Potrebbero piacerti anche
- The Human Microbiota: How Microbial Communities Affect Health and DiseaseDa EverandThe Human Microbiota: How Microbial Communities Affect Health and DiseaseValutazione: 3.5 su 5 stelle3.5/5 (6)
- Investigating Human Diseases with the Microbiome: Metagenomics Bench to BedsideDa EverandInvestigating Human Diseases with the Microbiome: Metagenomics Bench to BedsideNessuna valutazione finora
- The Human Microbiome Project: A Community Resource For The Healthy Human MicrobiomeDocumento6 pagineThe Human Microbiome Project: A Community Resource For The Healthy Human MicrobiomeJam Uly GastyNessuna valutazione finora
- Human Microbiome Acquisition and Bioinformatic Challenges in Metagenomic StudiesDocumento12 pagineHuman Microbiome Acquisition and Bioinformatic Challenges in Metagenomic StudiesAminaHodžićNessuna valutazione finora
- The Hoops, Hopes, and Hypes of Human Microbiome ResearchDocumento11 pagineThe Hoops, Hopes, and Hypes of Human Microbiome ResearchIHTISHAM UL HAQNessuna valutazione finora
- Gut MicrobiomeDocumento23 pagineGut Microbiomejyotisingh7Nessuna valutazione finora
- Pro Pre HarvardDocumento18 paginePro Pre HarvardTran Thach Uyen NhiNessuna valutazione finora
- Human Microbiome - Symbiosis To PathogenesisDocumento6 pagineHuman Microbiome - Symbiosis To PathogenesisAle Pushoa UlloaNessuna valutazione finora
- The Intestinal Microbiome and Surgical DiseaseDocumento37 pagineThe Intestinal Microbiome and Surgical DiseaseBolivar IseaNessuna valutazione finora
- 1-S2.0-S0009898115000170-Main Microbiomul Si Sanatatea Adultului PDFDocumento6 pagine1-S2.0-S0009898115000170-Main Microbiomul Si Sanatatea Adultului PDFLUTICHIEVICI NATALIANessuna valutazione finora
- Investigators' Perspectives On Translating Human Microbiome Research Into Clinical PracticeDocumento7 pagineInvestigators' Perspectives On Translating Human Microbiome Research Into Clinical Practiceabcder1234Nessuna valutazione finora
- Microbial Community Profiling of Human SalivaDocumento10 pagineMicrobial Community Profiling of Human SalivaJobin John PR15BI1001Nessuna valutazione finora
- Benezra DeStefano Gordon 2012 Anthropology of Microbes PDFDocumento4 pagineBenezra DeStefano Gordon 2012 Anthropology of Microbes PDFxxongh1Nessuna valutazione finora
- The Human Microbiome and Infectious Diseases: Beyond KochDocumento151 pagineThe Human Microbiome and Infectious Diseases: Beyond KochRamesh ShahNessuna valutazione finora
- Research Paper On Environmental MicrobiologyDocumento7 pagineResearch Paper On Environmental Microbiologywwvmdfvkg100% (1)
- RESEARCH Open Access Characterizing Oral Microbial Communities Across Dentition States and Colonization NichesDocumento10 pagineRESEARCH Open Access Characterizing Oral Microbial Communities Across Dentition States and Colonization NichesMuhammad HuzaifaNessuna valutazione finora
- Human Microbiome Handbook PreviewDocumento50 pagineHuman Microbiome Handbook PreviewBularda CrinaNessuna valutazione finora
- Annual Research Review: Critical Windows - The Microbiota - Gut-Brain Axis in Neurocognitive DevelopmentDocumento19 pagineAnnual Research Review: Critical Windows - The Microbiota - Gut-Brain Axis in Neurocognitive DevelopmentDhanush PNessuna valutazione finora
- NIH Human Microbiome Project Characterizes Microbial CommunitiesDocumento7 pagineNIH Human Microbiome Project Characterizes Microbial CommunitiesNicole WijayaNessuna valutazione finora
- Mam BascoDocumento2 pagineMam BascoFlorence De ChavezNessuna valutazione finora
