Potrebbero piacerti anche
- English Report PDFDocumento18 pagineEnglish Report PDFDewanggaWahyuPrajaNessuna valutazione finora
- Sticherling Christian 20160616 0800 Room 5ABDocumento23 pagineSticherling Christian 20160616 0800 Room 5ABDewanggaWahyuPrajaNessuna valutazione finora
- 4 FullDocumento9 pagine4 FullDewanggaWahyuPrajaNessuna valutazione finora
- Bookshelf NBK258 PDFDocumento3 pagineBookshelf NBK258 PDFDewanggaWahyuPrajaNessuna valutazione finora
- EULAR Recommendations For The Management of Rheumatoid Arthritis With Synthetic and Biological Disease-Modifying Antirheumatic Drugs: 2013 UpdateDocumento18 pagineEULAR Recommendations For The Management of Rheumatoid Arthritis With Synthetic and Biological Disease-Modifying Antirheumatic Drugs: 2013 UpdateDewanggaWahyuPrajaNessuna valutazione finora
- Evaluation of Three Paediatric Weight Estimation Methods in SingaporeDocumento6 pagineEvaluation of Three Paediatric Weight Estimation Methods in SingaporeDewanggaWahyuPrajaNessuna valutazione finora
- SCFguideline PDFDocumento210 pagineSCFguideline PDFDewanggaWahyuPrajaNessuna valutazione finora
- Anmsd Ahsdas HdasdaskjdasdbaskjdbasbdbaskdjakjdjkajsdjasjkdDocumento1 paginaAnmsd Ahsdas HdasdaskjdasdbaskjdbasbdbaskdjakjdjkajsdjasjkdDewanggaWahyuPrajaNessuna valutazione finora
- Wilson Disease2009 PDFDocumento23 pagineWilson Disease2009 PDFDewanggaWahyuPrajaNessuna valutazione finora
- AcuteLiverFailureUpdate201journalformat1 PDFDocumento26 pagineAcuteLiverFailureUpdate201journalformat1 PDFDewanggaWahyuPrajaNessuna valutazione finora
- Apasl HBV Guideline 2016 PDFDocumento98 pagineApasl HBV Guideline 2016 PDFDewanggaWahyuPrajaNessuna valutazione finora
- S CF GuidelineDocumento210 pagineS CF GuidelineDewanggaWahyuPrajaNessuna valutazione finora
- EvaluationPediatricLT2014 PDFDocumento37 pagineEvaluationPediatricLT2014 PDFDewanggaWahyuPrajaNessuna valutazione finora
- Guideline Ascites 4UFb 2015 PDFDocumento96 pagineGuideline Ascites 4UFb 2015 PDFDewanggaWahyuPrajaNessuna valutazione finora
- Nihms794087 PDFDocumento23 pagineNihms794087 PDFDewanggaWahyuPrajaNessuna valutazione finora
- S574.Full - First AIDDocumento17 pagineS574.Full - First AIDOséias AlvesNessuna valutazione finora
- S526 FullDocumento3 pagineS526 FullDewanggaWahyuPrajaNessuna valutazione finora
- 2017 Una Guia para Las Directrices Sepsis 2016Documento5 pagine2017 Una Guia para Las Directrices Sepsis 2016mpacajeNessuna valutazione finora
- C P A G F A Q (Faq) F P P MDocumento2 pagineC P A G F A Q (Faq) F P P MDewanggaWahyuPrajaNessuna valutazione finora
- 2017 American Heart Association Focused Update On Adult Basic Life Support and Cardiopulmonary Resuscitation QualityDocumento8 pagine2017 American Heart Association Focused Update On Adult Basic Life Support and Cardiopulmonary Resuscitation QualityDewanggaWahyuPrajaNessuna valutazione finora
- Review Article: The Cardiorenal Syndrome: A ReviewDocumento11 pagineReview Article: The Cardiorenal Syndrome: A ReviewrezykurniaNessuna valutazione finora
- Ehp507 PDFDocumento12 pagineEhp507 PDFDewanggaWahyuPrajaNessuna valutazione finora
- Acute Kidney Injury in Cardiorenal Syndrome Type 1 Patients: A Systematic Review and Meta-AnalysisDocumento13 pagineAcute Kidney Injury in Cardiorenal Syndrome Type 1 Patients: A Systematic Review and Meta-AnalysisDewanggaWahyuPrajaNessuna valutazione finora
- Pals 2015Documento18 paginePals 2015Sardono WidinugrohoNessuna valutazione finora
- Practice Guidelines As Implementation Science: The Journal Editors' PerspectiveDocumento2 paginePractice Guidelines As Implementation Science: The Journal Editors' PerspectiveDewanggaWahyuPrajaNessuna valutazione finora
- Management of Osteoarthritis of The Hip Companion Consensus Statements - 3.13.17Documento48 pagineManagement of Osteoarthritis of The Hip Companion Consensus Statements - 3.13.17DewanggaWahyuPrajaNessuna valutazione finora
- ACL Companion Consensus StatementsDocumento10 pagineACL Companion Consensus StatementsDewanggaWahyuPrajaNessuna valutazione finora
- Kdigo CKD GL Suppl Table Jan 2013Documento10 pagineKdigo CKD GL Suppl Table Jan 2013DewanggaWahyuPrajaNessuna valutazione finora
- Hand Hygiene When and How LeafletDocumento2 pagineHand Hygiene When and How Leaflet13eNessuna valutazione finora
- Fluid Electrolyte TherapyDocumento15 pagineFluid Electrolyte Therapyaarm1990Nessuna valutazione finora
