CLINICAL AND SYSTEMATIC REVIEWS 519
CME
Discontinuing Long-Term PPI Therapy: Why, With
REVIEW
Whom, and How?
Laura Targownik, MD, MSHS, FRCPC1
Proton pump inhibitors (PPIs) are among the most widely used class of drugs prescribed over the long term in all
of clinical medicine with 8–10% of ambulatory adults have been prescribed a PPI in the past 30 days. However,
numerous studies have raised doubts about the long term safety of PPI use. The purpose of this review is threefold:
(i) To provide an overview of the current evidence demonstrating associations between PPI use and adverse health
outcomes and the likelihood of the associations being causal (Why?); (ii) To be able to identify long-term PPI users in
whom the intensity of PPI therapy could be reduced or in whom PPIs could be eliminated outright (Who?); and (iii) To
provide strategies on how to reduce or stop chronic PPI therapy while maintaining symptom control and reducing the
risk for symptom or upper GI disease recurrence (How?).
Am J Gastroenterol 2018; 113:519–528; doi:10.1038/ajg.2018.29; published online 20 March 2018
INTRODUCTION balancing of the risks and benefits of reducing or eliminating PPI
The introduction of proton pump inhibitors (PPIs) in the mid- use in an individual patient. Also, if the decision is made to dis-
1980s into the marketplace represented a major step forward in continue chronic PPI therapy, consideration needs to be given as
the management of acid-peptic-related disease. By irreversibly how this process should be undertaken. The purpose of this review
blocking the proton pump in the gastric oxyntic mucosa, PPIs is threefold:
irreversibly block active proton pumps in the gastric oxyntic
mucosa, resulting in a profound reduction in basal and stimu- 1. To provide an overview of the current evidence demonstrating
lated gastric acid output (1). As a result, the intragastric pH can associations between PPI use and adverse health outcomes and
be maintained at a sufficiently high level to allow for consistent the likelihood of the associations being causal (Why?).
healing and prevention of esophagitis and peptic ulcer disease, 2. To be able to identify long-term PPI users in whom the
and more rapid control of associated symptoms (2,3). PPIs are intensity of PPI therapy could be reduced or outright elimi-
also perceived to have a favorable side effect profile, and are often nated (Who?).
prescribed not only for established acid-related upper gastroin- 3. To provide strategies on how to reduce or stop chronic PPI
testinal (GI) disease but also empirically for nonspecific upper GI therapy while maintaining symptom control and reducing
symptoms (4–6). As a result, PPIs have become among the most the risk for symptom or upper GI disease recurrence (How?).
widely used class of drugs prescribed over the long term in all
of clinical medicine. It is estimated that 8–10% of ambulatory
adults have been prescribed a PPI in the past 30 days (7). PPI use WHY SHOULD WE BE CONCERNED ABOUT LONG-
is particularly prevalent in the elderly; people over the age of 60 TERM PPI USE?
years are 3.5 times more likely to be using PPIs than those under To date, published studies have reported association between
60 years (8). In 2009, over US$7 billion was spent on PPI pre- the long-term use of PPIs and over two dozen unique complica-
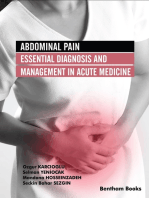
scriptions in the United States, and over US$13 billion was spent tions (13–24) (Figure 1). The specific details regarding the studies
worldwide (9) and this does not include money spent on over-the- reporting associations between PPI use and these conditions will
counter PPIs (10). not be described in detail in the article; the reader is directed to
However, numerous studies have raised doubts about the long- several excellent reviews of this topic ((25,26)).
term safety of PPI use (11,12). As a result, many practitioners are However, one key commonality of these studies demonstrating
looking for guidance of whether patients who have been using PPI-associated adverse events is that they are nearly all observa-
PPIs chronically should be curtailing their use. This decision is tional studies, with the majority of the most cited and noteworthy
dependent of the indications for PPI use, and an assessment and studies having been performed by retrospectively analyzing large
1
Section of Gastroenterology, Department of Internal Medicine, Max Rady School of Medicine at University of Manitoba, Winnipeg, Manitoba, Canada.
Correspondence: Laura Targownik, MD, MSHS, FRCPC, Section of Gastroenterology, Department of Internal Medicine, Max Rady School of Medicine at University
of Manitoba, 805G-715 McDermot Avenue, Winnipeg, Manitoba, Canada R3E 3P4. E-mail: laura.targownik@med.umanitoba.ca
© 2018 by the American College of Gastroenterology The American Journal of GASTROENTEROLOGY
520 Targownik
Stroke
Dementia
REVIEW
Lungs
(pneumonia) Heart
(MI)
Subacute cutaneous
lupus erythematosus
(SCLE)
Muscle
(rhabdomyolysis)
Liver
(hepatic
encephalopathy)
Blood
(anemia)
Stomach
(fundic gland polyps)
Spontaneous
bacterial peritonitis
(SBP)
Acute interstitial
nephritis (AIN)
ESRD/
chronic renal
insufficiency
Small bowel
(bacterial overgrowth) Colon (C difficile,
Salmonella,
Campylobacter
colitis)
Bone
(hip fracture/ Microscopic
osteoporosis) colitis
Figure 1. Adverse events associated with proton pump inhibitor use. Original: Complications of proton pump inhibitor therapy. Gastroenterology 2017
Jul;153(1):35–48. Used with permission of Michael Vaezi.
health-care utilization data sets which had been collected primar- assigned, and these non-random factors that lead to PPI use (or
ily for administrative purposes. In an observational study, the non-use) may individually impact on the probability of that per-
exposure status (i.e., PPI user vs. PPI non-user) is not randomly son developing the outcome of concern. This issue of confound-
The American Journal of GASTROENTEROLOGY VOLUME 113 | APRIL 2018 www.nature.com/ajg
Discontinuing Long-Term PPI Therapy 521
ing affects every observational trial, and it becomes impossible to cation, as is the case how we are comfortable stating that there is
definitely prove whether the PPI caused the outcome, or whether a causal association between cigarette smoking and lung cancer
the factors that led to PPI use caused the outcome. While statisti- even though there has never been a study where persons at risk
REVIEW
cal tools such as multivariable regression and propensity weighting for lung cancer were randomized to cigarette use or matching pla-
can be used to mitigate against the effects of confounding, there cebos (27).
will invariably remain some degree of residual confounding due to The Bradford Hill Criteria (Table 1) were conceived to provide
the presence of unmeasured differences in the exposed and non- a framework for determining the likelihood of causality where an
exposed groups. association between an exposure and outcome is detected (28).
To unequivocally prove that PPIs are directly responsible for While Hill originally proposed nine criteria for assessing the likeli-
any of the hypothesized complications, a randomized controlled hood of causality, the areas where there is universal agreement as
trial must be performed. However, it is exceedingly unlikely at this to their importance are those of strength of association, biologic
time that a randomized controlled trial will be undertaken that is plausibility, consistency, and temporality
sufficiently powered and of a sufficiently long duration to detect
a clinically and statistically significant increase in the incidence Strength of association
of these complications between PPI users and non-users. How- The greater the magnitude detected association between an expo-
ever, a causal relationship can potentially be presumed if there are sure and an outcome, the more likely that relationship is to be
other evidentiary pathways linking PPI use to a specific compli- causal and clinically relevant Strong associations that remain
between an exposure and outcome after adjusting for known con-
founders are less likely to due to the effect of residual unmeas-
ured confounders, and thus more likely to be real. Unmeasured
Table 1. Bradford Hill Criteria confounders are those factors that are associated with both PPI
use and the adverse event under study, but are either impossible
Criterion
to assess or difficult to measure accurately. As an example, global
Strength of Association Larger effect sizes are less likely to be due to frailty increases the risk of hip fractures and is associated with
chance or confounding degenerative diseases and senescence; people who are frail are
Biologic Plausibility Evidence for a plausible physiologic mechanism also more likely to be prescribed PPIs (29,30). While as clinicians
should exist, or be thought possible we may subjectively recognize when a patient is frail, it is difficult
Temporality The exposure must occur prior to the event to quantify precisely, and is therefore not generally reported in the
Consistency Results across studies in similar populations data sets in which these studies are performed.
should be similar This issue is distinct from that of statistical significance, which
Biologic Gradient Strength of Association should correlate with can be attained for small magnitude effects if the sample size of
exposure intensity the population under study if sufficiently large. This is particularly
Coherence Presence of association does not directly con- relevant given the epidemiologic studies reporting PPI-related
tradict pre-existing evidence complications are performed on data sets containing information
Analogy Similar exposures have been shown to be on thousands if not millions of people, meaning that highly sta-
cause similar disease processes tistically significant results can be reported for very small asso-
Specificity Other factors that would otherwise explain the ciations. Table 2 contains the reported effect sizes (odds ratios,
association are not present hazard, ratios, or risk ratios) of PPI exposure and the specific
Table 2. Most recent estimates of effect size for PPI-associated adverse events
Adverse event Effect size (95% CI) Reference Heterogeneity?
Enteral infection OR 2.55 (1.53–4.26) Leonard et al. (23) Yes
Community-acquired pneumonia OR 1.49 (1.16–1.92) Lambert et al. (36) Yes
Clostridium difficile-associated diarrhea OR 1.26 (1.12–1.29) Cao et al. (107) Yes
Hip fracture OR 1.26 (1.16–1.36) Zhou et al. (37) Yes
Dementia HR 1.44 (136–1.52) Gomm et al. (16) N/A
Vitamin B12 deficiency HR 1.83 (1.36–2.46) Jung et al. (108) Borderline
Chronic renal failure RR 1.36 (1.07–1.72) Nochaiwong et al. (109) Yes
Myocardial infarction OR 1.16 (1.09–1.24) Shah et al. (22) N/A
HR, hazard ratio; N/A, not applicable; OR, odds ratio; PPI, proton pump inhibitor; RR, relative risk.