- Using Data Science For Medical Decision Making Case: Role of Gut Microbiome in Multiple SclerosisDocumento11 pagineUsing Data Science For Medical Decision Making Case: Role of Gut Microbiome in Multiple SclerosisUhtredNessuna valutazione finora
- GB 2013 14 1 r1 PDFDocumento18 pagineGB 2013 14 1 r1 PDFabcder1234Nessuna valutazione finora
- Ijms 24 13507Documento15 pagineIjms 24 13507Kikin RizkynnisaNessuna valutazione finora
- The Vaginal Microbiota: Insights From High-Throughput SequencingDocumento15 pagineThe Vaginal Microbiota: Insights From High-Throughput SequencingHauNessuna valutazione finora
- Integrating The Human Microbiome in The Foresic ToolkitDocumento15 pagineIntegrating The Human Microbiome in The Foresic ToolkitAdnanNessuna valutazione finora
- Dekaboruah2020 Article HumanMicrobiomeAnAcademicUpdatDocumento21 pagineDekaboruah2020 Article HumanMicrobiomeAnAcademicUpdatMauricio MenaNessuna valutazione finora
- Breakthroughs in Biosciences and The Question of Morality Interactions Between Ethics and Bioscience PracticesDocumento9 pagineBreakthroughs in Biosciences and The Question of Morality Interactions Between Ethics and Bioscience PracticesIDWAR STNessuna valutazione finora
- Research Paper On Clinical MicrobiologyDocumento5 pagineResearch Paper On Clinical Microbiologyukldyebkf100% (1)
- Gastrointestinal Microbiology - A. Ouwehand, E. Vaughan (Taylor and Francis, 2006) WW PDFDocumento431 pagineGastrointestinal Microbiology - A. Ouwehand, E. Vaughan (Taylor and Francis, 2006) WW PDFGabriela Balan100% (2)
- Biobanks in The Era of Personalized MedicineDocumento12 pagineBiobanks in The Era of Personalized MedicinenylirameNessuna valutazione finora
- Preprints201809 0388 v1Documento35 paginePreprints201809 0388 v1Mayra SaenzNessuna valutazione finora
- Paper BioeticaDocumento2 paginePaper BioeticaRaúl ArroyoNessuna valutazione finora
- Consent Ethics and Genetic BiobanksDocumento10 pagineConsent Ethics and Genetic BiobanksgdlievanogNessuna valutazione finora
- Biodefense The Challenge For A New Microbial HunterDocumento2 pagineBiodefense The Challenge For A New Microbial HunterjuangbuenoNessuna valutazione finora
- Hiergeist Et Al, 2015 - Analise Da Microbiota Intestinal HumanoDocumento13 pagineHiergeist Et Al, 2015 - Analise Da Microbiota Intestinal HumanoanavcmeloNessuna valutazione finora
- TD1 Microbiologie Médicale Pérez-Carrasco Et Al., 2021Documento17 pagineTD1 Microbiologie Médicale Pérez-Carrasco Et Al., 2021abekhti abdelkaderNessuna valutazione finora
- Revised Estimates For The Number of Human and Bacteria Cells in The BodyDocumento21 pagineRevised Estimates For The Number of Human and Bacteria Cells in The BodyCaio SilvaNessuna valutazione finora
- Blake Zucco Independent Research Period 3Documento6 pagineBlake Zucco Independent Research Period 3api-321753881Nessuna valutazione finora
- Subjective On DemandDocumento6 pagineSubjective On DemandwadhitaubahNessuna valutazione finora
- Genome, Transcriptome and Proteome PDFDocumento17 pagineGenome, Transcriptome and Proteome PDFAdn CodeNessuna valutazione finora
- Articulo OxforDocumento16 pagineArticulo OxforbosueNessuna valutazione finora
- 1 s2.0 S2352552521000761 MainDocumento2 pagine1 s2.0 S2352552521000761 MainCharlierNessuna valutazione finora
- An Insight Into Gut Microbiota and Its Functionalities: Atanu Adak Mojibur R. KhanDocumento21 pagineAn Insight Into Gut Microbiota and Its Functionalities: Atanu Adak Mojibur R. Khanmacihi7305Nessuna valutazione finora
