Documenti di Didattica
Documenti di Professioni
Documenti di Cultura
2 5213442702175109522 PDF
Caricato da
Anonymous tDKku2Titolo originale
Copyright
Formati disponibili
Condividi questo documento
Condividi o incorpora il documento
Hai trovato utile questo documento?
Questo contenuto è inappropriato?
Segnala questo documentoCopyright:
Formati disponibili
2 5213442702175109522 PDF
Caricato da
Anonymous tDKku2Copyright:
Formati disponibili
REvIEWS
pathophysiology, diagnosis and management
of postoperative dumping syndrome
Jan Tack, Joris Arts, Philip Caenepeel, Dominiek De Wulf and Raf Bisschops
abstract | Dumping syndrome is a frequent complication of esophageal, gastric or bariatric surgery.
Rapid gastric emptying, with the delivery to the small intestine of a significant proportion of solid food
as large particles that are difficult to digest, is a key event in the pathogenesis of this syndrome. This
occurrence causes a shift of fluid from the intravascular component to the intestinal lumen, which results in
cardiovascular symptoms, release of several gastrointestinal and pancreatic hormones and late postprandial
hypoglycemia. Early dumping symptoms comprise both gastrointestinal and vasomotor symptoms. Late
dumping symptoms are the result of reactive hypoglycemia. Besides the assessment of clinical alertness and
endoscopic or radiological imaging, a modified oral glucose tolerance test might help to establish a diagnosis.
The first step in treating dumping syndrome is the introduction of dietary measures. Acarbose can be added to
these measures for patients with hypoglycemia, whereas several studies advocate guar gum or pectin to slow
gastric emptying. Somatostatin analogs are the most effective medical therapy for dumping syndrome, and a
slow‑release preparation is the treatment of choice. In patients with treatment‑refractory dumping syndrome,
surgical reintervention or continuous enteral feeding can be considered, but the outcomes of such approaches
are variable.
Tack, J. et al. Nat. Rev. Gastroenterol. Hepatol. 6, 583–590 (2009); published online 1 September 2009; doi:10.1038/nrgastro.2009.148
Introduction
Continuing Medical Education online
the stomach carries out an important role in digestion,
This activity has been planned and implemented in accordance not only through the secretion of hormones and diges-
with the Essential Areas and policies of the Accreditation Council tive enzymes and its mechanical action on ingested food,
for Continuing Medical Education through the joint sponsorship of
MedscapeCME and Nature Publishing Group.
but also by its role in the timed release of ingested nutri-
MedscapeCME is accredited by the Accreditation Council for
ents into the duodenum. the ‘accommodation reflex’
Continuing Medical Education (ACCME) to provide continuing involves a reduction in gastric tone and an increase in
medical education for physicians. gastric compliance in response to food intake, which
MedscapeCME designates this educational activity for a maximum enables an increase in fundic volume without an
of 0.75 aMa pra Category 1 CreditstM. Physicians should only accompanying rise in intragastric pressure.1 this reflex
claim credit commensurate with the extent of their participation
in the activity. All other clinicians completing this activity will
provides a means of temporarily storing ingested food
be issued a certificate of participation. To participate in this before its controlled release into the intestine. Gastric
journal CME activity: (1) review the learning objectives and author accommodation is controlled by a vago–vagal reflex
disclosures; (2) study the education content; (3) take the post‑test pathway that induces activation of inhibitory motor
and/or complete the evaluation at http://cme.medscape.com/
public/naturereviews; and (4) view/print certificate.
neurons in the proximal stomach.2 However, smooth
muscle contractions in the antrum gradually break
learning objectives down large food particles to 1–2 mm fragments, the size
Upon completion of this activity, participants should be able to: at which they can pass through the pylorus into the
1 Describe the main causes of postoperative dumping Department of
syndrome. duodenum. abnormalcies in the coordination of gastric Gastroenterology,
University Hospital
2 Describe differences between early and late dumping in storage and emptying processes lead to impaired food Gasthuisberg, Leuven,
postoperative dumping syndrome. processing and symptoms that are worsened by further Belgium (J. tack,
3 Describe Sigstad’s diagnostic scoring system for dumping
food intake.2,3 J. arts, p. Caenepeel,
syndrome. D. De Wulf,
4 Describe dietary approaches to managing postoperative Dumping syndrome refers to symptoms and signs that r. Bisschops).
dumping syndrome. occur when food reaches the small bowel too rapidly;
Correspondence:
5 Describe treatment approaches to postoperative dumping the condition commonly occurs after partial or total gas- J. Tack, Department of
syndrome.
trectomy, for reasons that are outlined below. Dumping Gastroenterology,
syndrome can also occur after esophageal surgery and, University Hospital
Gasthuisberg,
exceptionally, in the absence of previous surgery. Herestraat 49,
Dumping syndrome was first described by Hertz in B‑3000 Leuven,
Competing interests Belgium
The authors, the Journal Editor N. Wood and the CME questions 1913, who reported the occurrence of ‘dumping-like’ jan.tack@
author D. Lie declare no competing interests. symptoms after gastroenterostomy.4 He reported that med.kuleuven.ac.be
nature reviews | gastroenterology & hepatology volume 6 | oCtoBer 2009 | 583
© 2009 Macmillan Publishers Limited. All rights reserved
REvIEWS
Key points Box 1 | Symptoms of early and late dumping
■ Dumping syndrome is a common complication of esophageal and gastric early dumping
(including bariatric) surgery
Gastrointestinal symptoms
■ Symptoms include early (gastrointestinal and vasomotor) and late
■ Abdominal pain, diarrhea, borborygmi, bloating, nausea
(hypoglycemia) symptoms
■ Diagnosis is based on a suggestive symptom pattern in patients with the vasomotor symptoms
appropriate surgical history; a modified oral glucose tolerance test might help ■ Flushing, palpitations, perspiration, tachycardia,
to establish the diagnosis hypotension, syncope
■ Initial therapy should focus on dietary measures; acarbose can be added to
late dumping
these measures in patients with hypoglycemia
Hypoglycemia
■ In patients who have not responded to initial therapy, (slow‑release)
somatostatin analogs are the treatment of choice Perspiration, palpitations, hunger, weakness, confusion,
■ In patients with treatment‑refractory dumping syndrome, surgical tremor, syncope
reinterventions or continuous enteral feeding can be considered, but the
outcomes of such approaches are variable
hunger, fatigue, confusion, aggression, tremor and
syncope. Both early and late dumping symptoms are
patients felt excessively full after meals, had diar- socially and professionally incapacitating, especially
rhea and needed to lie down because they felt unwell. when syncope occurs.
