year Old Female With Hypertension, Proteinuria, and HypercalciuriaDocumento13 pagineA Previously Healthy 3 Year Old Female With Hypertension, Proteinuria, and Hypercalciuriamenesesgilbertmd333Nessuna valutazione finora
- Marwan PEDocumento12 pagineMarwan PEHalfidaNessuna valutazione finora
- 16 4 2019Documento3 pagine16 4 2019asma .sassi100% (1)
- 2018 April MD Internal Medicine & Geriatrics Selection ExaminationDocumento22 pagine2018 April MD Internal Medicine & Geriatrics Selection ExaminationThanushan BalasingamNessuna valutazione finora
- final exam 2017 ER (sami) ٢Documento17 paginefinal exam 2017 ER (sami) ٢Dr. MLKNessuna valutazione finora
- National ExamDocumento55 pagineNational Examabel100% (1)
- Finalnursing Process ProjectDocumento13 pagineFinalnursing Process Projectapi-531834240Nessuna valutazione finora
- GonartrozaDocumento7 pagineGonartrozaElenaBinzariNessuna valutazione finora
- Updates On COVID 19 (19032020, V1) PDFDocumento32 pagineUpdates On COVID 19 (19032020, V1) PDFroserosannaNessuna valutazione finora
- مذكرة مايوSMLE-2019Documento514 pagineمذكرة مايوSMLE-2019Abidi HichemNessuna valutazione finora
- Choose the Correct Diagnosis from Clinical FindingsDocumento29 pagineChoose the Correct Diagnosis from Clinical Findingsanteneh67% (3)
- 2020 Refresher Course IDSDocumento88 pagine2020 Refresher Course IDSshrwn.y.goNessuna valutazione finora
- Brisbane, 11th October 2008Documento6 pagineBrisbane, 11th October 2008Ywagar YwagarNessuna valutazione finora
- HIV Infectious DiseasesDocumento50 pagineHIV Infectious Diseasesabdul qayyumNessuna valutazione finora
- Prelabor Rupture of Membranes CaseDocumento4 paginePrelabor Rupture of Membranes CaseIan RomanNessuna valutazione finora
- Lauren Herr Nsg-432cc-Care-Plan-ExemplarDocumento11 pagineLauren Herr Nsg-432cc-Care-Plan-Exemplarapi-520453750Nessuna valutazione finora
- C. 48-Year-Old Man Who Has Sex With Men: AlasanDocumento12 pagineC. 48-Year-Old Man Who Has Sex With Men: AlasanAjeng WidyastutiNessuna valutazione finora
- Tetanus Case StudyDocumento4 pagineTetanus Case StudyKervy Jay AgraviadorNessuna valutazione finora
- NCA BurrholeDocumento14 pagineNCA BurrholePhatsee PangilinanNessuna valutazione finora
- Caac 21599Documento8 pagineCaac 21599Kezia TindasNessuna valutazione finora
- نشاط ينايرDocumento23 pagineنشاط ينايرDark AngelNessuna valutazione finora
- Tocilizumab Treatment in COVID 19: A Single Center ExperienceDocumento5 pagineTocilizumab Treatment in COVID 19: A Single Center ExperienceBadiu ElenaNessuna valutazione finora
- MCQDocumento6 pagineMCQalirbidiNessuna valutazione finora
- Pneumonia PedsDocumento13 paginePneumonia PedsRSNessuna valutazione finora
- 病歷首頁 31Documento1 pagina病歷首頁 31waseric09Nessuna valutazione finora
- Neonatal Pneumonia Case StudyDocumento2 pagineNeonatal Pneumonia Case StudyAngel Villamor0% (1)
- Viral EncephalitisDocumento36 pagineViral Encephalitishqayq100% (1)
- Sba 1&2 Conjoint Exam Part II April 2017 Doc-1Documento21 pagineSba 1&2 Conjoint Exam Part II April 2017 Doc-1Fadhly SharimanNessuna valutazione finora
- Community-Acquired Pneumonia Diagnosis and TreatmentDocumento5 pagineCommunity-Acquired Pneumonia Diagnosis and TreatmentJerrica Charlene GalopeNessuna valutazione finora
- Communication Skill inDocumento21 pagineCommunication Skill inNader SugarNessuna valutazione finora
- Mel 2006 Apr 29Documento5 pagineMel 2006 Apr 29ZweNessuna valutazione finora