- Conducting A Microbiome StudyDocumento29 pagineConducting A Microbiome StudyTeodolinda HuertaNessuna valutazione finora
- Marselle 2021Documento22 pagineMarselle 2021Thom KeijzerNessuna valutazione finora
- The Effects of Antibiotics On The Microbiome Throughout Development and Alternative Approaches For Therapeutic ModulationDocumento16 pagineThe Effects of Antibiotics On The Microbiome Throughout Development and Alternative Approaches For Therapeutic ModulationBlasting DaveNessuna valutazione finora
- MannixDocumento32 pagineMannixLaura GaviriaNessuna valutazione finora
- Role of The Intestinal Microbiome in Health and Disease: From Correlation To CausationDocumento12 pagineRole of The Intestinal Microbiome in Health and Disease: From Correlation To CausationAlexa MaciucaNessuna valutazione finora
- Human Milk: A Source of More Life Than We ImagineDocumento14 pagineHuman Milk: A Source of More Life Than We Imagineminorka17Nessuna valutazione finora
- Neuroscience and Biobehavioral Reviews: Bogdana Golofast, Karel Vales TDocumento20 pagineNeuroscience and Biobehavioral Reviews: Bogdana Golofast, Karel Vales Ttimea_gheneaNessuna valutazione finora
- Community Health Care Therapeutic Opportunities in The Human MicrobiomeDocumento5 pagineCommunity Health Care Therapeutic Opportunities in The Human Microbiomeabcder1234Nessuna valutazione finora
- Microbiome JournalDocumento14 pagineMicrobiome JournalTiara Rachmaputeri AriantoNessuna valutazione finora
- 1 Ethic and BiosecurityDocumento6 pagine1 Ethic and BiosecurityajengNessuna valutazione finora
- Oup Accepted Manuscript 2016Documento17 pagineOup Accepted Manuscript 2016Janescu LucianNessuna valutazione finora
- The Human Microbiome Project: Lessons From Human GenomicsDocumento4 pagineThe Human Microbiome Project: Lessons From Human GenomicskiranshanesNessuna valutazione finora
- Legal MedicineDocumento8 pagineLegal MedicineElva PatabangNessuna valutazione finora
- Basic Research On Bacteria: The Essential FrontierDocumento16 pagineBasic Research On Bacteria: The Essential FrontierMircea MirceaNessuna valutazione finora
- Fifty Important Research Questions in Microbial EcologyDocumento10 pagineFifty Important Research Questions in Microbial EcologyJericho CarenaNessuna valutazione finora
- BMJ j831 FullDocumento14 pagineBMJ j831 FullsznistvanNessuna valutazione finora
- Perlman 2016 Mouse Models of Human Disease An EvDocumento7 paginePerlman 2016 Mouse Models of Human Disease An EvChen AiNessuna valutazione finora
- Problem BasedDocumento3 pagineProblem BasedLady KweeNessuna valutazione finora
- Different Laboratory Service ModelsDocumento1 paginaDifferent Laboratory Service ModelsGerald John PazNessuna valutazione finora
- Drug Abuse Video GuidelinesDocumento1 paginaDrug Abuse Video GuidelinesGerald John PazNessuna valutazione finora
- Problem Based Learning PDFDocumento1 paginaProblem Based Learning PDFGerald John PazNessuna valutazione finora
- Chapter 021Documento49 pagineChapter 021Gerald John PazNessuna valutazione finora
- 1 s2.0 S0167701216302627 MainDocumento8 pagine1 s2.0 S0167701216302627 MainGerald John PazNessuna valutazione finora
- The Impact of Teacher Presentation Style: (Please Email Me at For A References List.)Documento5 pagineThe Impact of Teacher Presentation Style: (Please Email Me at For A References List.)kashanpirzadaNessuna valutazione finora
- Phlebotomy: Phlebos - Greek Word Meaning "Vein" & Tome - "To Cut"Documento5 paginePhlebotomy: Phlebos - Greek Word Meaning "Vein" & Tome - "To Cut"Gerald John PazNessuna valutazione finora
