Potrebbero piacerti anche
- A Comparative Study of Typhidot and Widal Test For Rapid Diagnosis of Typhoid FeverDocumento5 pagineA Comparative Study of Typhidot and Widal Test For Rapid Diagnosis of Typhoid FeverArbusa86Nessuna valutazione finora
- IPIntJMedPaediatrOncol 7 1 41 45Documento5 pagineIPIntJMedPaediatrOncol 7 1 41 45Angelo FanusanNessuna valutazione finora
- Diagnostic Tyfoid 1Documento4 pagineDiagnostic Tyfoid 1Roberto SoehartonoNessuna valutazione finora
- Typhoid WidalDocumento4 pagineTyphoid WidalamaliamldNessuna valutazione finora
- 13 Jeyakumari EtalDocumento5 pagine13 Jeyakumari EtaleditorijmrhsNessuna valutazione finora
- Typoid Widal TestDocumento5 pagineTypoid Widal TestEnvhy AmaliaNessuna valutazione finora
- Accuracy of Widal vs blood culture for typhoid diagnosisDocumento3 pagineAccuracy of Widal vs blood culture for typhoid diagnosisRD ComputersNessuna valutazione finora
- Jurnal 5 Demam TypoidDocumento4 pagineJurnal 5 Demam TypoidAuliana Sania HanafiahNessuna valutazione finora
- Indro HandojoDocumento8 pagineIndro Handojonur syofiNessuna valutazione finora
- Asim,+prof +1726Documento6 pagineAsim,+prof +1726Zayn HNessuna valutazione finora
- Detection of Typhoid CarriersDocumento6 pagineDetection of Typhoid CarriersClarestaNessuna valutazione finora
- WidalDocumento3 pagineWidalkent harlendoNessuna valutazione finora
- Retrospective Audit of The Widal Test For Diagnosis of Typhoid Fever in Pediatric Patients in An Endemic RegionDocumento4 pagineRetrospective Audit of The Widal Test For Diagnosis of Typhoid Fever in Pediatric Patients in An Endemic RegionKiagus Mahendra EffendyNessuna valutazione finora
- Incidence of Typhoid Fever in Islamabad, Pakistan: September 2015Documento5 pagineIncidence of Typhoid Fever in Islamabad, Pakistan: September 2015Ulfat NiazyNessuna valutazione finora
- New Advances in The Rapid Diagnosis of Typhoid FevDocumento3 pagineNew Advances in The Rapid Diagnosis of Typhoid FevAarav MishraNessuna valutazione finora
- Diagnosis of Typhoid FeverDocumento5 pagineDiagnosis of Typhoid FeverpeterjongNessuna valutazione finora
- Bulletin of The World Health OrganizationDocumento11 pagineBulletin of The World Health OrganizationJohn LewandowskiNessuna valutazione finora
- Evaluation of Rapid Diagnostic Tests For Typhoid Fever: Ournal of Linical IcrobiologyDocumento5 pagineEvaluation of Rapid Diagnostic Tests For Typhoid Fever: Ournal of Linical IcrobiologyAjith NairNessuna valutazione finora
- Lokida 2020 Comparison of Commercial ELISA For Diagnosis of Acute Rickettsia Typhi InfectionsDocumento7 pagineLokida 2020 Comparison of Commercial ELISA For Diagnosis of Acute Rickettsia Typhi InfectionsRyan PratamaNessuna valutazione finora
- Tubex TestDocumento9 pagineTubex TestdnnivNessuna valutazione finora
- Journal of Clinical Microbiology-2004-Olsen-1885.fullDocumento5 pagineJournal of Clinical Microbiology-2004-Olsen-1885.fullRizka Putri HamuktionoNessuna valutazione finora
- Typhi-Specific Igm Antibodies and The Evolution of The ImmuneDocumento6 pagineTyphi-Specific Igm Antibodies and The Evolution of The ImmunefrankyNessuna valutazione finora
- Evaluation of Sensitivity and Specificity of ELISA Against Widal Test For Typhoid Diagnosis in Endemic Population of KathmanduDocumento8 pagineEvaluation of Sensitivity and Specificity of ELISA Against Widal Test For Typhoid Diagnosis in Endemic Population of KathmanduRiriMutammimaRizqiyaniNessuna valutazione finora