- DIET 1 Communications Upto 18 2 25Documento6 pagineDIET 1 Communications Upto 18 2 25nathanaellee92Nessuna valutazione finora
- Final Exam Flash Cards - PDocumento37 pagineFinal Exam Flash Cards - PReut shapiraNessuna valutazione finora
- (HOT) AMC MCQ Recalls 2020Documento33 pagine(HOT) AMC MCQ Recalls 2020Gofi100% (1)
- Jointly Team: SMLE GroupDocumento22 pagineJointly Team: SMLE GroupAkpevwe EmefeNessuna valutazione finora
- Ocne 9 SupportDocumento8 pagineOcne 9 Supportapi-349380871Nessuna valutazione finora
- COMPILATION PART 1 - APR 14 New-2Documento38 pagineCOMPILATION PART 1 - APR 14 New-2Rebecca WongNessuna valutazione finora
- BCCA Febrile Neutropenia GuidelinesDocumento2 pagineBCCA Febrile Neutropenia GuidelinesdenokayuMRNessuna valutazione finora
- Case StudyDocumento3 pagineCase StudyAmila RahmahNessuna valutazione finora
- Tuberculosis NclexDocumento3 pagineTuberculosis NclexMarinill SolimanNessuna valutazione finora
- Hope in Cancer Therapy: A holistic approach to cancer with curcumin, b17, insulin, methadone & co.Da EverandHope in Cancer Therapy: A holistic approach to cancer with curcumin, b17, insulin, methadone & co.Nessuna valutazione finora
- ProlanisDocumento1 paginaProlanisRaudha JanahNessuna valutazione finora
- Diabetes ProlanisDocumento11 pagineDiabetes ProlanisRaudha JanahNessuna valutazione finora
- Congenital Band Syndrome Case ReportDocumento5 pagineCongenital Band Syndrome Case ReportRaudha JanahNessuna valutazione finora
- Wolsey SlidesCarnivalDocumento25 pagineWolsey SlidesCarnivalRaudha JanahNessuna valutazione finora
- SoalDocumento19 pagineSoalRaudha JanahNessuna valutazione finora
- Ada, 2007Documento6 pagineAda, 2007shinigamigirl69Nessuna valutazione finora
- Penda Hulu AnDocumento3 paginePenda Hulu AnRaudha JanahNessuna valutazione finora
- Fungal Infection That Cause Brain and Lung DiseaseDocumento9 pagineFungal Infection That Cause Brain and Lung DiseaseRaudha JanahNessuna valutazione finora
- Manson's Tropical Diseases, 21st EditionDocumento2 pagineManson's Tropical Diseases, 21st EditionRaudha JanahNessuna valutazione finora
- CorelDRAW Graphics Suite X7Documento1 paginaCorelDRAW Graphics Suite X7Raudha JanahNessuna valutazione finora
- Guidelines TBC TerbaruDocumento160 pagineGuidelines TBC TerbaruSutoto MoeljadiNessuna valutazione finora
- Genetic RecessiveDocumento3 pagineGenetic Recessivegladz25Nessuna valutazione finora
- 1 Manufacture: A Typical Analysis of Commercial Chlorosulfonic Acid Would Be AsDocumento6 pagine1 Manufacture: A Typical Analysis of Commercial Chlorosulfonic Acid Would Be Asapi-19738746Nessuna valutazione finora
- Clostridium: There Are Four Main Types of ClostridiumDocumento2 pagineClostridium: There Are Four Main Types of ClostridiumHardeeshNessuna valutazione finora
- 05.03 - Interventional Neuroradiology PDFDocumento113 pagine05.03 - Interventional Neuroradiology PDFBivolaru AlinNessuna valutazione finora
- Unit 4 Calling in The Stroke TeamDocumento34 pagineUnit 4 Calling in The Stroke TeamBenazir Margaretha FarhanaNessuna valutazione finora
- Overview and Treatment Option: SkizofreniaDocumento8 pagineOverview and Treatment Option: SkizofreniaEvi LoNessuna valutazione finora