radiographic examination revealed very rapid empty-
ing of contrast dye from the stomach. rapid emptying Diagnosis
of liquids from the stomach is an important contribu- a suggestive symptom pattern in a patient who has
tor to the pathogenesis of dumping syndrome.5 studies undergone upper abdominal surgery should give cause
conducted in the 1980s demonstrated that a defect in to investigate the possibility of dumping syndrome. in
grinding or sieving within the stomach, which resulted 1970, sigstad proposed a scoring system, based on the
in the delivery of a considerable proportion of solid food occurrence of different symptoms of dumping syn-
as large, less easily digested particles to the small intes- drome, to calculate a diagnostic index (Box 2).12 the
tine (rather than rapid emptying itself), was a key event presence of hypoglycemia concurrently with several
in the pathogenesis of dumping syndrome.5,6 other symptoms is a strong indicator of dumping syn-
Dumping syndrome is now a well-established drome (although the occurrence of insulinoma needs
complication of gastric and esophageal surgery. the to be excluded).
condition has been estimated to occur in up to 20% of a provocative test for assessing dumping syndrome
patients who undergo vagotomy with pyloroplasty and can be used to confirm clinical suspicion. this test is
in up to 50% of patients who undergo esophagectomy.7,8 a modification of the oral glucose tolerance test and
Dumping syndrome has also been reported after nissen involves the ingestion of 50 g or 75 g glucose in solution
fundoplication in children and adults.9,10 in recent years, after an overnight fast. immediately before and up to
bariatric surgery has become the principal cause of 180 min after ingestion of this solution, the blood glucose
postoperative dumping syndrome.11 concentration, hematocrit, pulse rate and blood pressure
with an increasing number of patients undergoing are measured at 30 min intervals. the provocative test is
bariatric surgery, the incidence of dumping syndrome considered positive if late (120–180 min) hypoglycemia
is likely to increase, and clinicians should recognize the occurs, or if an early (30 min) increase in hematocrit of
syndrome and be familiar with its management. in this more than 3% occurs. the best predictor of dumping
review, we summarize the diagnosis, pathophysiological syndrome seems to be a rise in the pulse rate of more
basis and management options for postoperative than 10 bpm after 30 min.13
dumping syndrome. assessments of the speed of gastric emptying might
show that this process occurs rapidly in patients with
Symptoms dumping syndrome—especially for liquid nutrients—but
the symptom profile of patients with dumping syndrome this test does not seem to have good diagnostic sensi-
is summarized in Box 1. symptoms of dumping syn- tivity or specificity, probably because rapid emptying
drome can be classed as early or late, depending on how occurs early after meal ingestion, a phase that is not ana-
soon after ingestion they occur. early symptoms com- lyzed closely or separately in most protocols of gastric
prise both gastrointestinal and vasomotor symptoms. emptying testing.7,13,14
Gastrointestinal symptoms include abdominal pain,
diarrhea, borborygmi, nausea and bloating. vasomotor Pathophysiological mechanisms
symptoms include fatigue, a desire to lie down after the mechanisms that underlie dumping syndrome are
meals, facial flushing, palpitations, perspiration tachy- not completely understood. the symptoms of early and
cardia, hypotension and syncope. late dumping symp- late dumping syndrome are believed to have distinct
toms include hypoglycemia, perspiration, palpitations, underlying pathophysiologies (Figure 1).2,5–7,15
584 | OCTOBER 2009 | vOlumE 6 www.nature.com/nrgastro
© 2009 Macmillan Publishers Limited. All rights reserved
REvIEWS
Box 2 | Sigstad’s scoring system for dumping syndrome20 Agents that increase
Impaired gastric volume
capacity or gastroenterostomy meal viscosity
A total score >7 is suggestive of dumping syndrome, (pectin, guar gum)
whereas a score <4 suggests other diagnoses
■ Shock +5
Octreotide Rapid delivery of nutrients
■ Fainting, syncope, unconsciousness +4 into the duodenum
■ Desire to lie or sit down +4
■ Breathlessness, dyspnea +3
■ Weakness, exhaustion +3 Hyperosmolar contents Rapid absorption
in the duodenum of glucose Acarbose
■ Sleepiness, drowsiness, apathy, falling asleep +3
■ Palpitation +3
■ Restlessness +2 ■ Release of vasoactive agents Hyperinsulinemic response Diazoxide
(neurotensin, VIP)
■ Dizziness +2 ■ Release of incretins
(GIP, GLP-1)
■ Headaches +1 ■ Release of glucose-modulating
hormones (insulin, glucagon) Late dumping
■ Feeling of warmth, sweating, pallor, clammy skin +1 ■ Hypoglycemia
■ Nausea +1
■ Abdominal fullness, meteorism +1
Early dumping
■ Borborygmus +1 ■ Vasomotor symptoms
■ Gastrointestinal symptoms
■ Eructation –1 ■ Hyperglycemia
■ vomiting –4
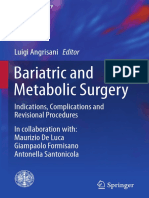
Figure 1 | Pathophysiology of dumping syndrome and mode of action of different
therapeutic agents. The key event in the pathophysiology of dumping syndrome is
the rapid delivery of nutrients into the duodenum. The presence of hyperosmolar
early dumping contents in the duodenum induces the release of a number of vasoactive agents,
after partial gastrectomy, vagotomy and related surger- incretins and glucose modulators, which cause early dumping symptoms. The
ies, gastric volume is reduced. this decreased capacity rapid absorption of glucose induces a hyperinsulinemic response, which leads to
the late dumping symptoms of hypoglycemia. The mode of action of octreotide,
causes the rapid passage of nutrients to the small intes-
diazoxide, viscosity‑increasing agents and acarbose is shown. Abbreviations: GIP,
tine, which induces a cascade of pathophysiological glucose‑dependent insulinotropic polypeptide (also known as gastic inhibitory
events. the arrival of hyperosmolar contents to the polypeptide); GLP‑1, glucagon‑like peptide 1; vIP, vasoactive intestinal peptide.
