Potrebbero piacerti anche
- Hypoglycemia, A Simple Guide To The Condition, Treatment And Related ConditionsDa EverandHypoglycemia, A Simple Guide To The Condition, Treatment And Related ConditionsNessuna valutazione finora
- Guideline HHS or Honk in AdultDocumento7 pagineGuideline HHS or Honk in AdultCarolina NauNessuna valutazione finora
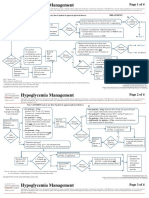
- Clin Management Hypoglycemia Web AlgorithmDocumento4 pagineClin Management Hypoglycemia Web AlgorithmannaNessuna valutazione finora
- Hypoglycemia Management: Page 1 of 4Documento4 pagineHypoglycemia Management: Page 1 of 4sidharth sauravNessuna valutazione finora
- Diabetic Ketoacidosis Pathophysiology, Assessment, TreatmentDocumento1 paginaDiabetic Ketoacidosis Pathophysiology, Assessment, TreatmentZunaira AliNessuna valutazione finora
- Potassium Chloride Drug OverviewDocumento2 paginePotassium Chloride Drug OverviewmichelleNessuna valutazione finora
- DiureticsDocumento5 pagineDiureticsUsmanNessuna valutazione finora
- Pediatric Diabetic Ketoacidosis (DKA) Algorithm (Page 1-ED) : DKA Diagnosed DKA Not DiagnosedDocumento2 paginePediatric Diabetic Ketoacidosis (DKA) Algorithm (Page 1-ED) : DKA Diagnosed DKA Not Diagnosedrolland_arrizaNessuna valutazione finora
- Drugstudy CalciumcarbonateDocumento3 pagineDrugstudy Calciumcarbonateduane27fronterasNessuna valutazione finora
- DKA Guidelines Version 4.0 28 Dec 2016FINALDocumento4 pagineDKA Guidelines Version 4.0 28 Dec 2016FINALbenNessuna valutazione finora
- Family Wellness PlanDocumento7 pagineFamily Wellness PlanGlenn Anthony Dela CruzNessuna valutazione finora
- DkaDocumento32 pagineDkanatheNessuna valutazione finora
- JBDS 02 Single Page Pathway Amended June 2021Documento2 pagineJBDS 02 Single Page Pathway Amended June 2021Oliverio MéndezNessuna valutazione finora
- Adult Diabetic Emergencies Care ProtocolDocumento4 pagineAdult Diabetic Emergencies Care ProtocolvladhdNessuna valutazione finora
- DKA Protocol With Calculation SheetDocumento7 pagineDKA Protocol With Calculation SheetAmanda Marie Best OsbourneNessuna valutazione finora
- Pediatric Anesthesiology: James Gordon Cain, M.DDocumento60 paginePediatric Anesthesiology: James Gordon Cain, M.DMesayu Nadya PrameswariNessuna valutazione finora
- The Neonatal Intensive Care Unit-2Documento28 pagineThe Neonatal Intensive Care Unit-2api-457873289Nessuna valutazione finora
- Archer Rapid Review Nclex SylabusDocumento9 pagineArcher Rapid Review Nclex SylabusMariaNessuna valutazione finora
- Mini Case Presentation SlidesDocumento21 pagineMini Case Presentation Slidesapi-640180401Nessuna valutazione finora
- Go KCLDocumento7 pagineGo KCLSAMANTHA T. MODESTONessuna valutazione finora
- Bsped Dka Guidelines 2020Documento23 pagineBsped Dka Guidelines 2020drsaleemNessuna valutazione finora
- HAC BrochureDocumento5 pagineHAC BrochureTanzir Bin Razzaque 1831914042Nessuna valutazione finora
- Guidelines Steroid Use CancerDocumento3 pagineGuidelines Steroid Use CancerAsh mohamedNessuna valutazione finora
- British Guide Algoritmo CetoacidosisDocumento2 pagineBritish Guide Algoritmo CetoacidosisMon GuevaraNessuna valutazione finora