© 2018 by the American College of Gastroenterology The American Journal of GASTROENTEROLOGY
522 Targownik
adverse events in the most recently published meta-analysis as non-published negative studies do not get included, biasing the
of September 2017, or of single studies where just one study has findings in favor of there being an effect when none exists.
been published. For all adverse events, the pooled adjusted effect
REVIEW
size is <2, and for many of the most frequently studied associa- Biologic plausibility
tions, the reported effect sizes are <1.5. This level of association, If PPIs do indeed directly cause any of the adverse events for
even if highly statistically significant, can be explained away by which PPI use is associated, then it must result from their physi-
the effects of unmeasured confounding, and do not let strong sup- ologic effects in the person using them. The physiologic effects of
port for causality. Conversely, clinicians should be cognizant that PPIs can be characterized into three categories: (1) effects result-
even small magnitude effects, if truly causal, can have enormous ing from decreased gastric acid output due to the direct effect of
impacts of population health if the exposure is highly prevalent, inhibition of proton pump-mediated gastric acid secretion; (2)
and the outcome is morbid, and not rare. As an example, if 15% inhibition of proton pumps found in other organ systems; (3)
of the geriatric population are chronic PPI users, and PPI use was effects due to alteration of drug metabolism, leading to changes in
directly responsible for 25% increase in the risk of hip fracture the concentration and activity of other drugs or metabolites that
among chronic users, then PPI use would lead to an additional affect bone metabolism.
45,000 hip fractures per year among people over age 65 years in
the United States (31) and would be responsible for 1,500 addi- (1) Effects resulting from reduction of gastric acid secretion:
tional deaths each year (32). Of these categories, the most well understood effect is that of
PPIs on blocking gastric acid output. The presence of gastric acid
Temporality is often considered to be a nuisance due to its role in the patho-
It is unimpeachably true that a patient must be exposed to a physiology of GERD and peptic ulcer disease. Further, although
putative risk factor before the occurrence of an adverse event gastric acid is needed to convert inactive pepsinogen into the
in order to be implicated in its cause. Essentially all studies that gastric protease pepsin, ingested proteins will still be completely
have studied PPI-related adverse events attempt to assess PPI digested in the absence of pepsin and gastric acid by pancreatic
exposure before the event of interest. However, the precise date proteases. Therefore, one might think that pharmacological in-
that a diagnosis of a putative complication occurs may not nec- hibition of gastric acid secretion would have minimal negative
essarily be the same as what is recorded in the study database. consequence.
This is particularly the case for diagnoses, which are progressive However, the fact that gastric acid production has been evo-
and degenerative like Alzheimer’s-type dementia or osteoporo- lutionary retained across nearly all vertebrates suggests that the
sis, or those with a long preclinical prodrome, which may have ability to generate gastric acid provides a survival advantage, at
an onset months to years before being clinically recognized (33). least until modern times (39). Most probably, the benefits of gas-
In more acutely occurring complications, early symptoms may tric acid pertain to its ability to stabilize the gut microbiota by
be misdiagnosed as similarly presenting conditions, as commu- preventing colonization with acid-sensitive organisms and path-
nity-acquired pneumonia may be initially misdiagnosed as an ogens; interestingly, carnivorous and scavenging animals, who
upper respiratory infection, congestive heart failure, or, if chest have a higher risk of exposure to pathogens, tend to have higher
pain is a predominant feature, gastroesophageal reflux disease levels of gastric acid production than do herbivores or grazers
(GERD) (34). If a PPI is dispensed during this prodromal period, (40). In humans, multiple studies have demonstrated that condi-
it may generate as association between PPI use and this adverse tions which lead to a reduction in gastric acid output (atrophic
outcome which appears to be temporal, but in fact violates gastritis, surgical gastrectomy) increase the risk of enteric infec-
this assumption. This phenomenon is commonly referred to as tions with acid-sensitive organisms such as Salmonella and
protopathic bias. Campylobacter (41).
PPI use has been strongly associated with an increased risk
Consistency of infection with C. difficile (35,42–44). However, ingested
In order for a result to be consistent, the results of the epidemio- C. difficile organisms are acid resistant, and therefore a reduc-
logic studies performed in different populations should fund tion in gastric acid itself should not result directly in an increased
associations between PPI use and adverse events of comparable likelihood of C. difficile infection (45). However, PPIs have also led
magnitude. Studies of the most widely evaluated PPI-associated to significant alterations of the gut microbiota (46), with decreases
adverse conditions (fracture, Clostridium difficile infection, com- in general biodiversity, increase in Firmicute phyla organisms,
munity acquired pneumonia) have demonstrated some degree of and a decrease in Bacteroides. These changes may create an envi-
heterogeneity, and also have not shown a consistent dose response ronment where C. difficile is more likely proliferate leading to
effect (35–37). In addition, as there is not currently a requirement symptomatic infection in people who are already colonized with
for preregistration of epidemiologic studies, it is very likely that C. difficile organisms (47).
studies which do not demonstrate an association between PPI In addition, gastric acid has a role in facilitating the absorption
use and an adverse event are not completed or published. Com- of iron, calcium, and vitamin B12. Of these, the effects of gastric
monly referred to as the “file-drawer effect ((38)),” this means that acid inhibition on calcium absorption are likely the most clini-
positive studies tend to be available for meta-analysis, and the cally relevant (48–50), given the important role that calcium has
The American Journal of GASTROENTEROLOGY VOLUME 113 | APRIL 2018 www.nature.com/ajg
Discontinuing Long-Term PPI Therapy 523
in bone homeostasis and in maintaining bone strength (51). While and it is not recommended to discontinue PPIs in persons who
calcium is more soluble in increasingly acidic solutions, the effects are already afflicted with any of the PPI-associated adverse events,
of PPI use on calcium absorption are negligible in most circum- nor should long-term PPI users receive specific treatment in an
REVIEW
stances (49,52,53). In addition, the majority of studies evaluating attempt to prevent any of the complications (12,64). As an exam-
the relationship between PPI use and bone mineral density have ple, it is not recommended that PPI users undergo screening for
not shown any effect of PPI use on bone strength or on the preva- osteoporosis or undergo a fracture risk assessment just because
lence of osteoporosis (54,55). Therefore, there is minimal biologic they are PPI users, and there is no contraindication against PPI
plausibility for PPIs to promote osteoporosis related fracture, at use among people with established osteoporosis or a history of hip
least as mediated by reduction in gastric acid secretion. fracture. However, one cannot prove that PPIs are entirely safe, and
the data sources that would be required to prove the safety of PPIs
(2) Effects from blockage of non-GI proton pumps: While PPIs pri- are lacking. Therefore, it remains important not to inappropriately
marily inhibit the action of the proton pumps found in the gas- use PPIs, and specifically, to limit their use to persons with condi-
tric oxyntic mucosa, vacuolar proton pumps that can be blocked tions where the benefits of PPI are well defined.
by PPIs are found elsewhere in the body, particularly in bone
osteoclasts and the distal tubules of the nephron (56,57). While
blockage of renal proton pumps in animal models may lead to de- WHO SHOULD REMAIN ON LONG-TERM PPI
creased renal acid secretion and cause a mild metabolic acidosis, THERAPY
it does not have any effect on glomerular function (58). Therefore, Definite indications for long-term PPI therapy
it is unlikely that this mechanism is responsible for the associa- Treatment of erosive esophagitis and prevention of relapse: Among
tion between PPIs and chronic renal insufficiency. In the case of persons with erosive esophagitis that completely healed on PPI
osteoclast-based proton pumps, inhibition should decrease bone therapy, the risk of endoscopic relapse is 72% for persons who
resorption, resulting in increased bone mineral density. stop using PPIs compared to 13% for those who continue PPI
therapy during this period (65). Furthermore, PPIs are more
(3) Other proposed mechanisms: In the studies that have linked effective than histamine-2 receptor antagonists (H2RAs) in main-
PPI use to Alzheimer’s disease, and chronic renal insufficiency taining symptom-free remission among person with healed ero-
(16,24), the investigators have suggested pathophysiologic path- sive esophagitis (91% PPI vs. 62% H2RA, P<0.001) (65). The risk
ways that are independent of their main pharmacologic action. As of relapse with PPI discontinuation is particularly high among
an example, the PPI lansoprazole has been shown to increase the persons with more severe forms of esophagitis. PPI discontinu-
synthesis of certain amyloid-β protein, which is also elaborated in ation could be considered among persons with milder forms of
persons with Alzheimer’s disease (59). However, the studies sup- erosive esophagitis (LA Class A/B), or in those persons where a
porting this and other mechanisms have not been demonstrated major factor that predisposed an individual to erosive esophagitis
in animal models or humans, and also have not be widely repli- (such as heavy alcohol use) has been eliminated.
cated. In these cases, the evidence for biologic plausibility is the Treatment of PPI-responsive esophageal eosinophilia (REE):
most tenuous. Approximately 50% of persons with apparent eosinophilic
In addition, PPIs are metabolized in the liver by enzymes in esophagitis will have a clinical and histologic response to PPI
the cytochrome P450 family; competitive inhibition of these therapy (66). These patients are referred to as having PPI-REE, or
cytochromes could interfere with the metabolism and/or clearance PPI-REE. Persons with PPI-REE have a high rate of symptomatic
of other drugs. The proposed mechanism for the apparent associa- and/or clinical relapse when effective therapy is discontinued.
tion between myocardial infarction and PPIs among clopidogrel Although the natural history of PPI-REE is not well defined, there
users was that PPIs would prevent cytochrome P450 metabolized is evidence that untreated or undertreated eosinophilic esophagitis
conversion of the prodrug form of clopidogrel into the active drug may eventually result in chronic stricture (67). In addition, the
(60). However, the clinical significance of this mechanism is doubt- long term risks associated with PPI use are likely less clinically
ful (61), given that prospective trials demonstrated no difference significant than those resulting from long-term corticosteroid use,
in adverse cardiovascular event rates between PPI users and non- the most commonly utilized medical therapy for EoE. Therefore,
users among persons who were exposed to clopidogrel (62,63). the long-term use of PPIs in persons with eosinophilic esophagitis
Overall, while correlations between chronic PPI use and a would seem to be reasonable.
diverse range of acute and chronic complications have been con- Prevention of peptic ulcer disease and its complications: PPIs are
sistently demonstrated, there is insufficient evidence supporting highly efficacious in preventing gastric and duodenal ulceration
a causal role for PPIs in the etiology of any of these conditions. in chronic users of nonsteroidal anti-inflammatory drugs (68,69).