duodenum causes fluid to move from the intravascular
component to the intestinal lumen.16 this movement
might lead to a decrease in the volume of circulating rapid delivery of carbohydrates to the small intestine in
fluid, tachycardia and, rarely, syncope. the fluid shift into dumping syndrome, therefore, causes excessive insulin
the duodenum might also cause duodenal distention, secretion that subsequently results in hypoglycemia.18
followed by cramp-like contractions. However, whether one of the mediators implicated in this late hypoglycemic
this fluid shift has any role in dumping syndrome or is effect is glucagon-like peptide 1.19
a consequence of it is a matter of controversy, as intra- However, not all cases of postprandial hypoglycemia
venous fluid substitution is unable to prevent early are attributable to dumping syndrome. several patients
dumping symptoms.16 were reported to suffer from hyperinsulinemic hypo-
another important mechanism that contributes to the glycemia with nesidioblastosis after gastric bypass
pathogenesis of early dumping might be the increased surgery; these patients were characterized by severely
release of several gastrointestinal peptide hormones, symptomatic postprandial hypoglycemias and hyper-
such as enteroglucagon, peptide YY, pancreatic poly- insulinemias that did not respond to treatment for
peptide, vasoactive intestinal polypeptide, glucagon- dumping syndrome. these patients were subse-
like peptide 1 and neurotensin, in postoperative dumping quently found to have pancreatic islet cell hyperplasia
syndrome.2,6,15 these hormones’ mode of action might or nesidioblastosis on analysis of resected pancreatic
include changes in gastrointestinal motility and secre- specimens.20,21 Diagnosis of this syndrome, which is
tion, as well as hemodynamic effects—for example, sys- cumbersome, might involve selective stimulation of the
temic hemoconcentration and hypotension occur as a celiac artery by use of calcium as an insulin secretagogue
result of splanchnic vasodilation induced by neurotensin with subsequent sampling of insulin levels from hepatic
or vasoactive intestinal polypeptide.17 venous serum (after insulinoma has been ruled out) as
well as pancreatic debulking and confirmation of islet
late dumping cell hyperplasia on a resected specimen.20,21 Hormonal
late dumping symptoms occur 1–3 h after ingestion changes after roux-en-Y gastric bypass surgery,
of a meal and are attributed to reactive hypoglycemia. including increased release of glucagon-like peptide 1
under ‘normal’ conditions, the presence of glucose in (which increases the mass of β cells in rodents), might
the jejunum is a strong stimulus for insulin secretion; the cause hyperplasia of islet cells. a study has, however,
nature reviews | gastroenterology & hepatology volume 6 | oCtoBer 2009 | 585
© 2009 Macmillan Publishers Limited. All rights reserved
REvIEWS
Suspected dumping pectin and guar gum
increasing the viscosity of food, which slows down gastric
emptying, is another approach to improve dumping
Confirmation by laboratory tests symptoms (table 1) and is achieved by ingesting up
to 15 g of guar gum or pectin with each meal. short-
term studies have shown a potential efficacy of this
Dietary measures for 3–4 weeks approach.26–32 However, the palatability and tolerability
Lack of response of these supplements is poor. moreover, these substances
are usually not readily available as pharmaceutical
Acarbose (in cases of late dumping)
products at sufficiently high doses.
Lack of response
acarbose
Octreotide LAR 20 mg i.m. for 3 months
acarbose is an α-glycosidase hydrolase inhibitor that
Lack of response interferes with carbohydrate absorption in the small intes-
tine. acarbose inhibits the α-glycosidase-mediated pro-
Surgical rescue options?
Continuous nutrition? duction of monosaccharides from carbohydrates in the
epithelial brush border cells of the small intestine. in
Figure 2 | Proposed treatment algorithm for dumping healthy individuals, a 100–200 mg dose of acarbose inhib-
syndrome. This algorithm for the management of patients its the postprandial rise in glycemia, triglycerides and
with dumping syndrome is used at the
insulin. the results from a number of small studies, in
Neurogastroenterology and Motility Clinic of the University
Hospitals in Leuven, Belgium. In case of clinical suspicion, which acarbose was given three times daily at 50–100 mg
we use a modified oral glucose tolerance test to help doses to patients with dumping syndrome, showed an
establish the diagnosis. Our initial therapy is based on improvement in glucose tolerance, a decreased release
dietary measures for 3–4 weeks, plus acarbose treatment of gastrointestinal hormones and a reduction in the inci-
in patients who have hypoglycemia. In patients who fail to dence of hypoglycemia (table 2).33–38 these results were
respond to this initial therapy, slow‑release octreotide is associated with an improvement in dumping symptoms
used. In patients with treatment‑refractory dumping
in these patients.
syndrome, surgical reintervention or continuous enteral
feeding can be considered, but the outcomes of such
this treatment approach, however, affects only the
approaches are variable. Abbreviations: i.m., symptoms of late dumping owing to the mode of action
intramuscular; LAR, long‑acting repeatable. of acarbose (as mentioned above, the production of
monosaccharides in the small intestine is the target
of acarbose). in addition, acarbose treatment often
challenged this theory: the findings showed that the results in bloating, flatulence or diarrhea, as the unab-
β-cell mass in patients with hyperinsulinemic hypo- sorbed carbohydrates undergo bacterial fermentation in
glycemia after gastric bypass surgery was comparable the small intestine; these adverse effects might hamper
to that in Bmi-matched control individuals.22 treatment compliance.
Treatment of dumping syndrome somatostatin analogs
the first step in treating dumping syndrome is the intro- somatostatin and its synthetic analogs have been used
duction of dietary measures. if this approach is insuffi- successfully in the treatment of dumping syndrome
cient, medical therapy and (in some cases) surgery, and have displayed a number of pathophysiologically
might be considered (Figure 2). evidence of the efficacy attractive effects. somatostatin analogs can retard the
of several of these therapies is limited, as most studies gastric emptying rate, retard transit through the small
involve only a few patients and are not controlled. bowel, inhibit the release of gastrointestinal hormones,
inhibit insulin secretion and inhibit postprandial vaso-
Dietary measures dilation. 14,39–50 as such, these analogs show a broad
Dietary measures are the first approach to manage range of activity against the full spectrum of symptoms
dumping syndrome and are probably helpful for the of dumping syndrome. Both short-acting and delayed-
majority of patients.7,11,23–25 Dietary measures include release somatostatin analogs have been used in the treat-
advising patients to consume smaller amounts in one ment of dumping syndrome. short-acting or long-acting
go by dividing the recommended daily energy intake repeatable (lar) formulations of octreotide are the
between six meals. Patients are also advised to delay any agents that have been most commonly studied.14,51–63
liquid intake until at least 30 min after a meal. all rapidly
absorbable carbohydrates (for example, all sweet or Studies of short-acting somatostatin analog octreotide
sweetened foods) should be eliminated from the diet to the results of several short-term studies of subcutane-
prevent late dumping symptoms. lying down for 30 min ously administered octreotide have shown efficacy at
after meals can prolong gastric emptying and help to improving symptoms, improving glycemia and slowing
reduce the symptoms of hypovolemia. gastric emptying (table 3).55–60 However, the need for
586 | OCTOBER 2009 | vOlumE 6 www.nature.com/nrgastro
© 2009 Macmillan Publishers Limited. All rights reserved
REvIEWS
Table 1 | Summary of studies that evaluated pectin and guar gum in dumping syndrome
study no. of treatment results
patients
Jenkins et al. 5 Pectin 14.5 g, single Improved symptoms and glycemia (normalized in 46%
(1977)30 administration before OGTT of patients) during OGTT
Leeds et al. 11 Pectin 15 g, single Improved vasomotor symptoms and glycemia, lower insulin
(1981)31 administration before OGTT levels and prolonged gastric emptying during OGTT
Lawaetz et al. 4 Pectin 15 g, single Reduced vasomotor symptoms, decreased levels of insulin,
(1983)32 administration before OGTT glucagon, neurotensin and GIP and slower initial gastric
emptying during OGTT
Andersen et al. 5 Pectin 5 g, single administration No effect on symptoms or gastric emptying rate
(1989)29 before muffin meal
Harju et al. (1983)26 11 Guar gum 5 g with meals Improvement of symptoms
Harju et al. (1984) 27
11 Guar gum 5 g with meals Slowing of gastric emptying
Harju et al. (1987)28 11 Guar gum 5 g with a glucose Improvement of symptoms and hyperglycemia after
challenge meal a glucose challenge meal
Abbreviations: GIP, glucose‑dependent insulinotropic polypeptide (also known as gastic inhibitory polypeptide); OGTT, oral glucose tolerance test.