- GROUP11 Section1 PBL2 Gerald John PazDocumento1 paginaGROUP11 Section1 PBL2 Gerald John PazGerald John PazNessuna valutazione finora
- Geopolitical Challenges For Infectious Disease Prevention and ControlDocumento17 pagineGeopolitical Challenges For Infectious Disease Prevention and ControlGerald John PazNessuna valutazione finora
- Concepts of Culture MediaDocumento1 paginaConcepts of Culture MediaGerald John PazNessuna valutazione finora
- Chapter 022Documento100 pagineChapter 022Gerald John PazNessuna valutazione finora
- Gene Therapy May Prevent Retinoschisis in Boys: ReviewDocumento2 pagineGene Therapy May Prevent Retinoschisis in Boys: ReviewGerald John PazNessuna valutazione finora
- Case Studies On CoagulationDocumento3 pagineCase Studies On CoagulationGerald John PazNessuna valutazione finora
- Role of Microbiota in Immunity and InflammationDocumento12 pagineRole of Microbiota in Immunity and InflammationGerald John PazNessuna valutazione finora
- Host Microbiomes and Their Interactions With Immune SystemDocumento9 pagineHost Microbiomes and Their Interactions With Immune SystemGerald John PazNessuna valutazione finora
- Chapter 025Documento31 pagineChapter 025Gerald John PazNessuna valutazione finora
- Chapter 023Documento34 pagineChapter 023Gerald John PazNessuna valutazione finora
- Chapter 024Documento49 pagineChapter 024Gerald John PazNessuna valutazione finora
- Laboratory Safety ChapterDocumento39 pagineLaboratory Safety ChapterGerald John PazNessuna valutazione finora
- Managment and Planning PDFDocumento53 pagineManagment and Planning PDFGerald John PazNessuna valutazione finora
- Chapter 023Documento34 pagineChapter 023Gerald John PazNessuna valutazione finora
- Chapter 002Documento68 pagineChapter 002Gerald John PazNessuna valutazione finora
- Chapter 001Documento83 pagineChapter 001Gerald John PazNessuna valutazione finora
- Papa Bear of The Berenstain BearsDocumento1 paginaPapa Bear of The Berenstain BearsGerald John PazNessuna valutazione finora
- The First Blind Man On Top of The WorldDocumento1 paginaThe First Blind Man On Top of The WorldGerald John PazNessuna valutazione finora
- Short Report: Genetics Islet Autoantibodies Can Discriminate Maturity-Onset Diabetes of The Young (MODY) From Type 1 DiabetesDocumento7 pagineShort Report: Genetics Islet Autoantibodies Can Discriminate Maturity-Onset Diabetes of The Young (MODY) From Type 1 DiabetesGerald John PazNessuna valutazione finora
- GROUP 6-Micro Biochem ResultsDocumento2 pagineGROUP 6-Micro Biochem ResultsGerald John PazNessuna valutazione finora
- Managment and PlanningDocumento53 pagineManagment and PlanningGerald John PazNessuna valutazione finora
- DynamedDocumento41 pagineDynamedkaren AlvaradoNessuna valutazione finora
- Nature Magazine 7170 - 2007-11-29Documento189 pagineNature Magazine 7170 - 2007-11-29Roberto KlesNessuna valutazione finora
- Replication, Transcription, Translation QuizDocumento4 pagineReplication, Transcription, Translation QuizAakash ReddyNessuna valutazione finora
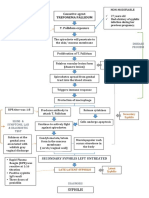
- Pathophysiology of Syphilis ReinfectionDocumento1 paginaPathophysiology of Syphilis Reinfection3S - JOCSON, DENESE NICOLE LEE M.Nessuna valutazione finora
- Wound Care in Orthopaedic Case-Borromeus HospitalDocumento96 pagineWound Care in Orthopaedic Case-Borromeus HospitalDavid DavidNessuna valutazione finora
- Immune Response to Viral Infections: The Role of Interferons and Cell-Mediated ImmunityDocumento20 pagineImmune Response to Viral Infections: The Role of Interferons and Cell-Mediated ImmunityErum JanNessuna valutazione finora