The supporting evidence for infectious complications, specifically In epidemiologic studies, persons who used PPIs concomitantly
enteric infections, is the most compelling, whereas the evidence with nonsteroidal anti-inflammatory drug therapy reduce the
for extragastrointestinal complications whose pathophysiology odds of being hospitalized for complicated peptic ulcer disease
should not be influenced by reduced acid secretion is especially by between 50% and 80% (70–72). PPI-based gastroprotection is
weak. At this point, guidelines that do not suggest chronic PPI recommended for all chronic aspirin and/or nonsteroidal anti-
users should be screened for any of the PPI-associated disease, inflammatory drug users who have risk factors that increase the
© 2018 by the American College of Gastroenterology The American Journal of GASTROENTEROLOGY
524 Targownik
risk of peptic ulcer disease-related complications; these risk fac- disease and those with functional heartburn, who manifest reflux
tors include concomitant use of antiplatelet and/or anticoagulants, symptoms consistent with reflux but do not have physiologic evi-
concomitant use of systemic corticosteroids, age over 70 years, dence of reflux of acidic gastric contents in to the esophagus. PPIs
REVIEW
prior history of peptic ulcer disease, and the presence of severe are likely effective in the long term for the former, but they are less
medical comorbidities (71,73,74). likely to be efficacious in those whose symptoms are not due to
Prevention of progression of Barrett’s esophagus: Acid-induced esophageal acid exposure (87).
esophageal injury is a major etiologic factor in the development Symptoms presumed secondary to laryngopharyngeal reflux:
of intestinal metaplasia, and has been implicated in the progres- Laryngopharyngeal reflux (LPR) is often implicated in the etiol-
sion to dysplasia and neoplasia (75). There are conflicting reports ogy of chronic symptoms of laryngopharyngeal irritation such as
about the benefits of PPIs in the prevention of esophageal adeno- hoarse voice, sore throat, or globus sensation (88). Current ENT
carcinoma, although there is a trend towards their being protec- guidelines recommend PPI therapy for persons with laryngeal
tive (76–78). All major guidelines on the management of Barrett’s symptoms presumed secondary to LPR, often at high dose and for
esophagus strongly recommend PPI therapy, even in the absence durations of at least 3–6 months (89). However, the diagnosis of
of symptoms, to prevent progression of Barrett’s esophagus to dys- LPR is generally based on the finding of irritation of the posterior
plasia and esophageal adenocarcinoma (79,80) larynx and arytenoid cartilage on visual inspection, which poorly
Zollinger–Ellison Syndrome: Hypersecretion of gastric acid due differentiates between laryngitis and those due to other causes,
to the unregulated release of gastrin from a gastrinoma is the cardi- such as post-nasal drip or environmental allergens and irritants
nal feature of Zollinger–Ellison Syndrome. PPIs are the most effec- (90). Further, more accurate evaluations for physiologic reflux,
tive therapy for control of complications of gastric acid secretion such as pH monitoring or multichannel impedance are rarely done
(81–83) While removal of the gastrinomatous tissue may allow for (91). The evidence supporting PPIs for treatment of LPR is at best
discontinuation of PPIs, this is not possible for persons with meta- conflicted, with the most recently published meta-analyses dem-
static disease, or those with underlying multiple endocrine neopla- onstrating PPIs were no better than placebo in achieving symptom
sia type 1 (84). In these patients, long-term continuation of PPIs is improvement (defined as a 50% reduction in laryngeal symptoms
of unquestioned value. (PPIs 42% vs. placebo 39%, difference 4%, 95% CI: 6–14)), and also
were no different than placebo in improving the signs of presumed
Possible indications for long-term PPI therapy LPR on laryngoscopic examination (92).
There are a number of indications where though PPI use may
be effective in the short term, the benefits of continuing therapy Inappropriate PPI use
are not well described. In these scenarios, withdrawal of PPIs in Inappropriate PPI use can be defined as use which either occurs in
would be unlikely to be result in significant adverse events. For the absence of a known indication, or for use for a non-absolute
patients with these indications, n=1 trials of substitution of PPIs indication where a trial of PPI cessation has not been considered
with less potent anti-secretory therapies like H2RAs, pain modu- or attempted (93). All current guidelines recommend limiting
lating agents like tricyclic antidepressants or selective serotonin PPI use to specific indication, and to use the smallest dose for the
reuptake inhibitors, or outright discontinuation should be con- shortest duration required to adequately control symptoms. Even
sidered. in the absence of definitive evidence of medical harm associated
Functional dyspepsia: PPIs are frequently prescribed for patients with PPI use, the excess cost associated with unnecessary therapy
with dyspepsia, even if no ulcer is present. The most recent meta- should be enough reason to make attempts to curtail the inap-
analysis of studies comparing PPIs with placebo for functional dys- propriate PPI use.
pepsia showed response rates of 34% for PPIs and 25% for placebo In 2010, Heidelbaugh et al. (94) assessed PPI use and their
(risk ratio (RR) 0.88, 95% confidence interval (CI): 0.82–0.94) (85). indications in 946 patients in ambulatory care clinic, and found
However, the maximum duration of therapy evaluated is 8 weeks, that over one-third of PPI users did not have a documented indi-
and it is unclear whether this efficacy benefit is maintained over cation for ongoing use, and 10% were using for extraesophageal
time. As functional dyspepsia is a chronic condition with recur- indications. Furthermore, nearly one-half patients did not have
rent symptoms, persons with functional dyspepsia likely will use any documentation of the response to therapy having been re-
PPIs for longer periods of time, despite there being no evidence of evaluated at any point following PPI initiation. Patients without
continued benefit over the longer term. appropriate indications who were using PPIs, without an indica-
Endoscopy-negative reflux disease: Persons with reflux-like symp- tion, spent approximately US$1,500 per year on PPIs. Similarly,
toms but with no endoscopic evidence of erosive esophagitis who Ladd et al. (95) found that among 201 persons who were newly
are given PPIs have higher levels of symptom relief when com- prescribed PPIs on a in-patient medical ward, three-quarters
pared to placebo (RR 0.69, 95% CI: 0.65–0.78); H2RAs (RR 0.78, had either no documented indication or an inappropriate indi-
95% CI: 0.62–0.97) or prokinetics (RR 0.72, 95% CI: 0.56–0.92) cation for PPI, of whom 40% continued PPI therapy following
(86). However, there is no evidence for the benefit of PPI therapy discharge.
over the long-term among patients with endoscopy-negative reflux The factors that are driving the inappropriate initiation and/or
disease. Persons with endoscopy-negative reflux disease are a het- failure to address the need for ongoing PPI therapy have not been
erogeneous group, including those who have non-erosive reflux systematically evaluated, although a model characterizing patient
The American Journal of GASTROENTEROLOGY VOLUME 113 | APRIL 2018 www.nature.com/ajg
Discontinuing Long-Term PPI Therapy 525
and physician behaviors that drive inappropriate PPI therapy can a significantly lower rate of symptom control than did those
be envisioned. First, in primary care, PPIs are often initiated empir- maintained on regular PPI therapy (32% vs. 72%, P<0.0001)
ically for GI symptoms, as opposed to being used for an objectively (98). While these findings seem to favor continuing therapy as
REVIEW
diagnosed condition, and there it is difficult if not impossible to opposed to stepping down, the majority of persons who were
differentiate based on symptoms alone whether someone with decreased to on-demand therapy continued to report adequate
pyrosis has functional heartburn vs. erosive esophagitis, or func- symptom relief, as did a meaningfully large minority of those
tional dyspepsia vs. peptic ulcer disease. Second, PPIs will lead to given H2RAs.
complete healing of the active ulceration in persons with peptic Inadomi et al. (99) prospectively demonstrated that 80% of per-
ulcer disease or erosive esophagitis, rendering it impossible to sons with controlled symptoms of GERD on higher-than-standard
determine whether the original symptoms arose from an organic doses of PPIs could be stepped down to standard dose PPIs with-
disease or a functional one. Third, PPI therapy in many instances out developing significant recurrent symptoms. Aside from the
is initiated following endoscopy, or during an in-patient stay, by a exceedingly rare Zollinger–Ellison syndrome, there are no clinical
physician who does not maintain an ongoing relationship with the scenarios that absolutely necessitate the use of higher-than-stand-
patient. In these situations, the primary care physician may not be ard doses of PPIs. Therefore, dose reduction strategies should be
certain as to whether PPI discontinuation is reasonable and safe. considered for all persons who are using PPIs chronically at high
Fourth, most upper GI symptoms arising from a functional syn- doses.
drome wax and wane in intensity, and patients are more likely to
seek health care and remedies when symptoms are at their worst. Total discontinuation of PPIs
The symptoms for which PPIs are then prescribed would have In persons without a clear indication for PPI therapy, or in those
a high chance of having improved, even if the PPI had not been persons who were treated empirically for upper GI symptoms, a
used due to regression to the mean. Last, the absence of highly trial of discontinuation can be attempted. Not surprisingly, per-
effective competing drug options for upper GI symptomatology sons with mild esophagitis who initially responded to PPI therapy
compels prescribers to favor PPIs over other options. This model who were given placebo had a relapse rate between 48 and 100%
provides an important framework for health-care prescribers and over the next 6 months, compared with 17–33%% for those who
symptoms who want to engage with reducing the burden of inap- continued on standard dose PPI (100).