Table 2 | Summary of studies that evaluated acarbose in dumping syndrome
study no. of treatment result
patients
McLoughlin et al. 10 Acarbose 100 mg single Improved symptoms and glycemia during OGTT; reduced rise
(1979)36 administration before OGTT in plasma levels of GIP and insulin; no change in gastric
emptying rate
Gerard et al. 24 Acarbose 100 mg single Improved glycemia during OGTT; reduced rise in plasma levels
(1983)35 administration before OGTT of insulin; inhibition of glucose‑induced glucagon suppression
Lyons et al. 13 Acarbose 50 mg single Significant attenuation of hyperglycemia; reduced rise in
(1985)33 administration before standard plasma levels of GIP, enteroglucagon and insulin; no influence
breakfast on plasma levels of vIP and somatostatin; no significant
effect on symptoms
Hasegawa et al. 6 Acarbose 50–100 mg three Attenuation of glucose fluctuations and improvement
(1998)34 times daily before meals for of dumping symptoms (uncontrolled)
a month
Abbreviations: GIP, glucose‑dependent insulinotropic polypeptide (also known as gastic inhibitory polypeptide); OGTT, oral glucose tolerance test; vIP, vasoactive
intestinal peptide.
3–4 daily injections is potentially a major limitation for continued octreotide therapy after the follow-up period
the long-term application of short-acting somatostatin of 93 ± 15 months.62
analogs. three studies have evaluated the long-term use
of subcutaneously administered octreotide in the treat- Studies of long-acting octreotide LAR
ment of dumping syndrome. Geer et al. found that long- slow-release preparations of somatostatin analogs, which
term octreotide therapy (15 months on average) provided require only monthly intramuscular injections, are an
sustained symptom control. 57 of 10 patients, eight attractive alternative to multiple daily injections of the
received three daily injections of 100 μg octreotide, which short-acting formulations. two studies have investigated
resulted in good symptom control; seven indivi duals the efficacy of a slow-release preparation of octreotide
were able to resume work. similarly, vecht et al. evalu- in dumping syndrome. Penning et al. compared the
ated the long-term effect of three daily doses of 25–200 μg efficacy of monthly octreotide lar (10 mg) to sub-
octreotide in 20 patients with a mean follow-up of cutaneous octreotide and found both formulations to be
37 months.61 all patients had an initial positive response; effective at improving symptoms.63 the long-acting form
at 3 months, 80% continued this positive response. after seemed superior at increasing body weight and improv-
10 years, however, 11 of the 20 patients had stopped ing quality of life. the 10 mg dose is only available in a
therapy for a variety of reasons, including lack of effect limited number of countries; the 20 mg dose is the usual
at 3 months (n = 4), diarrhea (n = 4), painful injec- standard dose for octreotide lar.
tions (n = 1), reversible alopecia (n = 1) and weight loss a multicenter study in Belgium confirmed the efficacy
(n = 1). similar data were obtained in a larger group of of monthly octreotide lar (20 mg) in the treatment of
patients, in whom long-term effects seemed less favor- dumping syndrome that was refractory to dietary mea-
able than short-term effects, although 41% of the cohort sures and acarbose treatment.14 the study compared the
nature reviews | gastroenterology & hepatology volume 6 | oCtoBer 2009 | 587
© 2009 Macmillan Publishers Limited. All rights reserved
REvIEWS
Table 3 | Summary of studies that evaluated octreotide in dumping syndrome
study no. of treatment result
patients
Hopman et al. 12 Octreotide 50 μg vs Improved dumping symptoms and suppression of postprandial
(1988)51 placebo before OGTT rise in pulse rate; reduced peak insulin and increased nadir
glycemia; slowing of gastrointestinal transit
Primrose & Johnston 10 Octreotide 50 μg vs 100 μg Reduced early dumping and abolished late dumping symptoms;
(1989)52 vs placebo before OGTT suppression of early dumping‑associated changes in hematocrit
and pulse rate; inhibition of hypoglycemia
Tulassay et al. 8 Octreotide 50 μg vs Suppression of rise in pulse rate and hematocrit; suppression
(1989)56 placebo before OGTT of rise in plasma levels of vIP; inhibition of postprandial
hypoglycemia; inhibition of rise in plasma levels of insulin and GIP
Geer et al. (1990)57 10 Octreotide 100 μg vs Prevention of development of dumping symptoms and diarrhea;
placebo before a dumping prevention of late hypoglycemia and of the rise in plasma levels
provocative meal of glucose, glucagon, pancreatic polypeptide, neurotensin and
insulin; delayed gastric emptying and intestinal transit
Richards et al. 6 Octreotide 100 μg vs Prevention of dumping symptoms; induction of migrating motor
(1990)58 placebo before a dumping complex phase III in the small intestine; decreased postprandial
provocative meal intestinal motor activity
Gray et al. (1991)59 9 Octreotide 100 μg vs Suppression of rise in pulse rate; inhibition of insulin release;
placebo before a dumping prevention of hypoglycemia; inhibition of dumping symptoms
provocative meal
Hasler et al. 8 Octreotide 50 μg vs Suppression of rise in pulse rate; inhibition of dumping symptoms
(1996)60 placebo before OGTT and diarrhea; no influence on change in hematocrit; inhibition
of insulin release; prevention of hypoglycemia; no influence on
gastric emptying rate
Arts et al. (2009)14 30 Octreotide 50 μg before Suppression of rise in pulse rate and hematocrit; inhibition of
OGTT postprandial hypoglycemia; inhibition of rise in plasma levels
of insulin; improvement of early and late dumping symptoms
Abbreviations: GIP, glucose‑dependent insulinotropic polypeptide (also known as gastic inhibitory polypeptide); OGTT, oral glucose tolerance test; vIP, vasoactive
intestinal peptide.