- HACCP PLAN Sample Report PDFDocumento7 pagineHACCP PLAN Sample Report PDFBhaskar Shitole100% (1)
- Complications of Blood TransfusionsDocumento4 pagineComplications of Blood TransfusionsZain Hadi100% (1)
- Week 006 Animal-Immune-SystemDocumento13 pagineWeek 006 Animal-Immune-SystemMark Lorens StaanaNessuna valutazione finora
- New Hope For A Cure To Liver CirrhosisDocumento2 pagineNew Hope For A Cure To Liver Cirrhosissina_bopol100% (1)
- CytogeneticsDocumento17 pagineCytogeneticsLee LuceroNessuna valutazione finora
- Protozoan - Intestinal SporozoaDocumento39 pagineProtozoan - Intestinal SporozoafsdafvNessuna valutazione finora
- The Lymphatic SystemDocumento27 pagineThe Lymphatic Systemوجد عمرNessuna valutazione finora
- (ASM403) Reflective Paper Wan Muhammad Akram Bin Wan Mohd Azli Ba2321aDocumento2 pagine(ASM403) Reflective Paper Wan Muhammad Akram Bin Wan Mohd Azli Ba2321aWan Muhammad AkramNessuna valutazione finora
- CV of Indonesian Nursing Professor and ResearcherDocumento5 pagineCV of Indonesian Nursing Professor and Researcherwedus2Nessuna valutazione finora
- Hiv & Persons Living With HIVDocumento32 pagineHiv & Persons Living With HIVjericho dinglasanNessuna valutazione finora
- Mushtaq Ahmad: Running Head: REFLECTIVE LOG 1Documento5 pagineMushtaq Ahmad: Running Head: REFLECTIVE LOG 1Shafiq Ur RahmanNessuna valutazione finora
- Endemic Infusate Contamination and Related BactereDocumento7 pagineEndemic Infusate Contamination and Related BactereFania SalsabillaNessuna valutazione finora
- Ambedkar University Delhi School of Business, Public Policy and Social EntrepreneurshipDocumento11 pagineAmbedkar University Delhi School of Business, Public Policy and Social EntrepreneurshipSakshi AggarwalNessuna valutazione finora
- Labcomp FDocumento23 pagineLabcomp Fking peaceNessuna valutazione finora
- MudWatt SubModule1Documento23 pagineMudWatt SubModule1Guaracyara Ribas AugustoNessuna valutazione finora
- Rainsure Company, Instrument and Assays Introduction CLVDocumento61 pagineRainsure Company, Instrument and Assays Introduction CLVMohammed H. KeshtaNessuna valutazione finora
- The Eukaryotic Replication Machine: D. Zhang, M. O'DonnellDocumento39 pagineThe Eukaryotic Replication Machine: D. Zhang, M. O'DonnellÁgnes TóthNessuna valutazione finora
- Bio Viva QuestionsDocumento5 pagineBio Viva QuestionsJaefar ShameemNessuna valutazione finora
- International Journal of Infectious DiseasesDocumento3 pagineInternational Journal of Infectious DiseasesDetti FahmiasyariNessuna valutazione finora
- Anatomy of Stomach and Duodenum. Physiology of Gastric Secretion. Pathophysiology of Acute and Chronic UlcerDocumento6 pagineAnatomy of Stomach and Duodenum. Physiology of Gastric Secretion. Pathophysiology of Acute and Chronic UlcerMarin VozianNessuna valutazione finora
- Cancer Therapy: PreclinicalDocumento8 pagineCancer Therapy: PreclinicalGeorge GeorgakisNessuna valutazione finora
- Vet Comparative Oncology - 2022 - Harris - Using Digital RNA Counting To Establish Flow Cytometry Diagnostic Criteria ForDocumento10 pagineVet Comparative Oncology - 2022 - Harris - Using Digital RNA Counting To Establish Flow Cytometry Diagnostic Criteria Formarta idziakNessuna valutazione finora
- 1 s2.0 S0042682214002293 MainDocumento14 pagine1 s2.0 S0042682214002293 MainNouri RaidNessuna valutazione finora
- Virus StructureDocumento2 pagineVirus Structurewakadur RahmanNessuna valutazione finora