propriate PPI use For patients who are taking PPIs for unclear indications, or for
symptoms where there is little evidence for PPI use, common sense
would dictate that they should be discontinued without the expec-
HOW SHOULD PPI THERAPY BE DEPRESCRIBED tation of adverse consequences. However, the sudden discontinu-
PPI deprescribing refers to a patient or physician effort to either ation of PPIs may cause a sudden and profound rise in gastric acid
discontinue PPIs outright, decrease exposure to PPIs by stepping output, a phenomenon known as rebound gastric acid hypersecre-
down to a lower dose or intermittent/on-demand treatment regi- tion. The regular use of PPI raises intragastric pH; at high pH lev-
men, or substituting PPIs with a less costly and/or less potent form els, the secretion of the trophic hormone gastrin is not negatively
of gastric acid inhibition. An attempt at PPI deprescription should inhibited, predisposing to the development of hypergastrinemia
be considered for all PPI users who do not have definite indica- that in turn stimulates oxyntic cell proliferation and an increased
tions for long-term therapy (severe erosive esophagitis, high risk capacity to generate gastric acid (101). So long as the PPI is being
for aspirin/nonsteroidal anti-inflammatory drug-related compli- taken, this increased capacity for gastric acid generation is kept
cations, and Barrett’s esophagus), with the goal of therapy being to in check. However, if PPI therapy is abruptly discontinued, large
use the lowest dose of PPI necessary to control acid-related symp- amounts of gastric acid may be generated, which can theoretically
toms and/or mucosa damage. aggravate upper GI symptoms (102).
In a study assessing the clinical significance of this physiologic
Effectiveness of step-down regimens phenomenon, Reimer et al. (103) took persons with no history
On-demand therapy, where a patient uses PPIs only when of GERD or dyspepsia and gave them all PPIs continuously for 8
symptoms occur and taken until symptoms are adequately weeks. At the eighth week mark, these persons were randomized
relieved, is significantly more effective than placebo in providing to either placebo or continuing the PPI for an additional 4 weeks;
adequate symptom relief (51% vs. 14%, P<0.0001) (96). A meta- 40% of persons who discontinued the PPI reported dyspepsia in
analysis that included randomized controlled trials comparing the 4 weeks following discontinuation. In a similarly designed
continuing PPI use to on-demand PPI use or in persons with study, Niklasson et al. (104) found that symptoms on PPI with-
mild treatment-responsive GERD symptoms found that per- drawal were significantly correlated with the degree of PPI-induced
sons assigned to on-demand therapy has a significant increase hypergastrinemia. In a follow-up study where 78 PPI users not
in the risk of loss of symptom control (16% vs. 10%, RR 1.71, having a documented indication were discontinued, nearly two-
95% CI: 1.31–2.21), while decreasing weekly pill intake by nearly thirds (51/78) developed upper GI symptoms within 6 months.
3.8 PPI doses per week (97). In a primary care-based Norwegian People who developed upper GI symptoms subsequently under-
study of 2156 patients who had PPI-responsive GERD, persons went endoscopy, where 40% had endoscopic findings consistent
randomized to receive ongoing management with H2RAs had with their symptoms, mostly mild esophagitis (105).
© 2018 by the American College of Gastroenterology The American Journal of GASTROENTEROLOGY
526 Targownik
One strategy to mitigate against rebound acid hypersecretion- 3. Li Y, Sha W, Nie Y et al. Effect of intragastric pH on control of peptic ulcer
related symptoms would be to taper off PPI use, as opposed to bleeding. J Gastroenterol Hepatol 2000;15:148–54.
4. Austin PC, Stuart EA. Moving towards best practice when using inverse
sudden discontinuation. In a study by Inadomi et al. (106) where probability of treatment weighting (IPTW) using the propensity score
REVIEW
PPI users were discontinued gradually (1/2 of a standard dose to estimate causal treatment effects in observational studies. Stat Med
for 2 weeks, then discontinuing), 60% were asymptomatic on no 2015;34:3661–79.
5. Meineche-Schmidt V. Empiric treatment with high and standard dose of
medications or over-the-counter antacids in the year following. omeprazole in general practice: two-week randomized placebo-controlled
Whether a more prolonged taper leads to fewer rebound symp- trial and 12-month follow-up of health-care consumption. Am J Gastro-
toms is not known, but could be considered for those who develop enterol 2004;99:1050–8.
6. Rabeneck L, Souchek J, Wristers K et al. A double blind, randomized,
rebound symptoms with a more rapid taper. In my practice, I will placebo-controlled trial of proton pump inhibitor therapy in patients with
advise persons who wish to discontinue PPIs to take them every uninvestigated dyspepsia. Am J Gastroenterol 2002;97:3045–51.
other day for 2 weeks, twice per week for 2 weeks, and then to 7. Rotman SR, Bishop TF. Proton pump inhibitor use in the U.S. ambulatory
setting, 2002–2009. PLoS ONE 2013;8:e56060.
discontinue. I also advise patients who discontinue PPIs to be 8. Pottegard A, Broe A, Hallas J et al. Use of proton-pump inhibitors among
mindful of rebound symptoms, and not to immediately reintro- adults: a Danish nationwide drug utilization study. Ther Adv Gastroen-
duce PPIs at the first sign of recurrent symptoms, especially if they terol 2016;9:671–8.
9. Katz MH. Failing the acid test: benefits of proton pump inhibitors may
occur in the first week after stopping therapy. not justify the risks for many users. Arch Intern Med 2010;170:747–8.
10. Shaikh M, Dutta Choudhury S, Mohanty J et al. Modulation of excited-
state proton transfer of 2-(2'-hydroxyphenyl)benzimidazole in a macro-
cyclic cucurbit[7]uril host cavity: dual emission behavior and pK(a) shift.
SUMMARY Chemistry 2009;15:12362–70.
While there is not yet definitive evidence of serious harm associated 11. Chen J, Yuan YC, Leontiadis GI et al. Recent safety concerns with proton
with PPI use, it remains possible that further studies will be more pump inhibitors. J Clin Gastroenterol 2012;46:93–114.
12. Gill JM, Player MS, Metz DC. Balancing the risks and benefits of proton
strongly suggestive of a causal relationship, especially for those associ- pump inhibitors. Ann Fam Med 2011;9:200–2.
ations where biologic plausibility exists. Given the current uncertainty, 13. Lam JR, Schneider JL, Zhao W et al. Proton pump inhibitor and histamine 2
it behooves the clinician to limit the use of long-term PPIs to those receptor antagonist use and vitamin B12 deficiency. JAMA 2013;310:2435–42.
14. Bajaj JS, Zadvornova Y, Heuman DM et al. Association of proton pump
with definite indications, and to actively identify and make attempts to inhibitor therapy with spontaneous bacterial peritonitis in cirrhotic
deprescribe PPIs in persons without absolute indications for contin- patients with ascites. Am J Gastroenterol 2009;104:1130–4.
ued use, or those in whom a reason for ongoing use cannot be deter- 15. Xie Y, Bowe B, Li T et al. Risk of death among users of proton pump
inhibitors: a longitudinal observational cohort study of United States
mined. When discontinuing PPIs, consideration should be given to veterans. BMJ Open 2017;7:e015735.
step-down strategies, such as using H2RAs, or tapering the dose of 16. Gomm W, von Holt K, Thome F et al. Association of proton pump
PPIs over time. Further, chronic PPI users should be cautioned that inhibitors with risk of dementia: a pharmacoepidemiological claims data
analysis. JAMA Neurol 2016;73:410–6.
upper GI symptoms may recur in the short term, and that the occur- 17. Laheij RJ, Sturkenboom MC, Hassing RJ et al. Risk of community-
rence of these symptoms do not necessarily indicate a need for long- acquired pneumonia and use of gastric acid-suppressive drugs. JAMA
term PPIs, but rather may be a sign of transient reversible gastric acid 2004;292:1955–60.
18. Yang YX, Lewis JD, Epstein S et al. Long-term proton pump inhibitor
hypersecretion. Last, health-care systems should aim to develop and therapy and risk of hip fracture. JAMA 2006;296:2947–53.
evaluate programs to assist and guide physicians and patients through 19. Targownik LE, Lix LM, Metge CJ et al. Use of proton pump inhibitors and
the deprescribing process with the goal of eliminating unnecessary risk of osteoporosis-related fractures. CMAJ 2008;179:319–26.
20. Dial S, Delaney JA, Barkun AN et al. Use of gastric acid-suppressive
PPI use, and reduce superfluous health-care expenditures agents and the risk of community-acquired Clostridium difficile-associated
disease. JAMA 2005;294:2989–95.
CONFLICT OF INTEREST 21. Juurlink DN, Gomes T, Ko DT et al. A population-based study of the
drug interaction between proton pump inhibitors and clopidogrel. CMAJ
Guarantor of the article: Laura Targownik, MD, MSHS, FRCPC. 2009;180:713–8.
Specific author contributions: All aspects of creation of this article 22. Shah NH, LePendu P, Bauer-Mehren A et al. Proton pump inhibitor usage
were undertaken by Laura Targownik without assistance from other and the risk of myocardial infarction in the general population. PLoS
ONE 2015;10:e0124653.
individuals 23. Leonard J, Marshall JK, Moayyedi P. Systematic review of the risk of
Financial support: No external financial support. enteric infection in patients taking acid suppression. Am J Gastroenterol
Potential competing interests: Laura Targownik has received sup- 2007;102:2047–56.quiz 2057
24. Klatte DCF, Gasparini A, Xu H et al. Association between proton pump
port for research studies from Janssen Canada and Abbvie Canada. inhibitor use and risk of progression of chronic kidney disease. Gastro-
In the past 24 months, she has served on advisory boards for Janssen enterology 2017;153:702–10.