- Original Article: Clinical and Laboratory Features of Typhoid Fever in ChildhoodDocumento6 pagineOriginal Article: Clinical and Laboratory Features of Typhoid Fever in ChildhoodRidha Surya NugrahaNessuna valutazione finora
- High Prevalence of Azithromycin Resistance To Treponema Pallidum in Geographically Different Areas in ChinaDocumento5 pagineHigh Prevalence of Azithromycin Resistance To Treponema Pallidum in Geographically Different Areas in Chinaselvia emilyaNessuna valutazione finora
- Clinical Presentation and Laboratory Features in Pediatric Typhoid Fever Patient Susceptibility To First-Line Antibiotic TherapyDocumento10 pagineClinical Presentation and Laboratory Features in Pediatric Typhoid Fever Patient Susceptibility To First-Line Antibiotic TherapySuci ZahraniNessuna valutazione finora
- Accuracy of A Commercial Igm Elisa For The Diagnosis of Human Leptospirosis in ThailandDocumento4 pagineAccuracy of A Commercial Igm Elisa For The Diagnosis of Human Leptospirosis in Thailandrestu anindityaNessuna valutazione finora
- Sensitivity and Specificity of Typhoid Fever Rapid Antibody Tests For Laboratory Diagnosis at Two Sub-Saharan African SitesDocumento9 pagineSensitivity and Specificity of Typhoid Fever Rapid Antibody Tests For Laboratory Diagnosis at Two Sub-Saharan African SitesAde SupraptoNessuna valutazione finora
- Role of Widal Test in The Diagnosis of Typhoid Fever in Context To Other TestDocumento3 pagineRole of Widal Test in The Diagnosis of Typhoid Fever in Context To Other TestsimbawulaNessuna valutazione finora
- Value of Single Widal Test in Children For Diagnosis of Typhoid FeverDocumento5 pagineValue of Single Widal Test in Children For Diagnosis of Typhoid FeverArdita FaradhikaNessuna valutazione finora
- Comparative Study of Typhidot-M With Widal and Blood Culture in Diagnosis of Enteric FeverDocumento4 pagineComparative Study of Typhidot-M With Widal and Blood Culture in Diagnosis of Enteric FeverPranay BhosaleNessuna valutazione finora
- Diagnostic Value of Serological Tests (IgA, IgG, IgM)Documento4 pagineDiagnostic Value of Serological Tests (IgA, IgG, IgM)Gustomo PanantroNessuna valutazione finora
- Jurnal 2Documento12 pagineJurnal 2zingioNessuna valutazione finora
- Typhoid JournalDocumento7 pagineTyphoid JournalRegina AyediaNessuna valutazione finora
- JCDR 8 DC22 - 2Documento4 pagineJCDR 8 DC22 - 2manalNessuna valutazione finora
- Malaria or Typhoid Co-Infection in A Tertiary CareDocumento6 pagineMalaria or Typhoid Co-Infection in A Tertiary CareStephanie AndersonNessuna valutazione finora
- Comparing Widal and ELISA Tests for Diagnosing Typhoid Fever in Iraqi PatientsDocumento6 pagineComparing Widal and ELISA Tests for Diagnosing Typhoid Fever in Iraqi PatientsMildred MontNessuna valutazione finora
- 175 326 1 SMDocumento8 pagine175 326 1 SMElfiana IfaNessuna valutazione finora
- Ajmr 3 6 1 TyphoidfeverDocumento4 pagineAjmr 3 6 1 TyphoidfeverBikeshNessuna valutazione finora
- A Igm: Simple Adherence Test For Detection of Antibodies in TyphoidDocumento4 pagineA Igm: Simple Adherence Test For Detection of Antibodies in TyphoidguemadiNessuna valutazione finora
- Jurnal Respi - Comparison of IGRA AssayDocumento5 pagineJurnal Respi - Comparison of IGRA AssaykaynabilNessuna valutazione finora