control of symptoms and underlying pathophysiological with dumping syndrome. However, dumping syndrome
mechanisms after 3 days of subcutaneous treatment with is associated with major impairment of quality of life, and
octreotide (50 μg, 3 times daily) with 3 months of treat- the improvement in this parameter with somatostatin
ment with octreotide lar at 20 mg. Both the short-acting analogs is impressive.14,57
and the long-acting formulations had a favorable effect on
dumping symptoms, glycemia and pulse rate during provo- Diazoxide
cative testing for dumping. the short-acting form showed Diazoxide is a potassium channel activator that hyper-
greater efficacy than the long-acting form at improving polarizes cells, including β cells, and, therefore, inhib-
hypoglycemia. However, treatment with the long-acting its voltage-sensitive calcium channels. the drug has
formulation was associated with a significant improve- been used clinically in the treatment of hypertension
ment in patients’ quality of life and was markedly preferred and insulinoma, as it inhibits calcium-induced insulin
by recipients over the short-acting preparation.14 release. the use of diazoxide administered three times
daily at 100–150 mg for late dumping symptoms has been
Adverse effects of somatostatin analogs anecdotally reported,21 but no effect on the early symp-
the main adverse events related to the use of somato- toms of dumping syndrome is expected with diazoxide
statin analogs are pain at the site of injection, gallstone treatment owing to its mode of action.
formation and the occurrence of steatorrhea. the latter
symptom is usually mild, and the long-term use of somato- rescue therapies
statin analogs is usually associated with a weight gain of in spite of some successful therapeutic options, a number
approximately 1% in spite of the occurrence of steatorrhea. of patients continue to have treatment-refractory dumping
Gallstone formation is not an uncommon complication of symptoms. in these difficult cases, surgical interventions
the long-term use of somatostatin analogs and should be or continuous enteral feeding can be considered.
taken into account when considering treatment options for
dumping syndrome.64,65 another disadvantage of somato- Surgery
statin analogs is their considerable cost. For this and the Depending on the previous type of gastric surgery, several
aforementioned reasons, treatment with somatostatin types of reintervention have been proposed, including
analogs is not the first-line treatment option for patients narrowing of the anastomosis, conversion of Bilroth
588 | OCTOBER 2009 | vOlumE 6 www.nature.com/nrgastro
© 2009 Macmillan Publishers Limited. All rights reserved
REvIEWS
type ii to Bilroth type i gastroenterostomy, conversion to more prevalent with increasing rates of bariatric surgery.
a roux-en-Y construction, reconstruction of the pylorus a diagnosis is made on the basis of clinical suspicion in
or interposition of a 10 cm antiperistaltic jejunal loop.66–71 case of suggestive symptoms, aided by a modified oral
the results from case series support the conversion of glucose tolerance test. initial therapy should focus on
Bilroth type ii to Bilroth type i gastroenterostomy in the dietary measures for 3–4 weeks. if insufficient improve-
treatment of dumping syndrome.66 ment occurs, acarbose can also be administered to
in patients who develop the syndrome after vagotomy patients with predominant late dumping symptoms.
with pyloroplasty, surgical reconstruction of the pylorus somatostatin analogs are the next approach to consider
improves symptoms and decreases the gastric emptying in patients with well-established dumping syndrome
rate.66,68,69 the reversal of rapid initial gastric emptying has who have failed to respond to initial therapy and whose
been implicated in the therapeutic effect of pyloric quality of life is substantially affected by their symptoms;
reconstruction.69 in addition, roux-en-Y reconstruc- the approach of choice is treatment with slow-release
tion has a favorable effect on dumping symptoms after formulations because of their ease of administration and
partial gastrectomy and results in retardation of gastric superior effect on quality of life. after an initial 3-month
emptying.70 Concomitant vagotomy improves the thera- treatment with somatostatin analogs, long-term therapy
peutic outcome of roux-en-Y reconstruction.71 Jejunal should be continued only if a substantial improvement
interposition of an antiperistaltic loop is superior to an in symptoms is seen. whether increasing the dose
isoperistaltic (Henley) loop in the management of refrac- (for example, of octreotide lar from 20 mg to 30 mg)
tory dumping.66,67,72 However, our own experience sug- improves symptom control in dumping syndrome is cur-
gests that the outcomes of these interventions are often rently unclear, but our personal experience would argue
unpredictable in clinical practice. against dose increments in patients who fail to respond.
in these patients, surgery or continuous enteral feeding
Continuous enteral feeding might be necessary, but the outcome of these approaches
a final approach to treatment of patients with refractory is variable.
dumping syndrome is the creation of a feeding jejuno-
stomy, through which a continuous background flow of
nutrients can be provided. this is a rather invasive inter- Review criteria
vention, with a major effect on daily life, but it seems to be To identify relevant studies, the MEDLINE database was
effective at avoiding the symptoms of the syndrome that are searched. Medical subject headings and free‑text terms
triggered by meal ingestion (on the basis of one published for (postoperative) dumping were combined with the
case report and on our own, unpublished, experience).73 terms “pathophysiology”, “symptoms”, “management”,
“diet”, “pectin”, “guar gum”, “acarbose”, “diazoxide”,
“somatostatin analog”, “octreotide”, “somatulin” and
Conclusions
“surgery”. The reference lists from retrieved articles were
Dumping syndrome is a well-established complication
also examined for relevant papers.
of upper gastrointestinal surgery and is likely to become
1. Kindt, S. & Tack, J. Impaired gastric 9. Pimpalwar, A. & Najmaldin, A. Results of 16. Johnson, L. P., Sloop, R. D. & Jesseph, R. E.
accommodation and its role in dyspepsia. Gut laparoscopic antireflux procedures in Etiologic significance of the early symptomatic
55, 1685–1691 (2006). neurologically impaired children. Semin. phase in the dumping syndrome. Ann. Surg.
2. Tack, J. Gastric motor disorders. Best Pract. Res. Laparosc. Surg. 9, 190–196 (2002). 156, 173–179 (1962).
Clin. Gastroenterol. 21, 633–644 (2007). 10. Zaloga, G. P. & Chernow, B. Postprandial 17. Sirinek, K. R., O’Dorisio, T. M., Howe, B. &
3. Bisschops, R. et al. Relationship between hypoglycemia after Nissen fundoplication for McFee, A. S. Neurotensin, vasoactive
symptoms and ingestion of a meal in functional reflux esopahgitis. Gastroenterology 84, intestinal peptide, and Roux‑en‑Y
dyspepsia. Gut 57, 1495–1503 (2008). 840–842 (1983). gastrojejunostomy: their role in the dumping
4. Hertz, A. F. The cause and treatment of certain 11. Abell, T. L. & Minocha, A. Gastrointestinal syndrome. Arch. Surg. 120, 605–609 (1985).
unfavorable after‑effects of gastro‑enterostomy. complications of bariatric surgery: 18. Eloy, R., Garaud, J. C., Moody, A., Jaeck, D. &
Proc. R. Soc. Med. 6, 155–163 (1913). diagnosis and therapy. Am. J. Med. Sci. 331, Grenier, J. F. Jejunal factor stimulating insulin
5. MacGregor, I., Parent, J. & Meyer, J. H. Gastric 214–218 (2006). release in the isolated perfused canine
emptying of liquid meals and pancreatic and 12. Sigstad, H. A clinical diagnostic index in the pancreas and jejunum. Horm. Metab. Res. 7,
biliary secretion after subtotal gastrectomy or diagnosis of the dumping syndrome. Changes in 461–467 (1975).
truncal vagotomy and pyloroplasty in man. plasma volume and blood sugar after a test 19. Toft‑Nielsen, M., Madsbad, S. & Holst, J. J.