Canada, Takeda Canada, Merck Canada, Pfizer Canada, Ferring 25. Vaezi MF, Yang YX, Howden CW. Complications of proton pump inhibi-
tor therapy. Gastroenterology 2017;153:35–48
Canada, and Mallinckrodt. She has served on the Speaker’s Panel for 26. Johnson DA, Oldfield EC. Reported side effects and complications of
Takeda Canada and Janssen Canada long-term proton pump inhibitor use: dissecting the evidence. Clin
Gastroenterol Hepatol 2013;11:458–64.quiz e37–8
27. Doll R. Smoking and carcinoma of the lung. Acta Unio Int Contra
Cancrum 1953;9:495–506
REFERENCES 28. Hill AB. The environment and disease: association or causation? Proc R
1. Wolfe MM, Soll AH. The physiology of gastric acid secretion. N Engl J Soc Med 1965;58:295–300
Med 1988;319:1707–15. 29. Woods NF, LaCroix AZ, Gray SL et al. Frailty: emergence and conse-
2. Hunt RH, Cederberg C, Dent J et al. Optimizing acid suppression for quences in women aged 65 and older in the Women's Health Initiative
treatment of acid-related diseases. Dig Dis Sci 1995;40:24S–49S. Observational Study. J Am Geriatr Soc 2005;53:1321–30.
The American Journal of GASTROENTEROLOGY VOLUME 113 | APRIL 2018 www.nature.com/ajg
Discontinuing Long-Term PPI Therapy 527
30. Teramura-Gronblad M, Hosia-Randell H, Muurinen S et al. Use of 56. Valles P, Lapointe MS, Wysocki J et al. Kidney vacuolar H+-ATPase:
proton-pump inhibitors and their associated risks among frail elderly physiology and regulation. Semin Nephrol 2006;26:361–74.
nursing home residents. Scand J Prim Health Care 2010;28:154–9. 57. Tuukkanen J, Vaananen HK. Omeprazole, a specific inhibitor of H+-K+-
31. Brauer CA, Coca-Perraillon M, Cutler DM et al. Incidence and mortality ATPase, inhibits bone resorption in vitro. Calcif Tissue Int 1986;38:
of hip fractures in the United States. JAMA 2009;302:1573–9. 123–5.
REVIEW
32. Haentjens P, Magaziner J, Colon-Emeric CS et al. Meta-analysis: excess 58. Yang Q, Li G, Singh SK et al. Vacuolar H+-ATPase B1 subunit mutations
mortality after hip fracture among older women and men. Ann Intern that cause inherited distal renal tubular acidosis affect proton pump as-
Med 2010;152:380–90. sembly and trafficking in inner medullary collecting duct cells. J Am Soc
33. Dubois B, Padovani A, Scheltens P et al. Timely diagnosis for Alzheimer’s Nephrol 2006;17:1858–66.
disease: a literature review on benefits and challenges. J Alzheimers Dis 59. Badiola N, Alcalde V, Pujol A et al. The proton-pump inhibitor lansopra-
2016;49:617–31. zole enhances amyloid beta production. PLoS ONE 2013;8:e58837.
34. Filion KB, Chateau D, Targownik LE et al. Proton pump inhibitors and 60. Gilard M, Arnaud B, Cornily JC et al. Influence of omeprazole on the
the risk of hospitalisation for community-acquired pneumonia: replicated antiplatelet action of clopidogrel associated with aspirin: the randomized,
cohort studies with meta-analysis. Gut 2014;63:552–8. double-blind OCLA (Omeprazole CLopidogrel Aspirin) study. J Am Coll
35. Tariq R, Singh S, Gupta A et al. Association of gastric acid suppression Cardiol 2008;51:256–60.
with recurrent Clostridium difficile infection: a systematic review and 61. Bundhun PK, Teeluck AR, Bhurtu A et al. Is the concomitant use of clopi-
meta-analysis. JAMA Intern Med 2017;177:784–91. dogrel and proton pump inhibitors still associated with increased adverse
36. Lambert AA, Lam JO, Paik JJ et al. Risk of community-acquired pneumo- cardiovascular outcomes following coronary angioplasty?: a systematic
nia with outpatient proton-pump inhibitor therapy: a systematic review review and meta-analysis of recently published studies (2012–2016). BMC
and meta-analysis. PLoS ONE 2015;10:e0128004. Cardiovasc Disord 2017;17:3.
37. Zhou B, Huang Y, Li H et al. Proton-pump inhibitors and risk of fractures: 62. Douglas I, Evans S, Hingorani A et al. Clopidogrel and the interaction
an update meta-analysis. Osteoporos Int 2016;27:339–47. with proton pump inhibitors: a comparison between cohort and within
38. Duyx B, Urlings MJE, Swaen GMH et al. Scientific citations favor posi- person study designs. BMJ 2012;345:e4388.
tive results: a systematic review and meta-analysis. J Clin Epidemiol 63. O'Donoghue ML, Braunwald E, Antman EM et al. Pharmacodynamic
2017;88:92–101. effect and clinical efficacy of clopidogrel and prasugrel with or without
39. Koelz HR. Gastric acid in vertebrates. Scand J Gastroenterol Suppl a proton-pump inhibitor: an analysis of two randomised trials. Lancet
1992;193:2–6. 2009;374:989–97.
40. Beasley DE, Koltz AM, Lambert JE et al. The evolution of stom- 64. Freedberg DE, Kim LS, Yang YX. The risks and benefits of long-term
ach acidity and its relevance to the human microbiome. PLoS ONE use of proton pump inhibitors: expert review and best practice advice
2015;10:e0134116. from the american gastroenterological association. Gastroenterology
41. Giannella RA, Broitman SA, Zamcheck N. Influence of gastric acidity on 2017;152:706–15.
bacterial and parasitic enteric infections. A perspective. Ann Intern Med 65. Caro JJ, Salas M, Ward A. Healing and relapse rates in gastroesophageal
1973;78:271–6. reflux disease treated with the newer proton-pump inhibitors lanso-
42. Seto CT, Jeraldo P, Orenstein R et al. Prolonged use of a proton pump prazole, rabeprazole, and pantoprazole compared with omeprazole,
inhibitor reduces microbial diversity: implications for Clostridium difficile ranitidine, and placebo: evidence from randomized clinical trials. Clin
susceptibility. Microbiome 2014;2:42. Ther 2001;23:998–1017.
43. Freedberg DE, Salmasian H, Friedman C et al. Proton pump inhibitors 66. Molina-Infante J, Ferrando-Lamana L, Ripoll C et al. Esophageal eosino-
and risk for recurrent Clostridium difficile infection among inpatients. Am philic infiltration responds to proton pump inhibition in most adults. Clin
J Gastroenterol 2013;108:1794–801. Gastroenterol Hepatol 2011;9:110–7.
44. Tleyjeh IM, Bin Abdulhak AA, Riaz M et al. Association between proton 67. Schoepfer AM, Safroneeva E, Bussmann C et al. Delay in diagnosis of
pump inhibitor therapy and clostridium difficile infection: a contempo- eosinophilic esophagitis increases risk for stricture formation in a time-
rary systematic review and meta-analysis. PLoS ONE 2012;7:e50836. dependent manner. Gastroenterology 2013;145:1230–6 e1-2.
45. Wilson KH, Sheagren JN, Freter R. Population dynamics of ingested 68. Hawkey CJ, Karrasch JA, Szczepanski L et al. Omeprazole compared
Clostridium difficile in the gastrointestinal tract of the Syrian hamster. J with misoprostol for ulcers associated with nonsteroidal antiinflamma-
Infect Dis 1985;151:355–61. tory drugs. Omeprazole versus Misoprostol for NSAID-induced
46. Freedberg DE, Toussaint NC, Chen SP et al. Proton pump inhibitors alter Ulcer Management (OMNIUM) Study Group. N Engl J Med 1998;338:
specific taxa in the human gastrointestinal microbiome: a crossover trial. 727–34.
Gastroenterology 2015;149:883–885 e9. 69. Yeomans ND, Tulassay Z, Juhasz L et al. A comparison of omeprazole
47. Seekatz AM, Young VB. Clostridium difficile and the microbiota. J Clin with ranitidine for ulcers associated with nonsteroidal antiinflammatory
Invest 2014;124:4182–9. drugs. Acid Suppression Trial: Ranitidine versus Omeprazole for NSAID-
48. Recker RR. Calcium absorption and achlorhydria. N Engl J Med associated Ulcer Treatment (ASTRONAUT) Study Group. N Engl J Med
1985;313:70–3. 1998;338:719–26.
49. O'Connell MB, Madden DM, Murray AM et al. Effects of proton pump 70. Targownik LE, Metge CJ, Leung S et al. The relative efficacies of gastro-
inhibitors on calcium carbonate absorption in women: a randomized protective strategies in chronic users of nonsteroidal anti-inflammatory
crossover trial. Am J Med 2005;118:778–81. drugs. Gastroenterology 2008;134:937–44.
50. Bo-Linn GW, Davis GR, Buddrus DJ et al. An evaluation of the impor- 71. Andrade C, Sandarsh S, Chethan KB et al. Serotonin reuptake inhibi-
tance of gastric acid secretion in the absorption of dietary calcium. J Clin tor antidepressants and abnormal bleeding: a review for clinicians and a
Invest 1984;73:640–7. reconsideration of mechanisms. J Clin Psychiatry 2010;71:1565–75.
51. Ensrud KE, Duong T, Cauley JA et al. Low fractional calcium absorption 72. Lanas A, Garcia-Rodriguez LA, Arroyo MT et al. Risk of upper gastro-
increases the risk for hip fracture in women with low calcium intake. intestinal ulcer bleeding associated with selective cyclo-oxygenase-2
Study of Osteoporotic Fractures Research Group. Ann Intern Med inhibitors, traditional non-aspirin non-steroidal anti-inflammatory drugs,
2000;132:345–53. aspirin and combinations. Gut 2006;55:1731–8.