- Killian Middle School: Texas School Survey of Drug and Alcohol Use 2008 Lewisville ISD Campus Level AnalysisDocumento59 pagineKillian Middle School: Texas School Survey of Drug and Alcohol Use 2008 Lewisville ISD Campus Level AnalysisTexas School Survey of Drug and Alcohol UseNessuna valutazione finora
- Biochem-Rebecca NEET Recall 2020 PDFDocumento21 pagineBiochem-Rebecca NEET Recall 2020 PDFNaazneen MohammedNessuna valutazione finora
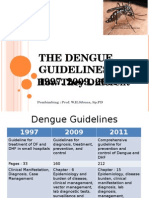
- Guideline Evolution for Diagnosis and Management of DengueDocumento35 pagineGuideline Evolution for Diagnosis and Management of DengueFrinciaNessuna valutazione finora
- The Treatment For Dengue Fever Is Often Supportive in NatureDocumento8 pagineThe Treatment For Dengue Fever Is Often Supportive in NatureJames FabioNessuna valutazione finora
- Interventions With PneumoniaDocumento2 pagineInterventions With PneumoniaAnonymous qemC1CybLNessuna valutazione finora
- 2 ESIC Pharmacist (Employees State Insurance Corporation-Allopathic)Documento10 pagine2 ESIC Pharmacist (Employees State Insurance Corporation-Allopathic)pratyush swarnkar100% (1)
- A Components' Model of Addiction Within A Biopsychosocial FrameworkDocumento8 pagineA Components' Model of Addiction Within A Biopsychosocial FrameworkBognár ErzsébetNessuna valutazione finora
- HSB Pneumonia Antibiotic AlgorithmDocumento4 pagineHSB Pneumonia Antibiotic AlgorithmDr.Senthil KumarNessuna valutazione finora
- URO 14 Carte Program A5Documento12 pagineURO 14 Carte Program A5PápaiZoltánNessuna valutazione finora
- Med J Malaysia Vol 64 No 4 Dec 2009Documento55 pagineMed J Malaysia Vol 64 No 4 Dec 2009Musthafa Afif WardhanaNessuna valutazione finora
- Pulsion Work Booklet: Bucarest Hemodynamic Monitoring WorkshopDocumento43 paginePulsion Work Booklet: Bucarest Hemodynamic Monitoring WorkshopghuoiNessuna valutazione finora
- Facts About The Hand-Off Communications ProjectDocumento2 pagineFacts About The Hand-Off Communications ProjectMukhlish MudaNessuna valutazione finora
- Pulse OximetryDocumento38 paginePulse OximetryJoanna Jauculan Albaño100% (2)
- Pharmaceutical Calculations VIOLET PACOPDocumento41 paginePharmaceutical Calculations VIOLET PACOPSan DarraNessuna valutazione finora
- OmphaloceleDocumento3 pagineOmphaloceleAnonymous uI8yHXobYNessuna valutazione finora
- 3 Heart InternetNewDocumento55 pagine3 Heart InternetNewCoral Srinivasa RamaluNessuna valutazione finora
- RN ScopeofPracticeDocumento86 pagineRN ScopeofPracticeAhmad JamaluddinNessuna valutazione finora
- Dietary Guidelines Allowances For Americans 2010 USDADocumento112 pagineDietary Guidelines Allowances For Americans 2010 USDAkiki_scrabsNessuna valutazione finora
- Science and Health IV 1st Rating45Documento77 pagineScience and Health IV 1st Rating45Juan Alas Ronaldo AziongNessuna valutazione finora
- Bogduk - Pain DefinitionDocumento3 pagineBogduk - Pain DefinitiontapiocadudeNessuna valutazione finora
- Medicine Lecture 1 - History Taking (Colored)Documento4 pagineMedicine Lecture 1 - History Taking (Colored)miguel cuevas100% (2)
- Provision of Higher Education Opportunities for Students of Balochistan & FATADocumento2 pagineProvision of Higher Education Opportunities for Students of Balochistan & FATAAziz okz100% (1)
- Keever FamilyDocumento2 pagineKeever FamilymarylcookpubliclibraNessuna valutazione finora
- Highly Skilled Medical Technologist Seeking New OpportunityDocumento8 pagineHighly Skilled Medical Technologist Seeking New Opportunityrosalyn cabucoNessuna valutazione finora