- 1 SMDocumento7 pagine1 SMGeorge AniborNessuna valutazione finora
- Microbiolres 08 05564Documento4 pagineMicrobiolres 08 05564Prashant MishraNessuna valutazione finora
- Can A Rapid Test Justify As A Screening Test For Syphilis in Hard-To-Reach Population? Its EvaluationDocumento3 pagineCan A Rapid Test Justify As A Screening Test For Syphilis in Hard-To-Reach Population? Its EvaluationInternational Journal of Innovative Science and Research TechnologyNessuna valutazione finora
- Postgrad Med J 2000 Olopoenia 80 4Documento6 paginePostgrad Med J 2000 Olopoenia 80 4Christian Ivan SantosoNessuna valutazione finora
- 12 ArtikelDocumento8 pagine12 ArtikelArrahmi Hutami HasbilaNessuna valutazione finora
- Diagnosis of Typhoid Fever: Detection of Salmonella Typhi Porins-Specific Antibodies by Inhibition ELISADocumento6 pagineDiagnosis of Typhoid Fever: Detection of Salmonella Typhi Porins-Specific Antibodies by Inhibition ELISAguemadiNessuna valutazione finora
- Evaluation of A Simple and Rapid Dipstick Assay For The Diagnosis of Typhoid Fever in IndonesiaDocumento5 pagineEvaluation of A Simple and Rapid Dipstick Assay For The Diagnosis of Typhoid Fever in IndonesiaFauzi SatriaNessuna valutazione finora
- An Early Evaluation On The Usefulness of NS1 Antigen-Capture ELISA Versus IGM ELISA TEST For The Diagnosis of Acute Dengue InfectionDocumento10 pagineAn Early Evaluation On The Usefulness of NS1 Antigen-Capture ELISA Versus IGM ELISA TEST For The Diagnosis of Acute Dengue Infectionkurniawan naryoNessuna valutazione finora
- Typod in PapuaDocumento13 pagineTypod in PapuayogiNessuna valutazione finora
- 7611 193 16003 1 10 20180511 PDFDocumento6 pagine7611 193 16003 1 10 20180511 PDFUkhti Aisha Syafa Az-zahraNessuna valutazione finora
- 7611 193 16003 1 10 20180511 PDFDocumento6 pagine7611 193 16003 1 10 20180511 PDFEltriNessuna valutazione finora
- Gondii, Cytomegalovirus, and Rubella Virus InfectionsDocumento6 pagineGondii, Cytomegalovirus, and Rubella Virus InfectionsLucrezia Lo grassoNessuna valutazione finora
- Suleiman 1Documento8 pagineSuleiman 1elsa_imamNessuna valutazione finora
- 67 1437543936 PDFDocumento5 pagine67 1437543936 PDFrivandiNessuna valutazione finora
- MedicineDocumento7 pagineMedicineRatu Laura Baskara PutriNessuna valutazione finora
- WFVSDCSVSFDocumento7 pagineWFVSDCSVSFmuscadomNessuna valutazione finora
- Significance and Value of The Widal Test in The Diagnosis of Typhoid Fever in An Endemic AreaDocumento6 pagineSignificance and Value of The Widal Test in The Diagnosis of Typhoid Fever in An Endemic AreaDavide BorgesNessuna valutazione finora
- AUF Original ArticleDocumento8 pagineAUF Original Articleshikha tiwariNessuna valutazione finora
- NNNNNNNNNDocumento9 pagineNNNNNNNNNnurahmi widyani ratriNessuna valutazione finora
- Book 1Documento2 pagineBook 1nurahmi widyani ratriNessuna valutazione finora
- MMMDocumento19 pagineMMMnurahmi widyani ratriNessuna valutazione finora
- 12 - Chronic Care ManagementDocumento54 pagine12 - Chronic Care Managementnurahmi widyani ratriNessuna valutazione finora
- 1 s2.0 S1201971216310244 MainDocumento2 pagine1 s2.0 S1201971216310244 Mainnurahmi widyani ratriNessuna valutazione finora
- Jo 8 PDFDocumento5 pagineJo 8 PDFnurahmi widyani ratriNessuna valutazione finora
- Jo 8 PDFDocumento5 pagineJo 8 PDFnurahmi widyani ratriNessuna valutazione finora
- Kesici 2019Documento7 pagineKesici 2019nurahmi widyani ratriNessuna valutazione finora