52. Wright MJ, Sullivan RR, Gaffney-Stomberg E et al. Inhibiting gastric acid 73. Lanza FL, Chan FK, Quigley EM. Guidelines for prevention of NSAID-
production does not affect intestinal calcium absorption in young, healthy related ulcer complications. Am J Gastroenterol 2009;104:728–38.
individuals: a randomized, crossover, controlled clinical trial. J Bone 74. Rostom A, Moayyedi P, Hunt R. Canadian consensus guidelines on
Miner Res 2010;25:2205–11. long-term nonsteroidal anti-inflammatory drug therapy and the need
53. Hansen KE, Jones AN, Lindstrom MJ et al. Do proton pump inhibitors for gastroprotection: benefits versus risks. Aliment Pharmacol Ther
decrease calcium absorption? J Bone Miner Res 2010;25:2510–9. 2009;29:481–96.
54. Fraser LA, Leslie WD, Targownik LE et al. The effect of proton pump 75. Ouatu-Lascar R, Fitzgerald RC, Triadafilopoulos G. Differentiation and
inhibitors on fracture risk: report from the Canadian Multicenter Osteo- proliferation in Barrett's esophagus and the effects of acid suppression.
porosis Study. Osteoporos Int 2013;24:1161–8. Gastroenterology 1999;117:327–35.
55. Targownik LE, Lix LM, Leung S et al. proton pump inhibitor use is not 76. Hu Q, Sun TT, Hong J et al. Proton pump inhibitors do not reduce the
associated with osteoporosis or accelerated bone mineral density loss. risk of esophageal adenocarcinoma in patients with Barrett's esophagus: a
Gastroenterology 2009;138:896–904 systematic review and meta-analysis. PLoS ONE 2017;12:e0169691.
© 2018 by the American College of Gastroenterology The American Journal of GASTROENTEROLOGY
528 Targownik
77. Masclee GM, Coloma PM, Spaander MC et al. NSAIDs, statins, low-dose 94. Heidelbaugh JJ, Goldberg KL, Inadomi JM. Magnitude and economic
aspirin and PPIs, and the risk of oesophageal adenocarcinoma among pa- effect of overuse of antisecretory therapy in the ambulatory care setting.
tients with Barrett's oesophagus: a population-based case–control study. Am J Manag Care 2010;16:e228–e234.
BMJ Open 2015;5:e006640. 95. Ladd AM, Panagopoulos G, Cohen J et al. Potential costs of inappropriate
78. Singh S, Garg SK, Singh PP et al. Acid-suppressive medications and risk use of proton pump inhibitors. Am J Med Sci 2014;347:446–51.
REVIEW
of oesophageal adenocarcinoma in patients with Barrett's oesophagus: a 96. Talley NJ, Lauritsen K, Tunturi-Hihnala H et al. Esomeprazole 20 mg
systematic review and meta-analysis. Gut 2014;63:1229–37. maintains symptom control in endoscopy-negative gastro-oesophageal
79. Shaheen NJ, Falk GW, Iyer PG et al. ACG Clinical Guideline: diag- reflux disease: a controlled trial of “on-demand” therapy for 6 months.
nosis and management of Barrett's esophagus. Am J Gastroenterol Aliment Pharmacol Ther 2001;15:347–54.
2016;111:30–50quiz 51 97. Boghossian TA, Rashid FJ, Thompson W et al. Deprescribing versus
80. Spechler SJ, Sharma P, Souza RF et al. American Gastroenterological continuation of chronic proton pump inhibitor use in adults. Cochrane
Association medical position statement on the management of Barrett’s Database Syst Rev 2017;3:CD011969.
esophagus. Gastroenterology 2011;140:1084–91. 98. Hansen AN, Wahlqvist P, Jorgensen E et al. Six-month management of
81. Metz DC, Comer GM, Soffer E et al. Three-year oral pantoprazole admin- patients following treatment for gastroesophageal reflux disease symp-
istration is effective for patients with Zollinger–Ellison syndrome and toms—a Norwegian randomized, prospective study comparing the costs
other hypersecretory conditions. Aliment Pharmacol Ther 2006;23: and effectiveness of esomeprazole and ranitidine treatment strategies in a
437–44. general medical practitioners setting. Int J Clin Pract 2005;59:655–64.
82. Maton PN, Vinayek R, Frucht H et al. Long-term efficacy and safety of 99. Inadomi JM, McIntyre L, Bernard L et al. Step-down from multiple- to
omeprazole in patients with Zollinger–Ellison syndrome: a prospective single-dose proton pump inhibitors (PPIs): a prospective study of patients
study. Gastroenterology 1989;97:827–36. with heartburn or acid regurgitation completely relieved with PPIs. Am J
83. Hirschowitz BI, Mohnen J, Shaw S. Long-term treatment with lansopra- Gastroenterol 2003;98:1940–4.
zole for patients with Zollinger–Ellison syndrome. Aliment Pharmacol 100. Armstrong D. Systematic review: persistence and severity in gastro-oe-
Ther 1996;10:507–22. sophageal reflux disease. Aliment Pharmacol Ther 2008;28:841–53.
84. Weber HC, Venzon DJ, Lin JT et al. Determinants of metastatic rate and 101. Waldum HL, Arnestad JS, Brenna E et al. Marked increase in gastric acid
survival in patients with Zollinger-Ellison syndrome: a prospective long- secretory capacity after omeprazole treatment. Gut 1996;39:649–53.
term study. Gastroenterology 1995;108:1637–49. 102. Fossmark R, Johnsen G, Johanessen E et al. Rebound acid hypersecretion
85. Pinto-Sanchez MI, Yuan Y, Bercik P et al. Proton pump inhibitors for after long-term inhibition of gastric acid secretion. Aliment Pharmacol
functional dyspepsia. Cochrane Database Syst Rev 2017;3:CD011194. Ther 2005;21:149–54.
86. Sigterman KE, van Pinxteren B, Bonis PA et al. Short-term treatment 103. Reimer C, Sondergaard B, Hilsted L et al. Proton-pump inhibitor therapy
with proton pump inhibitors, H2-receptor antagonists and prokinetics for induces acid-related symptoms in healthy volunteers after withdrawal of
gastro-oesophageal reflux disease-like symptoms and endoscopy negative therapy. Gastroenterology 2009;137:80–7.87 e1
reflux disease. Cochrane Database Syst Rev 2013;(5):CD002095. 104. Niklasson A, Lindstrom L, Simren M et al. Dyspeptic symptom develop-
87. Sifrim D, Zerbib F. Diagnosis and management of patients with reflux ment after discontinuation of a proton pump inhibitor: a double-blind
symptoms refractory to proton pump inhibitors. Gut 2012;61:1340–54. placebo-controlled trial. Am J Gastroenterol 2010;105:1531–7.
88. Vaezi MF. Laryngeal manifestations of gastroesophageal reflux disease. 105. Reimer C, Bytzer P. Discontinuation of long-term proton pump inhibi-
Curr Gastroenterol Rep 2008;10:271–7. tor therapy in primary care patients: a randomized placebo-controlled
89. Ford CN. Evaluation and management of laryngopharyngeal reflux. trial in patients with symptom relapse. Eur J Gastroenterol Hepatol
JAMA 2005;294:1534–40. 2010;22:1182–8.
90. Qadeer MA, Swoger J, Milstein C et al. Correlation between symptoms and 106. Inadomi JM, Jamal R, Murata GH et al. Step-down management of gas-
laryngeal signs in laryngopharyngeal reflux. Laryngoscope 2005;115:1947–52. troesophageal reflux disease. Gastroenterology 2001;121:1095–100.
91. Friedman M, Maley A, Kelley K et al. Impact of pH monitoring on 107. Cao F, Chen C, Wang M et al. An updated meta-analysis of controlled
laryngopharyngeal reflux treatment: improved compliance and symptom observational studies: proton-pump inhibitors and risk of Clostridium
resolution. Otolaryngol Head Neck Surg 2011;144:558–62. difficile infection. J Hosp Infect 2017;98:4–13.
92. Wei C. A meta-analysis for the role of proton pump inhibitor therapy 108. Jung SB, Nagaraja V, Kapur A et al. Association between vitamin B12
in patients with laryngopharyngeal reflux. Eur Arch Otorhinolaryngol deficiency and long-term use of acid-lowering agents: a systematic review
2016;273:3795–801. and meta-analysis. Intern Med J 2015;45:409–16.
93. Heidelbaugh JJ, Kim AH, Chang R et al. Overutilization of proton-pump 109. Nochaiwong S, Ruengorn C, Awiphan R et al. The association between
inhibitors: what the clinician needs to know. Ther Adv Gastroenterol proton pump inhibitor use and the risk of adverse kidney outcomes: a sys-
2012;5:219–32. tematic review and meta-analysis. Nephrol Dial Transplant 2017;33:331–42.
