Potrebbero piacerti anche
- Cell J 13 65 2 PDFDocumento8 pagineCell J 13 65 2 PDFRaissaNessuna valutazione finora
- Add Slide AbberationDocumento119 pagineAdd Slide AbberationRaissaNessuna valutazione finora
- PERIPHERAL ULCERATIVE KERATITIS (PUK) AND MOOREN'S ULCER: PATHOGENESIS AND TREATMENTDocumento35 paginePERIPHERAL ULCERATIVE KERATITIS (PUK) AND MOOREN'S ULCER: PATHOGENESIS AND TREATMENTRaissaNessuna valutazione finora
- Pasien RSWBDocumento6 paginePasien RSWBRaissaNessuna valutazione finora
- Management of Giant Gastric Ulcer Perforation RepoDocumento4 pagineManagement of Giant Gastric Ulcer Perforation Reporiski dwi sudaenyNessuna valutazione finora
- Abdominal OperationDocumento9 pagineAbdominal OperationRaissaNessuna valutazione finora
- Assessing visual function of commercial drivers in Rivers StateDocumento8 pagineAssessing visual function of commercial drivers in Rivers StateRaissaNessuna valutazione finora
- Refraction ManagementDocumento8 pagineRefraction ManagementRaissaNessuna valutazione finora
- Opth 10 879Documento8 pagineOpth 10 879Naindy Gita SafitriNessuna valutazione finora
- Dry EyeDocumento106 pagineDry EyeRaissa100% (1)
- RAAB Di IndonesiaDocumento42 pagineRAAB Di IndonesiaRaissa100% (2)
- Seidel2015 PDFDocumento5 pagineSeidel2015 PDFRaissaNessuna valutazione finora
- Dry EyeDocumento129 pagineDry EyeRaissa100% (3)
- Resume Tugas Akademik 8-Journal Reading 5-REFDocumento3 pagineResume Tugas Akademik 8-Journal Reading 5-REFRaissaNessuna valutazione finora
- Venousdrainageofheadandneck 150107032819 Conversion Gate02Documento78 pagineVenousdrainageofheadandneck 150107032819 Conversion Gate02RaissaNessuna valutazione finora
- Sensory PhysiologyDocumento34 pagineSensory PhysiologyRaissaNessuna valutazione finora
- OCT Classification of Macular HoleDocumento80 pagineOCT Classification of Macular HoleRaissaNessuna valutazione finora
- Kasus DM PDFDocumento22 pagineKasus DM PDFVidia AsriyantiNessuna valutazione finora
- GonioskopiDocumento40 pagineGonioskopiRaissaNessuna valutazione finora
- Cryotherapy FinishingDocumento50 pagineCryotherapy FinishingRaissaNessuna valutazione finora
- Pediatric Eye Examination: Seia MahananiDocumento35 paginePediatric Eye Examination: Seia MahananiRaissaNessuna valutazione finora
- General Principle & Eye DevelopmentDocumento28 pagineGeneral Principle & Eye DevelopmentRaissaNessuna valutazione finora
- Viper 3Documento5 pagineViper 3RaissaNessuna valutazione finora
- Reflex PupilDocumento21 pagineReflex PupilRaissaNessuna valutazione finora
- Arbonic Anhydrase ArinDocumento11 pagineArbonic Anhydrase ArinAndriati NadhilaNessuna valutazione finora
- SPR1 PDFDocumento17 pagineSPR1 PDFRaissaNessuna valutazione finora
- Difference Between Gram Positive and Gram Negative Bacteria: April 2017Documento14 pagineDifference Between Gram Positive and Gram Negative Bacteria: April 2017Da BondadNessuna valutazione finora
- Understanding Trabecular Meshwork Physiology: A Key To The Control of Intraocular Pressure?Documento5 pagineUnderstanding Trabecular Meshwork Physiology: A Key To The Control of Intraocular Pressure?RaissaNessuna valutazione finora
- Viper 1Documento6 pagineViper 1RaissaNessuna valutazione finora
- Resume. Tugas Akademik I. Journal Reading I. Tumor Trauma Rekonstruksi.Documento2 pagineResume. Tugas Akademik I. Journal Reading I. Tumor Trauma Rekonstruksi.RaissaNessuna valutazione finora
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (399)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (890)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (587)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (265)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (72)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (119)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- National TLD transition and viral load monitoringDocumento18 pagineNational TLD transition and viral load monitoringSemeeeJuniorNessuna valutazione finora
- Hormones Beta HCG - SerumDocumento1 paginaHormones Beta HCG - SerumsaniyaNessuna valutazione finora