Gastroenterology 72, 195–205 (1977). meal. Acta Med. Scand. 188, 479–486 (1970). Exaggerated secretion of glucagon‑like
6. Mayer, E. A. et al. Gastric emptying and sieving of 13. van der Kleij, F. G., vecht, J., Lamers, C. B. & peptide‑1 could cause reactive hypoglycemia.
solid food and pancreatic and biliary secretion Masclee, A. A. Diagnostic value of dumping Diabetologia 41, 1180–1186 (1998).
after solid meals in patients with truncal provocation in patients after gastric surgery. 20. Service, G. J. et al. Hyperinsulinemic
vagotomy and antrectomy. Gastroenterology 83, Scand. J. Gastroenterol. 31, 1162–1166 (1996). hypoglycemia with nesidioblastosis after
184–192 (1982). 14. Arts, J. et al. Efficacy of the long‑acting gastric‑bypass surgery. N. Engl. J. Med. 353,
7. vecht, J., Masclee, A. & Lamers, C. The dumping repeatable formulation of the somatostatin 249–254 (2005).
syndrome. Current insights into pathophysiology, analog octreotide in postoperative dumping. 21. Patti, M. E. et al. Severe hypoglycemia post‑
diagnosis and treatment. Scand. J. Gastroenterol. Clin. Gastroenterol. Hepatol. 7, 432–437 (2009). gastric bypass requiring partial
223, 21–27 (1997). 15. Lawaetz, O. et al. Gut hormone profile and pncreatectomy: evidence for inappropriate
8. McLarty, A. et al. Esophageal resection for cancer gastric emptying in the dumping syndrome. insulin secretion and pancreatic islet
of the esophagus: long‑term function and quality A hypothesis concerning the pathogenesis. hyperplasia. Diabetologia 48, 2236–2240
of life. Ann. Thorac. Surg. 63, 1568–1572 (1997). Scand. J. Gastoenterol. 18, 73–80 (1983). (2005).
nature reviews | gastroenterology & hepatology volume 6 | oCtoBer 2009 | 589
© 2009 Macmillan Publishers Limited. All rights reserved
REvIEWS
22. Meier, J. J., Butler, A. E., Galasso, R. & Butler, P. C. (SMS 201–995) on postprandial gastric 57. Geer, R. J. et al. Efficacy of octreotide acetate in
Hyperinsulinemic hypoglycemia after gastric emptying of 99mTc–tin colloid and treatment of severe postgastrectomy dumping
bypass surgery is not accompanied by islet mouth‑to‑caecum transit time in man. Digestion syndrome. Ann. Surg. 212, 678–687 (1990).
hyperplasia or increased beta‑cell turnover. 36, 101–107 (1987). 58. Richards, W. O. et al. Octreotide acetate induces
Diabetes Care 49, 1554–1559 (2006). 41. van Berge Henegouwen, M. I., van Gulik, T. M., fasting small bowel motility in patients with
23. Robinson, F. W. & Pittman, A. C. Dietary Akkermans, L. M., Jansen, J. B. & Gouma, D. J. dumping syndrome. J. Surg. Res. 49, 483–487
management of postgastrectomy dumping The effect of octreotide on gastric emptying at a (1990).
syndrome. Surg. Gynecol. Obstet. 104, 529–534 dosage used to prevent complications after 59. Gray, J. L., Debas, H. T. & Mulvihill, S. J. Control
(1957). pancreatic surgery: a randomised, placebo of dumping symptoms by somatostatin analog in
24. Pittman, A. C. & Robinson, F. W. Dietary controlled study in volunteers. Gut 41, 758–762 patients after gastric surgery. Arch. Surg. 126,
management of the “dumping” syndrome: (1997). 1231–1235 (1991).
long‑term follow‑up. J. Am. Diet. Assoc. 40, 42. Foxx‑Orenstein, A., Camilleri, M., Stephens, D. & 60. Hasler, W. L., Soudah, H. C. & Owyang, C.
108–110 (1962). Burton, D. Effect of a somatostatin analog on Mechanisms by which octreotide ameliorates
25. Khoshoo, v., Reifen, R. M., Gold, B. D., gastric motor and sensory functions in healthy symptoms in the dumping syndrome.
Sherman, P. M. & Pencharz, P. B. Nutritional humans. Gut 52, 1555–1561 (2003). J. Pharmacol. Exp. Ther. 277, 1359–1365 (1996).
manipulation in the management of dumping 43. Di Lorenzo, C., Lucanto, C., Flores, A., Idries, S. & 61. vecht, J., Lamers, C. & Masclee, A. Long‑term
syndrome. Arch. Dis. Child 66, 1447–1448 Hyman, P. Effect of sequential erythromycin and results of octreotide‑therapy in severe dumping
(1991). octreotide on antroduodenal manometry. syndrome. Clin. Endocrinol. (Oxf.) 51, 619–624
26. Harju, E. & Larmi, T. K. Efficacy of guar gum in J. Pediatr. Gastroenterol. Nutr. 29, 293–296 (1999).
preventing the dumping syndrome. JPEN 7, (1999). 62. Didden, P., Penning, C. & Masclee, A. A.
470–472 (1983). 44. Nelson‑Piercy, C. et al. Effect of a new oral Octreotide therapy in dumping syndrome:
27. Harju, E., Heikkila, J. & Larmi, T. K. Effect of guar somatostatin analog (SDZCO611) on gastric analysis of long‑term results. Aliment. Pharmacol.
gum on gastric emptying after gastric resection. emptying, mouth to cecum transit time, and Ther. 24, 1367–1375 (2006).
JPEN 8, 18–20 (1984). pancreatic and gut hormone release in normal 63. Penning, C., vecht, J. & Masclee, A. Efficacy of
28. Harju, E. & Makela, J. Reduction in symptoms male subjects. J. Clin. Endocrinol. Metab. 78, depot long‑acting release octreotide therapy in
after proximal selective vagotomy through 329–336 (1994). severe dumping syndrome. Aliment. Pharmacol.
increased dietary viscosity. Am. J. Gastroenterol. 45. von der Ohe, M., Camilleri, M., Thomforde, G. & Ther. 22, 963–969 (2005).