The American Journal of GASTROENTEROLOGY VOLUME 113 | APRIL 2018 www.nature.com/ajg
Potrebbero piacerti anche
- The Safety of Iloprost in Systemic Sclerosis in A Real-Life ExperienceDocumento7 pagineThe Safety of Iloprost in Systemic Sclerosis in A Real-Life ExperienceArini NurlelaNessuna valutazione finora
- HCM Treatment Italy Ammirati2016Documento13 pagineHCM Treatment Italy Ammirati2016xy manNessuna valutazione finora
- 10 1016@j Ejim 2019 11 017Documento12 pagine10 1016@j Ejim 2019 11 017Mohammad Mahmudur RahmanNessuna valutazione finora
- Proton-Pump Inhibitors and Risk of Renal DiseaseDocumento5 pagineProton-Pump Inhibitors and Risk of Renal Diseaseawanhitam2013Nessuna valutazione finora
- Greuter Et Al Emereging Treatment Options For Extraintestinal Manifestations in IBDDocumento7 pagineGreuter Et Al Emereging Treatment Options For Extraintestinal Manifestations in IBDAriana HurtadoNessuna valutazione finora
- PIIS1078588420310728Documento2 paginePIIS1078588420310728MSNessuna valutazione finora
- Diclocenaco Ynitratos CPREDocumento9 pagineDiclocenaco Ynitratos CPREPaola LastraNessuna valutazione finora
- CKD HT 2Documento7 pagineCKD HT 2Peer TutorNessuna valutazione finora
- Condroitina Uebelhart Clinical Review of Chondroitin Sulfate in Osteoarthritis 2008Documento3 pagineCondroitina Uebelhart Clinical Review of Chondroitin Sulfate in Osteoarthritis 2008Elisabeth PradoNessuna valutazione finora
- Abdominal Pain: Essential Diagnosis and Management in Acute MedicineDa EverandAbdominal Pain: Essential Diagnosis and Management in Acute MedicineNessuna valutazione finora
- 2018 Kanasaki IMA TAC BBDocumento17 pagine2018 Kanasaki IMA TAC BBtesoro100Nessuna valutazione finora
- 10.1007@s11739 019 02210 4Documento7 pagine10.1007@s11739 019 02210 4alexandraNessuna valutazione finora
- Hooper SepsismanagementDocumento42 pagineHooper SepsismanagementElavarasi GanesanNessuna valutazione finora
- Manual Therapy in The Treatment of Carpal Tunnel Syndrome in Diabetic Patients: A Randomized Clinical TrialDocumento7 pagineManual Therapy in The Treatment of Carpal Tunnel Syndrome in Diabetic Patients: A Randomized Clinical TrialHerwanda PrasetyoNessuna valutazione finora
- 2.nonsteroidal Anti-Inflammatory Drug Effects On Renal and Cardiovascular Function From Physiology To Clinical PracticeDocumento18 pagine2.nonsteroidal Anti-Inflammatory Drug Effects On Renal and Cardiovascular Function From Physiology To Clinical Practicemorena19932308Nessuna valutazione finora
- Effects of Low Dose Amitriptyline On Epigastric Pain Syndrome in Functional Dyspepsia PatientsDocumento5 pagineEffects of Low Dose Amitriptyline On Epigastric Pain Syndrome in Functional Dyspepsia PatientsAnnisa apriliaNessuna valutazione finora
- MTX Cardio3Documento8 pagineMTX Cardio3Civic TypeRNessuna valutazione finora
- The Effect of Alternate Nostril Breathing Exercise in Vital Signs of Congestive Heart Failure PatientsDocumento7 pagineThe Effect of Alternate Nostril Breathing Exercise in Vital Signs of Congestive Heart Failure Patientsfrisca susdiNessuna valutazione finora
- Lin 2008Documento9 pagineLin 2008Belkhadir Fatima ZahraNessuna valutazione finora
- ArchRheumatol-2021-36-398Documento11 pagineArchRheumatol-2021-36-398filianalefaanNessuna valutazione finora
- Jurnal DinaDocumento11 pagineJurnal DinaRahma Puji LestariNessuna valutazione finora
- HiperK in CKDDocumento9 pagineHiperK in CKDRaymond RosarioNessuna valutazione finora
- EsomeprazoleDocumento7 pagineEsomeprazoleSanjay NavaleNessuna valutazione finora
- ArticleDocumento9 pagineArticleVictor ValarezoNessuna valutazione finora
- Effective and Safe Proton Pump Inhibitor Therapy in Acid-Related Diseases - A Position Paper Addressing Benefits and Potential Harms of Acid Suppression PDFDocumento35 pagineEffective and Safe Proton Pump Inhibitor Therapy in Acid-Related Diseases - A Position Paper Addressing Benefits and Potential Harms of Acid Suppression PDFmadcraftNessuna valutazione finora
- Obeticholic Acid For The Treatment of Non-Alcoholic Steatohepatitis: Interim Analysis From A Multicentre, Randomised, Placebo-Controlled Phase 3 TrialDocumento13 pagineObeticholic Acid For The Treatment of Non-Alcoholic Steatohepatitis: Interim Analysis From A Multicentre, Randomised, Placebo-Controlled Phase 3 TrialAdo QuirozNessuna valutazione finora
- Scandinavian SurgeryDocumento9 pagineScandinavian SurgeryDyah RendyNessuna valutazione finora
- Serology Biomarker AMIDocumento9 pagineSerology Biomarker AMIDyah RendyNessuna valutazione finora
- Inv Eusebi RevDocumento9 pagineInv Eusebi Revfernandadexiree.melendezNessuna valutazione finora
- Le Comorbilità Della Broncopneumopatia Cronica Ostruttiva: Possibili Implicazioni Nella Gestione Della MalattiaDocumento12 pagineLe Comorbilità Della Broncopneumopatia Cronica Ostruttiva: Possibili Implicazioni Nella Gestione Della MalattiaAndrea VitalianoNessuna valutazione finora
- Topical Steroids in Rhinosinusitis and Intraoperative Bleeding: More Harm Than Good?Documento7 pagineTopical Steroids in Rhinosinusitis and Intraoperative Bleeding: More Harm Than Good?lala poNessuna valutazione finora
- Time-Sensitive Approach in The Management of Acute ESC2020Documento18 pagineTime-Sensitive Approach in The Management of Acute ESC2020Grisel MezaNessuna valutazione finora
- Prevention of Post ERCP Pancreatitis Where Are We NowDocumento5 paginePrevention of Post ERCP Pancreatitis Where Are We NowPaul HartingNessuna valutazione finora
- Original ResearchDocumento14 pagineOriginal ResearchLee제노Nessuna valutazione finora
- Paracetamol: A Review of Guideline Recommendations: Clinical MedicineDocumento22 pagineParacetamol: A Review of Guideline Recommendations: Clinical Medicinevirgilio acostaNessuna valutazione finora
- WS16 Uun S - Empiric Antimicrobial Management of SepsisDocumento12 pagineWS16 Uun S - Empiric Antimicrobial Management of SepsissiputleletNessuna valutazione finora
- Extraintestinal Manifestationsassociated WithinflammatoryboweldiseaseDocumento15 pagineExtraintestinal Manifestationsassociated WithinflammatoryboweldiseaseJEFFERSON MUÑOZNessuna valutazione finora
- Sincope y TEP JAMA 2018Documento7 pagineSincope y TEP JAMA 2018coniestivillNessuna valutazione finora
- Japanese Clinical Practice Guidelines For Pancreaticobiliary MaljunctionDocumento29 pagineJapanese Clinical Practice Guidelines For Pancreaticobiliary MaljunctionadrianiNessuna valutazione finora
- Dynamic Arterial Elastance To Predict Mean Arterial Pressure Decrease After Reduction of Vasopressor in Septic Shock PatientsDocumento12 pagineDynamic Arterial Elastance To Predict Mean Arterial Pressure Decrease After Reduction of Vasopressor in Septic Shock PatientsAltair Monti TeslaNessuna valutazione finora
- Acute Surgical Topics: An Infographic GuideDa EverandAcute Surgical Topics: An Infographic GuideNessuna valutazione finora
- PancreatiteTRADUZIR - ESPEN Guideline On Clinical Nutrition in Acute and Chronic PancreatitisDocumento20 paginePancreatiteTRADUZIR - ESPEN Guideline On Clinical Nutrition in Acute and Chronic Pancreatitisthaisagoraer1Nessuna valutazione finora
- Joa3 12534Documento7 pagineJoa3 12534chasia chaselNessuna valutazione finora
- JTD 11 01 21Documento8 pagineJTD 11 01 21Kornelis AribowoNessuna valutazione finora
- 2017 Hwanglyunhaedok Pharmacopuncture Versus Saline Pharmacopuncture On Chronic Nonbacterial Prostatitis:Chronic Pelvic Pain SyndromeDocumento7 pagine2017 Hwanglyunhaedok Pharmacopuncture Versus Saline Pharmacopuncture On Chronic Nonbacterial Prostatitis:Chronic Pelvic Pain Syndromeenfermeironilson6321Nessuna valutazione finora
- Makalah Dan PPT CS BM HEPARDocumento30 pagineMakalah Dan PPT CS BM HEPARDellar Arciantika CahyaniNessuna valutazione finora
- PMR 2022 0017 PDFDocumento7 paginePMR 2022 0017 PDFStory WA DokterNessuna valutazione finora
- Guideline For Stress Ulcer Prophylaxis in The Intensive Care UnitDocumento4 pagineGuideline For Stress Ulcer Prophylaxis in The Intensive Care Unitannisa edwarNessuna valutazione finora
- FSSG Questionnaire Diagnostic Utility in Asthma Patients with Chronic CoughDocumento19 pagineFSSG Questionnaire Diagnostic Utility in Asthma Patients with Chronic CoughlocolocomedicinaNessuna valutazione finora
- BCS ManagementDocumento3 pagineBCS ManagementdoccommieNessuna valutazione finora
- Fphar 13 1021584Documento11 pagineFphar 13 1021584topanNessuna valutazione finora
- Oftal Case StudyDocumento11 pagineOftal Case StudyMohamad RaisNessuna valutazione finora
