Potrebbero piacerti anche
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- Rugged 5-In-1 Environmental MeterDocumento1 paginaRugged 5-In-1 Environmental MeterpaniyaNessuna valutazione finora
- Brass Low Pressure Ball ValvesDocumento1 paginaBrass Low Pressure Ball ValvespaniyaNessuna valutazione finora
- ZLT s10 Dialog UsermanualDocumento2 pagineZLT s10 Dialog Usermanualpaniya100% (1)
- Removal & Installation: Suspension Tire Pressure Monitoring System - Service Information - HR-VDocumento1 paginaRemoval & Installation: Suspension Tire Pressure Monitoring System - Service Information - HR-VpaniyaNessuna valutazione finora
- Gree Manual p5Documento13 pagineGree Manual p5paniyaNessuna valutazione finora
- Gree Manual p3Documento13 pagineGree Manual p3paniyaNessuna valutazione finora
- Gree Manual p4Documento13 pagineGree Manual p4paniyaNessuna valutazione finora
- Removal & Installation: Steering EPS Motor / Control Unit - Service Information - HR-VDocumento2 pagineRemoval & Installation: Steering EPS Motor / Control Unit - Service Information - HR-VpaniyaNessuna valutazione finora
- Gree Manual p1Documento13 pagineGree Manual p1paniyaNessuna valutazione finora
- DTC Troubleshooting: Before You Troubleshoot, Review The General Troubleshooting InformationDocumento32 pagineDTC Troubleshooting: Before You Troubleshoot, Review The General Troubleshooting InformationpaniyaNessuna valutazione finora
- S-849 - December 2018 Page - 6Documento1 paginaS-849 - December 2018 Page - 6paniyaNessuna valutazione finora
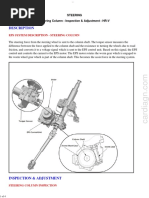
- Description: Steering Steering Column - Inspection & Adjustment - HR-VDocumento4 pagineDescription: Steering Steering Column - Inspection & Adjustment - HR-VpaniyaNessuna valutazione finora
- Description: Eps System Description - Eps ControlDocumento34 pagineDescription: Eps System Description - Eps ControlpaniyaNessuna valutazione finora
- Torque Specifications (Ka/Kc Models)Documento5 pagineTorque Specifications (Ka/Kc Models)paniyaNessuna valutazione finora
- Helix Portable Ventilators: Sustainable First Choice FlexibleDocumento3 pagineHelix Portable Ventilators: Sustainable First Choice FlexiblepaniyaNessuna valutazione finora
- Datenblatt / Data Sheet U51DL-012KK-5Documento6 pagineDatenblatt / Data Sheet U51DL-012KK-5paniyaNessuna valutazione finora
- Ambu PEEP ValvesDocumento2 pagineAmbu PEEP ValvespaniyaNessuna valutazione finora
- S-849 - December 2018 Page - 5Documento1 paginaS-849 - December 2018 Page - 5paniyaNessuna valutazione finora
- Diaphragm Pump - CompressorDocumento2 pagineDiaphragm Pump - CompressorpaniyaNessuna valutazione finora
- S-849 - December 2018 Page - 3Documento1 paginaS-849 - December 2018 Page - 3paniyaNessuna valutazione finora
- Sash Cross SectionDocumento2 pagineSash Cross Sectionpaniya100% (1)
- AUS PEEPValves 493480097 V02 0712Documento2 pagineAUS PEEPValves 493480097 V02 0712paniyaNessuna valutazione finora
- 02 Lectures OpenFOAM Solver ModificationDocumento33 pagine02 Lectures OpenFOAM Solver ModificationpaniyaNessuna valutazione finora
- Datenblatt / Data Sheet U51DL-012KK-5Documento6 pagineDatenblatt / Data Sheet U51DL-012KK-5paniyaNessuna valutazione finora
- Arici CHP VIIDocumento44 pagineArici CHP VIIpaniyaNessuna valutazione finora
- Ordering Specifications: Item No. DescriptionDocumento1 paginaOrdering Specifications: Item No. DescriptionpaniyaNessuna valutazione finora
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (74)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- Systematic Approach To Managing Vernal Keratoconjunctivitis in Clinical Practice Severity Grading System and A Treatment AlgorithmDocumento4 pagineSystematic Approach To Managing Vernal Keratoconjunctivitis in Clinical Practice Severity Grading System and A Treatment AlgorithmifarakhaNessuna valutazione finora
