Potrebbero piacerti anche
- Parent Guardian(s) Surrogate Parent(s)Documento6 pagineParent Guardian(s) Surrogate Parent(s)Zach SelnesNessuna valutazione finora
- Anatomic and Physiologic Overview of The BrainDocumento5 pagineAnatomic and Physiologic Overview of The BrainIlona Rosabel Bitalac0% (1)
- Guidelines Down Syndrome Assessment and Intervention PDFDocumento292 pagineGuidelines Down Syndrome Assessment and Intervention PDFZenithaMeidaNessuna valutazione finora
- Spinal Muscular Atrophy-2Documento10 pagineSpinal Muscular Atrophy-2api-344309408Nessuna valutazione finora
- Muscular DystrophyDocumento48 pagineMuscular DystrophySai BruhathiNessuna valutazione finora
- GmfmscoresheetDocumento6 pagineGmfmscoresheetapi-260049180Nessuna valutazione finora
- Common Rotational Variations in ChildrenDocumento9 pagineCommon Rotational Variations in ChildrendamonenNessuna valutazione finora
- Pediatric Acute Transverse Myelitis Overview and Differential DiagnosisDocumento12 paginePediatric Acute Transverse Myelitis Overview and Differential Diagnosismmoraes0709Nessuna valutazione finora
- Manual TherapyDocumento16 pagineManual TherapylecturioNessuna valutazione finora
- Developmental Milestones (Complete)Documento14 pagineDevelopmental Milestones (Complete)KIARA VENICE DELGADONessuna valutazione finora
- Barthel vs. FIMDocumento5 pagineBarthel vs. FIMFrancisco CampoverdeNessuna valutazione finora
- Child Growth and Development: Department of Pediatrics Soochow University Affiliated Children's HospitalDocumento67 pagineChild Growth and Development: Department of Pediatrics Soochow University Affiliated Children's HospitalAi ChanNessuna valutazione finora
- Bayley ReviewDocumento12 pagineBayley ReviewagNessuna valutazione finora
- TheoriesDocumento2 pagineTheoriesAngie MandeoyaNessuna valutazione finora
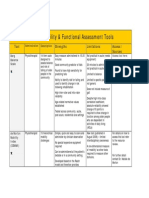
- Mobility and Functional Assessment ToolsDocumento4 pagineMobility and Functional Assessment Toolssonya63265Nessuna valutazione finora
- DyslexiaDocumento19 pagineDyslexiaJubie MathewNessuna valutazione finora
- Health-Related Quality of LifeDocumento23 pagineHealth-Related Quality of LifeHope GemidaNessuna valutazione finora
- Assessment of HandDocumento76 pagineAssessment of Handchirag0% (1)
- Cerebral PalsyDocumento80 pagineCerebral PalsyYuusuf MubarikNessuna valutazione finora
- Sample Neuro H&PDocumento3 pagineSample Neuro H&Pethereal45Nessuna valutazione finora
- OTB 502 Syllabus 2019Documento22 pagineOTB 502 Syllabus 2019Gehan BotorsNessuna valutazione finora
- Motor MildstonesDocumento13 pagineMotor MildstonesVaio Wolff AbendrothNessuna valutazione finora
- Seclusion and Restraints Final ReportDocumento54 pagineSeclusion and Restraints Final Reportjuliepipip23Nessuna valutazione finora
- Effect of Parent-Delivered Action Observation Therapy On Upper Limb Function in Unilateral Cerebral PalsyDocumento40 pagineEffect of Parent-Delivered Action Observation Therapy On Upper Limb Function in Unilateral Cerebral PalsyNovaria Puspita SamudraNessuna valutazione finora
- Development Chart For BookletDocumento13 pagineDevelopment Chart For BookletzapelNessuna valutazione finora
- ICF and Clinical ReasoningDocumento38 pagineICF and Clinical ReasoningKavitha RajaNessuna valutazione finora
- Neuro Case Study 1Documento2 pagineNeuro Case Study 1AngelaWise100% (1)
- Clinical Assesment in Pediatrics, Growth and Developement, Psychomotor Development - KópiaDocumento42 pagineClinical Assesment in Pediatrics, Growth and Developement, Psychomotor Development - Kópiamichal ben meronNessuna valutazione finora
- FIM ManualDocumento24 pagineFIM ManualAnshuman MihirNessuna valutazione finora
- Pediatric Outcome MeasuresDocumento40 paginePediatric Outcome MeasuresMaybelle Anne ZamoraNessuna valutazione finora
- Assess Screen Tools 2Documento17 pagineAssess Screen Tools 2hashem111Nessuna valutazione finora
- The Hand TestDocumento2 pagineThe Hand TestRhea CaasiNessuna valutazione finora
- Neuro Final Exam ReviewDocumento23 pagineNeuro Final Exam ReviewAaron James GrayNessuna valutazione finora
- Acute Flaccid Paralysis (AFP) Reportable DiseaseDocumento1 paginaAcute Flaccid Paralysis (AFP) Reportable DiseaseAuliyaa Rahmah100% (1)
- The University of Lahore, Lahore.: Cerebral PalsyDocumento16 pagineThe University of Lahore, Lahore.: Cerebral Palsynosheen murtazaNessuna valutazione finora