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (399)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (73)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (120)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- Using N, N, N',N'-tetramethyl-p-phenylenediamine (TMPD) To Assay Cyclooxygenase Activity in VitroDocumento13 pagineUsing N, N, N',N'-tetramethyl-p-phenylenediamine (TMPD) To Assay Cyclooxygenase Activity in VitroTatianaAlejandraCárdenasSolanoNessuna valutazione finora
- Marketing Mix Concept Based On One Pharmaceutical Company ProductDocumento12 pagineMarketing Mix Concept Based On One Pharmaceutical Company ProductDlow LopSkfnNessuna valutazione finora
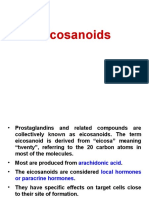
- ProstaglandinsDocumento33 pagineProstaglandinsAshwanth M.SNessuna valutazione finora
- Bp503t Pcol Unit-IIIDocumento38 pagineBp503t Pcol Unit-IIIAakkkNessuna valutazione finora
- Sytenol A Brochure Acne 2016Documento8 pagineSytenol A Brochure Acne 2016dian kaizenNessuna valutazione finora
- NSAIDDocumento1 paginaNSAIDShubhangiNessuna valutazione finora
- Role of Herbals As Anti-Cancer and Anti-Inflammatory AgentsDocumento11 pagineRole of Herbals As Anti-Cancer and Anti-Inflammatory AgentsInternational Journal of Innovative Science and Research TechnologyNessuna valutazione finora
- Nephar 305 Nsaids - 15Documento48 pagineNephar 305 Nsaids - 15NUR KINTAN APRILIANessuna valutazione finora
- Laboratory Manual: Biology 3055Documento37 pagineLaboratory Manual: Biology 3055Raj Kumar SoniNessuna valutazione finora
- NSAIDSDocumento12 pagineNSAIDSNikita ShokurNessuna valutazione finora
- Cytoplasmic Labile Iron Accumulates in Aging Stem Cells Perturbing A Key Rheostat For Identity ControlDocumento71 pagineCytoplasmic Labile Iron Accumulates in Aging Stem Cells Perturbing A Key Rheostat For Identity ControlValen EstevezNessuna valutazione finora
- AceclofenacDocumento26 pagineAceclofenacKamrun S NaharNessuna valutazione finora
- ACOG Committee Opinion No. 743 Low-Dose Aspirin Use During PregnancyDocumento9 pagineACOG Committee Opinion No. 743 Low-Dose Aspirin Use During PregnancyJaime RdNessuna valutazione finora
- Physiology of Labor: Moderator: Dr. Angesom.K, Obs/ Gyn-SpecialistDocumento58 paginePhysiology of Labor: Moderator: Dr. Angesom.K, Obs/ Gyn-SpecialistYobed MengeshaNessuna valutazione finora
- NSAIDDocumento22 pagineNSAIDaisyahNessuna valutazione finora
- Cyclooxygenase Enzyme Inhibitory Property of Anoxe®Documento5 pagineCyclooxygenase Enzyme Inhibitory Property of Anoxe®wxcvbnnbvcxwNessuna valutazione finora
- Analgesicos No Opiodes No Esteroideos y Cox SelectivosDocumento14 pagineAnalgesicos No Opiodes No Esteroideos y Cox SelectivosXY PragmaNessuna valutazione finora
- Contraindicaciones Del Flunixin en GatosDocumento26 pagineContraindicaciones Del Flunixin en GatosCami GamboaNessuna valutazione finora
- EicosanoidsDocumento22 pagineEicosanoidsKifayat Kamal NowshinNessuna valutazione finora
- Nsaids Nonsteroidal Anti-Inflammatory Drugs: Maher Khdour Msc. Phd. Clinical PharmacyDocumento65 pagineNsaids Nonsteroidal Anti-Inflammatory Drugs: Maher Khdour Msc. Phd. Clinical PharmacyYousef JafarNessuna valutazione finora
- Acetylsalicylic Acid 99.pdf SIGMADocumento5 pagineAcetylsalicylic Acid 99.pdf SIGMAFadli IkhsanNessuna valutazione finora
- Prostaglandins: Dr. Mohammed Shakil AkhtarDocumento25 pagineProstaglandins: Dr. Mohammed Shakil AkhtarShimmering MoonNessuna valutazione finora
- Nutritional and Medical Applications of Spirulina MicroalgaeDocumento7 pagineNutritional and Medical Applications of Spirulina MicroalgaenaniyagamiNessuna valutazione finora
- Chapter: One: Introduction and Aim of The ThesisDocumento12 pagineChapter: One: Introduction and Aim of The ThesislichenresearchNessuna valutazione finora
- Osteoarthritis, Inflammation and DegradationDocumento317 pagineOsteoarthritis, Inflammation and DegradationItai IzhakNessuna valutazione finora
- Antioxidant and Anti-Inflammatory Assays Confirm Bioactive Compounds in Ajwa Date FruitDocumento7 pagineAntioxidant and Anti-Inflammatory Assays Confirm Bioactive Compounds in Ajwa Date Fruitrizla67100% (1)
- Non-Selective Cox 1&2 Inhibitors: AspirinDocumento13 pagineNon-Selective Cox 1&2 Inhibitors: AspirinKristijan GoldašićNessuna valutazione finora
- Prepare Drug Profile of Aspirin: 1. Product DescriptionDocumento11 paginePrepare Drug Profile of Aspirin: 1. Product DescriptionUmna QureshiNessuna valutazione finora
- Docking and Molecular Dynamics Calculations of PyrDocumento15 pagineDocking and Molecular Dynamics Calculations of PyrVeliyana Londong AlloNessuna valutazione finora
- Sources of NADPHDocumento41 pagineSources of NADPHPalesa NtsekalleNessuna valutazione finora