- Trauma ServikalDocumento7 pagineTrauma Servikalnurahmi widyani ratriNessuna valutazione finora
- Nihms 604943Documento15 pagineNihms 604943nurahmi widyani ratriNessuna valutazione finora
- WHO-SEARO Snakebite Guidelines 2010Documento162 pagineWHO-SEARO Snakebite Guidelines 2010Galantry Ahmad AzhariNessuna valutazione finora
- 10.1177 2042018810382481Documento7 pagine10.1177 2042018810382481Je SoekocoNessuna valutazione finora
- Nihms 604943Documento15 pagineNihms 604943nurahmi widyani ratriNessuna valutazione finora
- Changes in Contrast Sensitivity in Young Adults With DiabetesDocumento5 pagineChanges in Contrast Sensitivity in Young Adults With Diabetesnurahmi widyani ratriNessuna valutazione finora
- Nihms 604943Documento15 pagineNihms 604943nurahmi widyani ratriNessuna valutazione finora
- Trauma Induce Coagulopaty AAH JurnalDocumento4 pagineTrauma Induce Coagulopaty AAH Jurnalnurahmi widyani ratriNessuna valutazione finora
- Breastfeeding Management: Hours To Two WeeksDocumento2 pagineBreastfeeding Management: Hours To Two Weeksnurahmi widyani ratriNessuna valutazione finora
- Evaluasi Konseling Menyusui PDFDocumento9 pagineEvaluasi Konseling Menyusui PDFErica FitrianiNessuna valutazione finora
- CASP Case Control Study Checklist DownloadDocumento6 pagineCASP Case Control Study Checklist DownloadbintangNessuna valutazione finora
- Muchiri 2016Documento10 pagineMuchiri 2016nurahmi widyani ratriNessuna valutazione finora
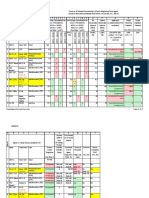
- Rundown Acara ADocumento5 pagineRundown Acara Anurahmi widyani ratriNessuna valutazione finora
- DDDDDFDocumento1 paginaDDDDDFnurahmi widyani ratriNessuna valutazione finora
- ACP Board ReviewDocumento593 pagineACP Board ReviewC Martin TraumatoNessuna valutazione finora
- Increased Mortality Associated With The Early Coagulopathy of Trauma in Combat CasualtiesDocumento7 pagineIncreased Mortality Associated With The Early Coagulopathy of Trauma in Combat Casualtiesnurahmi widyani ratriNessuna valutazione finora
- CASP Randomised Controlled Trial Checklist 2018 Fillable FormDocumento14 pagineCASP Randomised Controlled Trial Checklist 2018 Fillable Formnurahmi widyani ratriNessuna valutazione finora
- ADocumento1 paginaAnurahmi widyani ratriNessuna valutazione finora
- Diagnosis and Management of Acute Low Back PainDocumento2 pagineDiagnosis and Management of Acute Low Back Painnurahmi widyani ratriNessuna valutazione finora
- JBI Quasi-Experimental Appraisal Tool2017Documento7 pagineJBI Quasi-Experimental Appraisal Tool2017nurahmi widyani ratriNessuna valutazione finora
- Factsheet B2B PunchOut en 140623Documento2 pagineFactsheet B2B PunchOut en 140623Curtis GibsonNessuna valutazione finora
- Cold Forging Process TutorialDocumento28 pagineCold Forging Process TutorialpanyamnrNessuna valutazione finora
- SD-SCD-QF75 - Factory Audit Checklist - Rev.1 - 16 Sept.2019Documento6 pagineSD-SCD-QF75 - Factory Audit Checklist - Rev.1 - 16 Sept.2019Lawrence PeNessuna valutazione finora
- Time Table For Winter 2023 Theory ExaminationDocumento1 paginaTime Table For Winter 2023 Theory ExaminationSushant kakadeNessuna valutazione finora
- Weekly Choice - Section B - February 16, 2012Documento10 pagineWeekly Choice - Section B - February 16, 2012Baragrey DaveNessuna valutazione finora
- Standard Deviation IntroductionDocumento3 pagineStandard Deviation IntroductionShyam ShresthaNessuna valutazione finora