- Brundin Et Al-2019-Acta Psychiatrica ScandinavicaDocumento3 pagineBrundin Et Al-2019-Acta Psychiatrica ScandinavicaSeleccion PersonalNessuna valutazione finora
- Agnikumara Rasa A Herbo Mineral Formulation ReviewDocumento3 pagineAgnikumara Rasa A Herbo Mineral Formulation ReviewEditor IJTSRDNessuna valutazione finora
- 2015 Winter Newsletter WebDocumento8 pagine2015 Winter Newsletter WebandreymaNessuna valutazione finora
- CKD SCT DNDocumento55 pagineCKD SCT DNKim Jun-myeonNessuna valutazione finora
- Assessment Tool EpcbDocumento5 pagineAssessment Tool EpcbJered MoratoNessuna valutazione finora
- Diabetes Mellitus and Prosthodontic Care Chanchal Katariya & Dr. SangeethaDocumento3 pagineDiabetes Mellitus and Prosthodontic Care Chanchal Katariya & Dr. SangeethaKrupali JainNessuna valutazione finora
- Experimentica Ltd. Announces The Successful Acquisition of The Ophthalmic Contract Research Division From Ophthy-DS, Inc.Documento3 pagineExperimentica Ltd. Announces The Successful Acquisition of The Ophthalmic Contract Research Division From Ophthy-DS, Inc.PR.comNessuna valutazione finora
- Nursing Implications Filipino & German HeritageDocumento4 pagineNursing Implications Filipino & German HeritageArmstrong AsenaviNessuna valutazione finora
- Oresol Preparation...............Documento24 pagineOresol Preparation...............shielamarie06_ramos3821100% (2)
- Excerpt From "The Last Walk: Reflections On Our Pets at The End of Their Lives" by Jessica PierceDocumento4 pagineExcerpt From "The Last Walk: Reflections On Our Pets at The End of Their Lives" by Jessica Piercewamu885Nessuna valutazione finora
- Applying The Chronic Care Model in Low-Resource Settings Ada Dec2013Documento44 pagineApplying The Chronic Care Model in Low-Resource Settings Ada Dec2013Wawan JokoNessuna valutazione finora
- Altered Urinary Elimination - ADPCN Resource UnitDocumento5 pagineAltered Urinary Elimination - ADPCN Resource UnitChillette FarraronsNessuna valutazione finora
- Research Article: (Occlu-Pad) DeviceDocumento5 pagineResearch Article: (Occlu-Pad) Devicearyo aryoNessuna valutazione finora
- Interview With T.C. FryDocumento18 pagineInterview With T.C. Fryraweater100% (1)
- Rorational Atherectomy - Technical Update Mota Et AlDocumento8 pagineRorational Atherectomy - Technical Update Mota Et AlhamartinezNessuna valutazione finora
- HFMEA FormDocumento6 pagineHFMEA FormAnonymous HofOUrbNessuna valutazione finora
- 11 ADocumento5 pagine11 AJrar YapNessuna valutazione finora
- Peritonitis and Intra-Abdominal Abscess Diagnosis TreatmentDocumento16 paginePeritonitis and Intra-Abdominal Abscess Diagnosis TreatmentPekerja KesunyianNessuna valutazione finora
- Methylprednisolone Article 35 Referral Questions Answers Veterinary Medicinal Products Containing - enDocumento2 pagineMethylprednisolone Article 35 Referral Questions Answers Veterinary Medicinal Products Containing - enRajuNessuna valutazione finora
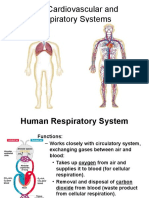
- Cardiovascular and Respiratory SystemDocumento51 pagineCardiovascular and Respiratory SystemKarel Mae SanoriaNessuna valutazione finora
- Safety Tips For Covid-19Documento5 pagineSafety Tips For Covid-19Angelo AsoqueNessuna valutazione finora
- Combustio: DR - Dian SyahputraDocumento35 pagineCombustio: DR - Dian SyahputraYulliza Kurniawaty LNessuna valutazione finora
- Brochure On Mental Health InitiativeDocumento2 pagineBrochure On Mental Health InitiativeantaraNessuna valutazione finora
- Diphtheria and Pertussis: Causes, Symptoms and PreventionDocumento30 pagineDiphtheria and Pertussis: Causes, Symptoms and Preventioneman khammasNessuna valutazione finora
- Diabetes MellitusDocumento11 pagineDiabetes MellitusChristinaRegatilloNessuna valutazione finora
- Caz PatologieDocumento5 pagineCaz PatologieBarbulescu Anca DianaNessuna valutazione finora
- A Comparative Clinical Study ofDocumento11 pagineA Comparative Clinical Study ofArter AdamNessuna valutazione finora
- Assignment 3 (Clerkship)Documento11 pagineAssignment 3 (Clerkship)Ataur RahmanNessuna valutazione finora