- Oral Versus Topical NSAIDs in Rheumatic DiseasesDocumento21 pagineOral Versus Topical NSAIDs in Rheumatic DiseasesAnonymous so6ZnlKywNessuna valutazione finora
- 05 Forms of DrugsDocumento3 pagine05 Forms of DrugsabdulNessuna valutazione finora
- Eksipien SignetDocumento94 pagineEksipien Signetnofha_90Nessuna valutazione finora
- PCT 211Documento380 paginePCT 211ezeudunicholas16Nessuna valutazione finora
- Cun Dell Objectionable Microorganism Sept 2015Documento36 pagineCun Dell Objectionable Microorganism Sept 2015KuldeepNessuna valutazione finora
- SAMPLE TRANS by @rehina - ADocumento3 pagineSAMPLE TRANS by @rehina - ANicole Anne Santiago SibuloNessuna valutazione finora
- Perioral DermatitisDocumento6 paginePerioral DermatitisYeni OktaviaNessuna valutazione finora
- Prinsipal Kode Produk Nama ProdukDocumento36 paginePrinsipal Kode Produk Nama ProdukLalu EyiqNessuna valutazione finora
- Transdermal Drug DeliveryDocumento37 pagineTransdermal Drug Deliveryabdullah2020Nessuna valutazione finora
- Assignment Spring 2020: Submitted ToDocumento11 pagineAssignment Spring 2020: Submitted ToFuad Hasan Pranto 1921147049Nessuna valutazione finora
- Products Without Methylisothiazolinone in US (Updated For 2014)Documento202 pagineProducts Without Methylisothiazolinone in US (Updated For 2014)danatodd75% (4)
- Healthsecure Pharma Mumbai. Product ListDocumento51 pagineHealthsecure Pharma Mumbai. Product Listsanjay_gawaliNessuna valutazione finora
- Indipharma Division Product ListDocumento6 pagineIndipharma Division Product ListGadamsetty MaheshNessuna valutazione finora
- ExplainingmedicationDocumento10 pagineExplainingmedicationHimatul AliyahNessuna valutazione finora
- Routes of Drug AdministrationDocumento39 pagineRoutes of Drug AdministrationAditya AdhikariNessuna valutazione finora
- PST 04104 Pharmaceutical Dosage Forms-Marking GuideDocumento20 paginePST 04104 Pharmaceutical Dosage Forms-Marking GuideambroceNessuna valutazione finora
- Chapter 5 Pharmaceutics Complete Notes by Noteskarts Acc To ER20Documento28 pagineChapter 5 Pharmaceutics Complete Notes by Noteskarts Acc To ER20Ayodele olumideNessuna valutazione finora
- c23 PDFDocumento15 paginec23 PDFAmit KochharNessuna valutazione finora
- Johnson & Johnson Inc. 88 Mcnabb Street Markham, On 29 July 2014 L3R 5L2 ©johnson & Johnson IncDocumento59 pagineJohnson & Johnson Inc. 88 Mcnabb Street Markham, On 29 July 2014 L3R 5L2 ©johnson & Johnson Incknight2huntNessuna valutazione finora
- Introduction To Pharmacology PDFDocumento11 pagineIntroduction To Pharmacology PDFSuraj PetkarNessuna valutazione finora
- Update Stok GSM 17 Oktober 2022Documento33 pagineUpdate Stok GSM 17 Oktober 2022Rezky Agung MedikaNessuna valutazione finora
- Pharmaceutical ExcipientsDocumento19 paginePharmaceutical ExcipientsTikaUlamNessuna valutazione finora
- Topical Antibiotics For Skin InfectionsDocumento4 pagineTopical Antibiotics For Skin InfectionsniklukNessuna valutazione finora
- Fundamentals of NddsDocumento26 pagineFundamentals of NddsPavan NagdevNessuna valutazione finora
- Update of FormularyDocumento72 pagineUpdate of FormularyGrace RamirezNessuna valutazione finora
- Cold Cream FormDocumento2 pagineCold Cream FormsskkaleNessuna valutazione finora
- SDS - Pine GelDocumento4 pagineSDS - Pine GelMohan KNessuna valutazione finora
- Dermatological PharmacologyDocumento53 pagineDermatological PharmacologyDesta BelachewNessuna valutazione finora
- Registered Medicine List 2014 FMHACADocumento162 pagineRegistered Medicine List 2014 FMHACASindy ElfasNessuna valutazione finora