- Empowerment Technology Reviewer: First SemesterDocumento5 pagineEmpowerment Technology Reviewer: First SemesterNinayD.MatubisNessuna valutazione finora
- Positioning for competitive advantageDocumento9 paginePositioning for competitive advantageOnos Bunny BenjaminNessuna valutazione finora
- NameDocumento5 pagineNameMaine DagoyNessuna valutazione finora
- Micropolar Fluid Flow Near The Stagnation On A Vertical Plate With Prescribed Wall Heat Flux in Presence of Magnetic FieldDocumento8 pagineMicropolar Fluid Flow Near The Stagnation On A Vertical Plate With Prescribed Wall Heat Flux in Presence of Magnetic FieldIJBSS,ISSN:2319-2968Nessuna valutazione finora
- Machine Spindle Noses: 6 Bison - Bial S. ADocumento2 pagineMachine Spindle Noses: 6 Bison - Bial S. AshanehatfieldNessuna valutazione finora
- Testbanks ch24Documento12 pagineTestbanks ch24Hassan ArafatNessuna valutazione finora
- C Exam13Documento4 pagineC Exam13gauravsoni1991Nessuna valutazione finora
- All Associates Warning Against ChangesDocumento67 pagineAll Associates Warning Against Changesramesh0% (1)
- Reflection Paper #1 - Introduction To Action ResearchDocumento1 paginaReflection Paper #1 - Introduction To Action Researchronan.villagonzaloNessuna valutazione finora
- Tender Notice and Invitation To TenderDocumento1 paginaTender Notice and Invitation To TenderWina George MuyundaNessuna valutazione finora
- Human Resouse Accounting Nature and Its ApplicationsDocumento12 pagineHuman Resouse Accounting Nature and Its ApplicationsParas JainNessuna valutazione finora
- Expressive Matter Vendor FaqDocumento14 pagineExpressive Matter Vendor FaqRobert LedermanNessuna valutazione finora
- Environmental Technology Syllabus-2019Documento2 pagineEnvironmental Technology Syllabus-2019Kxsns sjidNessuna valutazione finora
- Chapter 2Documento22 pagineChapter 2Okorie Chinedu PNessuna valutazione finora
- Emergency Room Delivery RecordDocumento7 pagineEmergency Room Delivery RecordMariel VillamorNessuna valutazione finora
- FALL PROTECTION ON SCISSOR LIFTS PDF 2 PDFDocumento3 pagineFALL PROTECTION ON SCISSOR LIFTS PDF 2 PDFJISHNU TKNessuna valutazione finora
- TransistorDocumento1 paginaTransistorXhaNessuna valutazione finora
- Inventarisasi Data Kondisi Jalan Ke Dalam Aplikasi Sistem Informasi Geografis (Sig)Documento10 pagineInventarisasi Data Kondisi Jalan Ke Dalam Aplikasi Sistem Informasi Geografis (Sig)Wiro SablengNessuna valutazione finora
- Rhodes Motion For Judicial NoticeDocumento493 pagineRhodes Motion For Judicial Noticewolf woodNessuna valutazione finora
- Florence Walking Tour MapDocumento14 pagineFlorence Walking Tour MapNguyễn Tấn QuangNessuna valutazione finora
- Lecture 1: Newton Forward and Backward Interpolation: M R Mishra May 9, 2022Documento10 pagineLecture 1: Newton Forward and Backward Interpolation: M R Mishra May 9, 2022MANAS RANJAN MISHRANessuna valutazione finora
- Clean Agent ComparisonDocumento9 pagineClean Agent ComparisonJohn ANessuna valutazione finora
- Term Sheet: Original Borrowers) Material Subsidiaries/jurisdiction) )Documento16 pagineTerm Sheet: Original Borrowers) Material Subsidiaries/jurisdiction) )spachecofdz0% (1)
- The Sound Collector - The Prepared Piano of John CageDocumento12 pagineThe Sound Collector - The Prepared Piano of John CageLuigie VazquezNessuna valutazione finora