- Guide To Child Nonverbal Iq MeasuresDocumento16 pagineGuide To Child Nonverbal Iq MeasuresRachel FranzenNessuna valutazione finora
- The Gross Motor Function Classification System For Cerebral PalsyDocumento5 pagineThe Gross Motor Function Classification System For Cerebral PalsyMarco Tulio FigueroaNessuna valutazione finora
- Intellectual DisablitiesDocumento21 pagineIntellectual DisablitiesKamal SahimNessuna valutazione finora
- Functional Assessment: DR Sonali Soumyashree BPT, MPT (Neurology) Lecturer, GDGUDocumento15 pagineFunctional Assessment: DR Sonali Soumyashree BPT, MPT (Neurology) Lecturer, GDGUSonali Soumyashree100% (2)
- Cerebral Palsy SlidesDocumento22 pagineCerebral Palsy Slidesapi-301967651Nessuna valutazione finora
- GMFMDocumento1 paginaGMFMFlorin Dragos Caprita100% (1)
- Einspieler Etal JPsychol 2008Documento7 pagineEinspieler Etal JPsychol 2008ramopavelNessuna valutazione finora
- Cns Infection: Dr. Herbowo Af Soetomenggolo Spa (K)Documento52 pagineCns Infection: Dr. Herbowo Af Soetomenggolo Spa (K)Fadia RasyiddahNessuna valutazione finora
- MotivateDocumento9 pagineMotivateVukashin.meNessuna valutazione finora
- Developmental AssessmentDocumento4 pagineDevelopmental AssessmentFranzine Elyzyvette VillarNessuna valutazione finora
- DDSTDocumento2 pagineDDSTsurender_singh_43Nessuna valutazione finora
- Angelman SyndromeDocumento16 pagineAngelman SyndromeThe Rat100% (3)
- Beery Vmi Performance in Autism Spectrum DisorderDocumento33 pagineBeery Vmi Performance in Autism Spectrum DisorderJayminertri Minorous100% (1)
- Develop Med Child Neuro - 2021 - Einspieler - Fetal Movements The Origin of Human BehaviourDocumento8 pagineDevelop Med Child Neuro - 2021 - Einspieler - Fetal Movements The Origin of Human BehaviourGabriela Moreno Yates100% (1)
- Neuro PEDocumento36 pagineNeuro PEkhaderbasha2020Nessuna valutazione finora
- Blood GroupingDocumento35 pagineBlood GroupingSUNIL KUMARNessuna valutazione finora
- DDST 2Documento11 pagineDDST 2Ibnu Fadirul WahedNessuna valutazione finora
- Developmental MilestonesDocumento38 pagineDevelopmental Milestonesryguy178100% (1)
- Month Questionnaire: Ages & Stages QuestionnairesDocumento7 pagineMonth Questionnaire: Ages & Stages QuestionnairesamaliakhoirunnisaNessuna valutazione finora
- Growth and Development in ChildrenDocumento118 pagineGrowth and Development in ChildrenVidya kiranNessuna valutazione finora
- CCRN Pediatricdemo PDFDocumento9 pagineCCRN Pediatricdemo PDFBARKHA VERMANessuna valutazione finora
- Rubric Mini PracticalDocumento2 pagineRubric Mini PracticalAigen OcampoNessuna valutazione finora
- Trunk Impairment ScaleDocumento11 pagineTrunk Impairment ScaleRavneet singhNessuna valutazione finora
- Trunk Impairment ScaleDocumento11 pagineTrunk Impairment Scale林良駿Nessuna valutazione finora
- Inter - and Intra-Rater Reliability of The B Lindmark Motor Assessment.Documento6 pagineInter - and Intra-Rater Reliability of The B Lindmark Motor Assessment.Raluca HereaNessuna valutazione finora
- The Relationship Between The Academic Procrastination and Self-Efficacy Among Sample of King Saud University StudentsDocumento12 pagineThe Relationship Between The Academic Procrastination and Self-Efficacy Among Sample of King Saud University StudentsJayson OcoNessuna valutazione finora
- Organizational Agility ScaleDocumento15 pagineOrganizational Agility ScaleSaba Munir100% (1)
- Mobile Games and Academic Performance of University StudentsDocumento7 pagineMobile Games and Academic Performance of University StudentsMarianita Jane P. BatinNessuna valutazione finora
- Action and Cognition in Task Oriented Coping: Factor Structure and Internal Consistency of The CISS-21 With An Indian SampleDocumento27 pagineAction and Cognition in Task Oriented Coping: Factor Structure and Internal Consistency of The CISS-21 With An Indian SampleChita Dana StefaniaNessuna valutazione finora
- A Critical Study of Human Resource Development Practices in Durgapur Steel PlantDocumento14 pagineA Critical Study of Human Resource Development Practices in Durgapur Steel PlantSaaleh AminNessuna valutazione finora
- McCullough Et Al. (1998) - Interpersonal Forgiving in Close Relationships-II-Theoretical Elaboration and MeasurementDocumento18 pagineMcCullough Et Al. (1998) - Interpersonal Forgiving in Close Relationships-II-Theoretical Elaboration and MeasurementTheRealyReallEngaliNessuna valutazione finora