- Gastroproteccion Anticoagulacion y AntiagregaciónDocumento13 pagineGastroproteccion Anticoagulacion y AntiagregaciónYesica Villalba CerqueraNessuna valutazione finora
- Durable Pain Relief and Islet Function from TPIATDocumento11 pagineDurable Pain Relief and Islet Function from TPIATEduardo castillo gonzalezNessuna valutazione finora
- Beloncle Et Al Determinants of RRI Impact On Hemodynamic Parameter, AKI and Predisposing FactorsDocumento8 pagineBeloncle Et Al Determinants of RRI Impact On Hemodynamic Parameter, AKI and Predisposing FactorsBijay KCNessuna valutazione finora
- Nakazawa 2016Documento7 pagineNakazawa 2016Yamila VicenteNessuna valutazione finora
- Original Article: Drug Utilization in Patients With OA: A Population-Based StudyDocumento8 pagineOriginal Article: Drug Utilization in Patients With OA: A Population-Based StudyShafira TamaraNessuna valutazione finora
- Refeeding Syndrome PDFDocumento5 pagineRefeeding Syndrome PDFManuel ArenasNessuna valutazione finora
- JurnalDocumento16 pagineJurnalsamuelionardiNessuna valutazione finora
- 2 (OA) Pazir 2021 - Impaired Semen Parameters in Patients With Confirmed SARS CoV 2 InfectionDocumento6 pagine2 (OA) Pazir 2021 - Impaired Semen Parameters in Patients With Confirmed SARS CoV 2 InfectionsamuelionardiNessuna valutazione finora
- Collins 2022 (Review) - Impact of Covid-19 On Male FertilityDocumento7 pagineCollins 2022 (Review) - Impact of Covid-19 On Male FertilitysamuelionardiNessuna valutazione finora
- 1 (OA) Best 2021 - Evaluation Off Sars Cov 2 in Human Semen and Effect OnDocumento7 pagine1 (OA) Best 2021 - Evaluation Off Sars Cov 2 in Human Semen and Effect OnsamuelionardiNessuna valutazione finora
- Fave 2021 (Review) - COVID-19 and Male Fertility, Taking Stock of One Year After The Outbreak BeganDocumento5 pagineFave 2021 (Review) - COVID-19 and Male Fertility, Taking Stock of One Year After The Outbreak BegansamuelionardiNessuna valutazione finora
- Certificate: Sexuality, Sexual and Reproduct Ive Health: Fall 2021 Entering StudentsDocumento3 pagineCertificate: Sexuality, Sexual and Reproduct Ive Health: Fall 2021 Entering StudentssamuelionardiNessuna valutazione finora
- Booklet The 8th JAKINUDocumento20 pagineBooklet The 8th JAKINUsamuelionardiNessuna valutazione finora
- (17417899 - Reproduction) Evaluating The Impact of COVID-19 On Male ReproductionDocumento8 pagine(17417899 - Reproduction) Evaluating The Impact of COVID-19 On Male Reproductionandre fregolenteNessuna valutazione finora
- Certificate: Child, Youth, and Family Health: Fall 2021 Entering StudentsDocumento2 pagineCertificate: Child, Youth, and Family Health: Fall 2021 Entering StudentssamuelionardiNessuna valutazione finora
- General Anatomy of Skull & ScalpDocumento21 pagineGeneral Anatomy of Skull & ScalpsamuelionardiNessuna valutazione finora
- Evidence Based Medicine: PICO Search Strategy for Cure Rate of Typhoid Patients on AntibioticsDocumento7 pagineEvidence Based Medicine: PICO Search Strategy for Cure Rate of Typhoid Patients on AntibioticssamuelionardiNessuna valutazione finora
- Evidence Based Medicine: PICO Search Strategy for Cure Rate of Typhoid Patients on AntibioticsDocumento7 pagineEvidence Based Medicine: PICO Search Strategy for Cure Rate of Typhoid Patients on AntibioticssamuelionardiNessuna valutazione finora
- Soal Batch IIDocumento2 pagineSoal Batch IIsamuelionardiNessuna valutazione finora
- Soal Batch IIDocumento2 pagineSoal Batch IIsamuelionardiNessuna valutazione finora
- Soal Batch IIDocumento2 pagineSoal Batch IIsamuelionardiNessuna valutazione finora
- Soal Batch IIDocumento2 pagineSoal Batch IIsamuelionardiNessuna valutazione finora
- (Padi) Soal To CBT 6 Batch 2 2019Documento22 pagine(Padi) Soal To CBT 6 Batch 2 2019samuelionardiNessuna valutazione finora
- Journal BPDocumento7 pagineJournal BPsamuelionardiNessuna valutazione finora
- Weight Loss InterventionDocumento21 pagineWeight Loss InterventionsamuelionardiNessuna valutazione finora
- TG 13 Updated Tokyo GuidelinesDocumento8 pagineTG 13 Updated Tokyo GuidelinessamuelionardiNessuna valutazione finora
- Leaflet ANCDocumento3 pagineLeaflet ANCsamuelionardiNessuna valutazione finora
- Jurnal 2Documento22 pagineJurnal 2samuelionardiNessuna valutazione finora
- Discontinuing PPI Ajg201829Documento10 pagineDiscontinuing PPI Ajg201829samuelionardiNessuna valutazione finora
- Stase 30 April 2018: Sudinkes Jakarta Barat & KarawangDocumento2 pagineStase 30 April 2018: Sudinkes Jakarta Barat & KarawangChristopher BurnsNessuna valutazione finora
- NEW - Konsensus Pengelolaan & Pencegahan DM Tipe 2 Di INDONESIA - Edisi 2015Documento93 pagineNEW - Konsensus Pengelolaan & Pencegahan DM Tipe 2 Di INDONESIA - Edisi 2015familyman80100% (3)
- Achilles Tendon Ruptures Dr. YanuarsoDocumento56 pagineAchilles Tendon Ruptures Dr. Yanuarsofahmi aryandiNessuna valutazione finora
- PDFJurnal Jantung 1Documento21 paginePDFJurnal Jantung 1samuelionardiNessuna valutazione finora
- Achilles Tendon Ruptures Dr. YanuarsoDocumento56 pagineAchilles Tendon Ruptures Dr. Yanuarsofahmi aryandiNessuna valutazione finora
- Sclar 2004Documento16 pagineSclar 2004Kelly N100% (1)
- TEDPB and Disability Support ServicesDocumento3 pagineTEDPB and Disability Support ServicesIrshaad Ally Ashrafi GolapkhanNessuna valutazione finora
- Child AbuseDocumento5 pagineChild AbusePeng Peng LimNessuna valutazione finora
- Agreement For Puppy BlankoDocumento3 pagineAgreement For Puppy BlankoMarko TardelliNessuna valutazione finora
- Introducing The Epidermis.: ReallyDocumento47 pagineIntroducing The Epidermis.: ReallyNaila JinNessuna valutazione finora
- Autocoid PharmacologyDocumento29 pagineAutocoid PharmacologyLyadelou Fortu100% (1)
- Endocrine Society Hypercalcemia MalignancyDocumento22 pagineEndocrine Society Hypercalcemia MalignancyJoão Pedro RibasNessuna valutazione finora
- Hospital Waste Water TreatmentDocumento5 pagineHospital Waste Water TreatmentNP100% (1)
- DAILY LESSON Plan 4 - 1.8Documento4 pagineDAILY LESSON Plan 4 - 1.8Wilbeth PanganibanNessuna valutazione finora
- A New Papilla Preservation Technique For Periodontal Regeneration of Severely Compromised TeethDocumento6 pagineA New Papilla Preservation Technique For Periodontal Regeneration of Severely Compromised TeethmaxNessuna valutazione finora
- E Stim PDFDocumento6 pagineE Stim PDFAlvaro Toledo100% (1)
- Background: Pediatric Chickenpox Next Section: PathophysiologyDocumento12 pagineBackground: Pediatric Chickenpox Next Section: PathophysiologyRachel Johann Aquinto100% (1)
- Research ArticleDocumento4 pagineResearch ArticleBharathi RagavanNessuna valutazione finora
- Med Surge 2 Mod 3 Study GuideDocumento19 pagineMed Surge 2 Mod 3 Study GuideDirk Buckner100% (4)
- Jack Poylangada - Copy of Stamper Self-Care JournalDocumento8 pagineJack Poylangada - Copy of Stamper Self-Care Journalapi-503633296100% (3)
- Hepatitis ADocumento58 pagineHepatitis AClaireGrandeNessuna valutazione finora
- Monoclonal Antibodies The Next Generation April 2010Documento10 pagineMonoclonal Antibodies The Next Generation April 2010Al ChevskyNessuna valutazione finora
- Myopia ManualDocumento337 pagineMyopia ManualRealPurgatory100% (1)
- Chron's Disease 2Documento3 pagineChron's Disease 2TarantadoNessuna valutazione finora
- Twins Bootcamp StudyDocumento5 pagineTwins Bootcamp Studyandi dirhanNessuna valutazione finora
- TramadolDocumento19 pagineTramadolanandhra2010Nessuna valutazione finora
- Formulation and Evaluation of Antiseptic Polyherbal OintmentDocumento11 pagineFormulation and Evaluation of Antiseptic Polyherbal OintmentandrapradeshsseNessuna valutazione finora
- Non-Modifiable Risk Factors: Modifiable Risk FactorsDocumento9 pagineNon-Modifiable Risk Factors: Modifiable Risk FactorsKimberly Bomediano100% (1)
- Reiki Master Manual (Odd)Documento47 pagineReiki Master Manual (Odd)Kaya Niranjan Kumar ReddyNessuna valutazione finora
- Cervicogenic HeadacheDocumento8 pagineCervicogenic HeadacheEmma KopcikasNessuna valutazione finora
- Practice Guidelines For The Diagnosis and Management of Aspergilosis 2016 Update by AmericaDocumento60 paginePractice Guidelines For The Diagnosis and Management of Aspergilosis 2016 Update by AmericaNur Prasetyo Nugroho100% (1)
- Magnetic StimulationDocumento5 pagineMagnetic StimulationMikaelNJonssonNessuna valutazione finora
- Bio Medical Waste Management and Handling Environment LawDocumento15 pagineBio Medical Waste Management and Handling Environment LawAnkit Tyagi100% (1)
- Nucleus DropDocumento1 paginaNucleus DropYovinus DenyNessuna valutazione finora
- Critical AppraisalDocumento132 pagineCritical AppraisalSanditia Gumilang100% (2)