79, 861–863 (1984). Klee, G. Differential regional effects of octreotide 64. Ewins, D. L. et al. Assessment of gall bladder
29. Andersen, J. R., Holtug, K. & Uhrenholt, A. Trial of on human gastrointestinal motor function. Gut dynamics, cholecystokinin release and the
pectin‑enriched muffins in patients with severe 36, 743–748 (1995). development of gallstones during octreotide
dumping syndrome after gastric resection: 46. Kreanzlin, M. et al. Effect of long‑acting therapy for acromegaly. Q. J. Med. 83, 295–306
observations on symptoms and gastric emptying somatostatin analog SMS 201–995 on gut (1992).
pattern. Acta Chir. Scand. 155, 39–41 (1989). hormone secretion in normal subjects. Experintia 65. Moschetta, A. et al. Severe impairment of
30. Jenkins, D. J. et al. Effect of dietary fiber on 41, 738–740 (1985). postprandial cholecystokinin release and gall‑
complications of gastric surgery: prevention of 47. Williams, G. et al. Postprandial effects of SMS bladder emptying and high risk of gallstone
postprandial hypoglycemia by pectin. 201–995 on gut hormones and glucose formation in acromegalic patients during
Gastroenterology 73, 215–217 (1977). tolerance. Scand. J. Gastroenterol. Sandostatin LAR. Aliment. Pharmacol. Ther. 15,
31. Leeds, A. R., Ralphs, D. N., Ebied, F., Metz, G. & 21 (suppl. 119), 73–83 (1986). 181–185 (2001).
Dilawari, J. B. Pectin in the dumping syndrome: 48. Parkinson, C. et al. A comparison of the effects of 66. Woodward, E. R., Deser, P. L. & Gasster, M.
reduction of symptoms and plasma volume pegvisomant and octreotide on glucose, insulin, Surgical treatment of the postgastrectomy
changes. Lancet 1, 1075–1078 (1981). gastrin, cholecystokinin, and pancreatic dumping syndrome. West. J. Surg. Obstet.
32. Lawaetz, O., Blackburn, A. M., Bloom, S. R., polypeptide responses to oral glucose and a Gynecol. 63, 567–573 (1955).
Aritas, Y. & Raplhs, D. N. Effect of pectin on standard mixed meal. J. Clin. Endocrinol. Metab. 67. Sawyers, J. L. & Herrington, J. L. Superiority of
gastric emptying and gut hormone release in the 87, 1797–1804 (2002). antipersitaltic jejunal segments in management
dumping syndrome. Scand. J. Gastroenterol. 18, 49. Kemmer, T. P. et al. Inhibition of human exocrine of severe dumping syndrome. Ann. Surg. 178,
327–336 (1983). pancreatic secretion by the long‑acting 311–321 (1973).
33. Lyons, T. J., McLoughlin, J. C., Shaw, C. & somatostatin analog octreotide (SMS201–995). 68. Koruth, N. M., Krukowski, Z. H. &
Buchanan, K. D. Effect of acarbose on Aliment. Pharmacol. Ther. 6, 41–50 (1992). Matheson, N. A. Pyloric reconstruction. Br. J.
biochemical responses and clinical symptoms in 50. Högenauer, C., Aichbichler, B., Santa Ana, C., Surg. 72, 808–810 (1985).
dumping syndrome. Digestion 31, 89–96 (1985). Porter, J. & Fordtran, J. Effect of octreotide on 69. Cheadle, W. G., Baker, P. R. & Cuschieri, A. Pyloric
34. Hasegawa, T. et al. Long‑term effect of fluid absorption and secretion by the normal reconstruction for severe vasomotor dumping
α‑glycosidase inhibitor on late dumping human jejunum and ileum in vivo. Aliment. after vagotomy and pylorpoplasty. Ann. Surg. 202,
syndrome. J. Gastroenterol. Hepatol. 13, Pharmacol. Ther. 16, 769–777 (2002). 568–572 (1985).
1201–1206 (1998). 51. Hopman, W., Wolberink, R., Lamers, C. & 70. vogel, S., Hocking, M. & Woodward, E. Clinical
35. Gerard, J., Luyckx, A. S. & Lefebvre, P. J. Acarbose van Tongeren, J. Treatment of the dumping and radionuclide evaluation of Roux‑Y diversion
in reactive hypoglycemia: a double‑blind study. Int. syndrome with the somatostatin analog for postgastrectomy dumping. Am. J. Surg. 155,
J. Clin. Pharmacol. Ther. Toxicol. 22, 25–31 (1983). SMS201–995. Ann. Surg. 207, 155–159 (1988). 57–62 (1988).
36. McLoughlin, J. C., Buchanan, K. D. & Alam, M. J. 52. Primrose, J. N. & Johnston, D. Somatostatin 71. Hocking, M. P., vogel, S. B., Falasca, C. A. &
α‑Glycoside‑hydrolase inhibitor in treatment of analog SMS 201–995 (octreotide) as a possible Woodward, E. R. Delayed gastric emptying of
dumping syndrome. Lancet 2, 603–605 (1979). solution to the dumping syndrome after liquids and solids following Roux‑en‑Y biliary
37. Ng, D. D. et al. Acarbose treatment of gastrectomy or vagotomy. Br. J. Surg. 76, diversion. Ann. Surg. 194, 494–501 (1981).
postprandial hypglycemia in children after Nissen 140–144 (1989). 72. Ramus, N., Williamson, R. & Jonhston, D. The
fundoplication. J. Pediatr. 139, 877–879 (2001). 53. Morz, R., Prager, J. & Pointer, H. Influence of use of jejunal interposition for intractable
38. Moreira, R. O., Moreira, R. B., Machado, N. A., somatostatin (SS‑14) on early dumping reaction symptoms complicating peptic ulcer surgery. Br.
Goncalves, T. B. & Coutinho, W. F. Postprandial in patients after partial gastrectomy [German]. J. Surg. 69, 265–268 (1982).
hypoglycemia after bariatric surgery Z. Gastroenterol. 20, 299–304 (1982). 73. veit, F., Heine, R. G. & Catto‑Smith, A. G.
pharmacological treatment with verapamil and 54. Long, R., Adrian, T. & Bloom, S. Somatostatin Dumping syndrome after Nissen fundoplication.
acarbose. Obes. Surg. 18, 1618–1621 (2008). and the dumping syndrome. Br. Med. J. (Clin. Res.) J. Pediatr. Child Health 30, 182–185 (1994).