- Getting Serious About Test-Retest Reliability: A Critique of Retest Research and Some RecommendationsDocumento8 pagineGetting Serious About Test-Retest Reliability: A Critique of Retest Research and Some Recommendationslengers poworNessuna valutazione finora
- Impact of Buying Behavior of Youth Towards Cosmetic Products in Perambalur TownDocumento10 pagineImpact of Buying Behavior of Youth Towards Cosmetic Products in Perambalur TownDeepuNessuna valutazione finora
- Data Analysis & InterpretationDocumento51 pagineData Analysis & InterpretationSouvik BakshiNessuna valutazione finora
- The Use Ofthe General Health Questionnaire As An Indicator of Mental Health in Occupational StudiesDocumento9 pagineThe Use Ofthe General Health Questionnaire As An Indicator of Mental Health in Occupational Studiesabrudan_silviaNessuna valutazione finora
- Peters (2014) The Alpha and The Omega of Scale Reliability and ValidityDocumento15 paginePeters (2014) The Alpha and The Omega of Scale Reliability and ValidityEmanuel CordeiroNessuna valutazione finora
- Empirical Study of Schedule Delay in Moroccan Construction ProjectsDocumento19 pagineEmpirical Study of Schedule Delay in Moroccan Construction ProjectsMomen AlodatNessuna valutazione finora
- REVISAR Escala de Lectura Funcional 2014Documento10 pagineREVISAR Escala de Lectura Funcional 2014Luz TamarNessuna valutazione finora
- The Smartpls Analyzes Approach in Validity and Reliability of Graduate Marketability InstrumentDocumento16 pagineThe Smartpls Analyzes Approach in Validity and Reliability of Graduate Marketability InstrumentSakinah Mhd ShukreeNessuna valutazione finora
- 12.effects of Anonymity, Media Richness, and Chat-Room Activeness On Online ChattingDocumento13 pagine12.effects of Anonymity, Media Richness, and Chat-Room Activeness On Online ChattingBlayel FelihtNessuna valutazione finora
- Role of Religious Orientation and Mental Health On Critical Thinking Among AcademiciansDocumento9 pagineRole of Religious Orientation and Mental Health On Critical Thinking Among AcademiciansGlobal Research and Development ServicesNessuna valutazione finora
- MKTG9 Questionnaire Pilot Study ResultDocumento5 pagineMKTG9 Questionnaire Pilot Study ResultKyrie JalijaliNessuna valutazione finora
- 91 33 PBDocumento271 pagine91 33 PBnajamuddinNessuna valutazione finora
- CronbachDocumento7 pagineCronbachhersheeyoNessuna valutazione finora
- Job Satisfaction Scale: Shagufta Munir, Tahira KhatoonDocumento4 pagineJob Satisfaction Scale: Shagufta Munir, Tahira KhatoonrlynmndzNessuna valutazione finora
- Differentiation of Self Inventory PDFDocumento12 pagineDifferentiation of Self Inventory PDFCaulfield DariaNessuna valutazione finora
- Kenny Music Performance Anxiety Inventory KMPAI TRDocumento4 pagineKenny Music Performance Anxiety Inventory KMPAI TRCão MauzãoNessuna valutazione finora
- The Career Maturity Inventory Revised A Preliminary Psychometric InvestigationDocumento17 pagineThe Career Maturity Inventory Revised A Preliminary Psychometric InvestigationJorge Luis Villacís Nieto100% (1)
- Ijrtem G021046051 PDFDocumento6 pagineIjrtem G021046051 PDFjournalNessuna valutazione finora
- Mba Project ReportDocumento37 pagineMba Project ReportSyed Farhaan AhmedNessuna valutazione finora
- The Impact of Strategic Planning On Crisis Management Styles in The 5-Star HotelsDocumento10 pagineThe Impact of Strategic Planning On Crisis Management Styles in The 5-Star HotelsVarun AVNessuna valutazione finora
- Parent Behavior Importance and Parent Behavior Frequency Questionnaires: Psychometric CharacteristicsDocumento14 pagineParent Behavior Importance and Parent Behavior Frequency Questionnaires: Psychometric CharacteristicsmerawatidyahsepitaNessuna valutazione finora
- Critical Care Nurses' Knowledge, Attitudes, and Perceived Barriers Towards Pressure Injuries PreventionDocumento6 pagineCritical Care Nurses' Knowledge, Attitudes, and Perceived Barriers Towards Pressure Injuries PreventionzaynmalikNessuna valutazione finora
- ASM1 5060 NganNTTDocumento17 pagineASM1 5060 NganNTTThanh Ngân NguyễnNessuna valutazione finora
- Monitoring and Evaluation Final PaperDocumento13 pagineMonitoring and Evaluation Final PaperDilshad AhmadNessuna valutazione finora