39. Edmunds, M., Chen, J., Soykan, I., Lin, Z. & 290, 886–888 (1985).
McCallum, W. Effect of octreotide on gastric and 55. Reasbeck, P. & van Rij, A. The effect of acknowledgments
small bowel motility in patients with somatostatin on dumping after gastric surgery: a Désirée Lie, University of California, Irvine, CA, is the
gastroparesis. Aliment. Pharmacol. Ther. 12, preliminary report. Surgery 99, 462–468 (1986). author of and is solely responsible for the content of
167–174 (1998). 56. Tulassay, Z., Tulassay, T., Gupta, R. & Cierny, G. the learning objectives, questions and answers of the
40. Fuessl, H., Carolan, G., Williams, G. & Bloom, S. Long acting somatostatin analog in dumping MedscapeCME‑accredited continuing medical
Effect of a long‑acting somatostatin analog syndrome. Br. J. Surg. 76, 1294–1295 (1989). education activity associated with this article.
590 | OCTOBER 2009 | vOlumE 6 www.nature.com/nrgastro
© 2009 Macmillan Publishers Limited. All rights reserved
Potrebbero piacerti anche
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- Megan Moore, RD - The Complete Bariatric Cookbook and Meal Plan Recipes and Guidance For Life Before and After Surgery-ROCKRIDGE PRESS (2019)Documento335 pagineMegan Moore, RD - The Complete Bariatric Cookbook and Meal Plan Recipes and Guidance For Life Before and After Surgery-ROCKRIDGE PRESS (2019)savingtavia100% (5)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (74)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- Robert F Kushner - Christopher D Still - Nutrition and Bariatric Surgery (2014, Taylor & Francis, CRC Press) PDFDocumento298 pagineRobert F Kushner - Christopher D Still - Nutrition and Bariatric Surgery (2014, Taylor & Francis, CRC Press) PDFLucas PabloNessuna valutazione finora
- Abstract Book IFSO 2014Documento373 pagineAbstract Book IFSO 2014Sarah LawrenceNessuna valutazione finora
- PreviewpdfDocumento103 paginePreviewpdfHarsh ChordiyaNessuna valutazione finora
- Anaesthesia For The Obese PatientDocumento8 pagineAnaesthesia For The Obese Patientstephanus henryNessuna valutazione finora
- Bariatric SurgeryDocumento20 pagineBariatric SurgeryNadia AbbasNessuna valutazione finora
- Bariatric and Metabolic Surgery: Luigi Angrisani EditorDocumento209 pagineBariatric and Metabolic Surgery: Luigi Angrisani EditorBadri KobalavaNessuna valutazione finora
- QuestionnaireDocumento7 pagineQuestionnairenoctulius_moongod6002100% (1)
- DANTAS 2020 Exercise-Induced Increases in Insulin Sensitivity After Bariatric Surgery Are Mediated by Muscle Extracellular Matrix RemodelingDocumento17 pagineDANTAS 2020 Exercise-Induced Increases in Insulin Sensitivity After Bariatric Surgery Are Mediated by Muscle Extracellular Matrix RemodelingCris AquinoNessuna valutazione finora
- Case Study 2 Nutr484Documento11 pagineCase Study 2 Nutr484api-644004752Nessuna valutazione finora
- 2019 Guidelines Bariatric Surgery EAES SAGESDocumento29 pagine2019 Guidelines Bariatric Surgery EAES SAGESDra Maha HafezNessuna valutazione finora
- Surgical Treatment of ObesityDocumento13 pagineSurgical Treatment of ObesityDorothy HernándezNessuna valutazione finora
- Loyola MSBC Nutrition Guidelines For Bariatric SurgeryDocumento28 pagineLoyola MSBC Nutrition Guidelines For Bariatric Surgeryapi-240589558Nessuna valutazione finora
- Long-Term and Midterm Outcomes of SGL Vs LRYGBDocumento11 pagineLong-Term and Midterm Outcomes of SGL Vs LRYGBArmando Caballero AdamesNessuna valutazione finora
- Physical Exercise and Morbid Obesity: A Systematic ReviewDocumento7 paginePhysical Exercise and Morbid Obesity: A Systematic ReviewTito AlhoNessuna valutazione finora
- Lembar Jawaban Skillab Evidence Based Medicine (Ebm) Nama: Rafika Triasa NIM: 040427223270003Documento11 pagineLembar Jawaban Skillab Evidence Based Medicine (Ebm) Nama: Rafika Triasa NIM: 040427223270003Yahya Darmais FaridNessuna valutazione finora
- By: Emmeline M. Baltero, SNDocumento54 pagineBy: Emmeline M. Baltero, SNMichelle B. AloveraNessuna valutazione finora
- GastrointestinalDocumento16 pagineGastrointestinalCelestial, Maybelle MarieNessuna valutazione finora
- 2022 Obesity Management As A Primary Treatment Goal For Type 2Documento12 pagine2022 Obesity Management As A Primary Treatment Goal For Type 2Peter Albeiro Falla CortesNessuna valutazione finora
- Health Professionals - WKTDocumento3 pagineHealth Professionals - WKTtimesnewspapersNessuna valutazione finora
- Bariatric Surgery Pre Operative Liver Reduction DietDocumento3 pagineBariatric Surgery Pre Operative Liver Reduction DietSecret SurgeryNessuna valutazione finora
- Patient Education Guide: CHI Health Immanuel Bariatric Surgery ProgramDocumento84 paginePatient Education Guide: CHI Health Immanuel Bariatric Surgery ProgramAndrea SándezNessuna valutazione finora
- Lembar Jawaban Ebm EliskaDocumento30 pagineLembar Jawaban Ebm EliskaNovi YantiNessuna valutazione finora
- Weight ManagementDocumento88 pagineWeight Managementjohn millsNessuna valutazione finora
- Seminars in Pediatric SurgeryDocumento6 pagineSeminars in Pediatric SurgeryDr Venkatachalapathy T S Ped SurgeonNessuna valutazione finora
- Argumentitive Essay About Bariatric SurgeryDocumento2 pagineArgumentitive Essay About Bariatric SurgeryNourNessuna valutazione finora
- Case 2 Bariac SurgeryDocumento8 pagineCase 2 Bariac Surgeryapi-437425014100% (1)
- Gastroplicatura en Pacientes Con Reflujo y Gastrectomia VerticalDocumento9 pagineGastroplicatura en Pacientes Con Reflujo y Gastrectomia VerticalOoAldoONessuna valutazione finora
- Laparoscopic Weight Loss Surgery (Bariatric Surgery) : A Simple Guide To Help Answer Your QuestionsDocumento67 pagineLaparoscopic Weight Loss Surgery (Bariatric Surgery) : A Simple Guide To Help Answer Your QuestionsSAGESWebNessuna valutazione finora
- Morbid Obesity - Anaesthetic Management: Prevalence and EpidemiologyDocumento8 pagineMorbid Obesity - Anaesthetic Management: Prevalence and EpidemiologyLorena GarcíaNessuna valutazione finora