- QR Management of Type 2 Diabetes Mellitus (5th Edition) PDFDocumento8 pagineQR Management of Type 2 Diabetes Mellitus (5th Edition) PDFKai Xin100% (1)
- CPG Diabetic NephropathyDocumento23 pagineCPG Diabetic NephropathyapalaginihNessuna valutazione finora
- Diabetic Care in Acute Febrile IllnessDocumento27 pagineDiabetic Care in Acute Febrile IllnessDr-Ajay TripathiNessuna valutazione finora
- TDH Drugstdy 1Documento6 pagineTDH Drugstdy 1Rhea Grace GelleNessuna valutazione finora
- DrugDocumento16 pagineDrugtrofacir100% (3)
- Bsped Dka Guideline 2020Documento24 pagineBsped Dka Guideline 2020Valentina Jiménez CárdenasNessuna valutazione finora
- Pharma ReviewerDocumento74 paginePharma ReviewerSamantha DiegoNessuna valutazione finora
- Case Based Learning Renal and EndocrineDocumento38 pagineCase Based Learning Renal and EndocrineSyeren VenesiaNessuna valutazione finora
- ASSESSMENT OF 11 HEALTH PATTERNSDocumento10 pagineASSESSMENT OF 11 HEALTH PATTERNSMa. Ferimi Gleam BajadoNessuna valutazione finora
- Dka AlgorithmDocumento1 paginaDka AlgorithmAbhinav AggarwalNessuna valutazione finora
- 16-K-Ca ImbalanceDocumento11 pagine16-K-Ca Imbalanceمصطفى محمد جواد كاظمNessuna valutazione finora
- EndocrineDocumento10 pagineEndocrineSanjie EufracioNessuna valutazione finora
- Flow Chart For Diabetic Ketoacidosis in Adults Management ofDocumento1 paginaFlow Chart For Diabetic Ketoacidosis in Adults Management ofsheryl maeNessuna valutazione finora
- Diabetic Ketoacidosis: Clinical Features and Management: - DR Sanjay Kalra, D.M. (Aiims)Documento26 pagineDiabetic Ketoacidosis: Clinical Features and Management: - DR Sanjay Kalra, D.M. (Aiims)Siti RahmahNessuna valutazione finora
- Massive Haemorrhage Protocol (MHP) : Lead Clinician Activates MHPDocumento1 paginaMassive Haemorrhage Protocol (MHP) : Lead Clinician Activates MHPonlyhamsterNessuna valutazione finora
- Aag Drug StudyDocumento7 pagineAag Drug StudyAudrie Allyson GabalesNessuna valutazione finora
- Drug Study Form 2Documento4 pagineDrug Study Form 2luiNessuna valutazione finora
- CH 51 Diuretic AgentsDocumento4 pagineCH 51 Diuretic Agentsericka abasNessuna valutazione finora
- ArcherReview NCLEX Rapid Prep CourseDocumento8 pagineArcherReview NCLEX Rapid Prep CourseLevy Melgarejo60% (5)
- Chronic Kidney DiseaseDocumento17 pagineChronic Kidney DiseaseJuanchi INNessuna valutazione finora
- Metabolic Disorders LONG CHAIN FAT OXIDATION DISORDERSDocumento5 pagineMetabolic Disorders LONG CHAIN FAT OXIDATION DISORDERSMahmoud khedrNessuna valutazione finora
- CCS Cases NotesDocumento12 pagineCCS Cases NotesMandeepNessuna valutazione finora
- Management of Type 2 Diabetes Mellitus: Quick Reference Guide For Healthcare ProfessionalsDocumento8 pagineManagement of Type 2 Diabetes Mellitus: Quick Reference Guide For Healthcare ProfessionalsAqilah SyafiqahNessuna valutazione finora
- Drugs For Diabetes PDFDocumento4 pagineDrugs For Diabetes PDFDylan RastoNessuna valutazione finora
- Drug-study-OmeprazoleDocumento2 pagineDrug-study-OmeprazolemaxynezolayvarNessuna valutazione finora
- Pancreatic Enzymes Help Digest CarbsDocumento7 paginePancreatic Enzymes Help Digest CarbsAngelaAmmcoNessuna valutazione finora
- G HieDocumento34 pagineG HieBia BarridoNessuna valutazione finora
- MGT of D KetoacidosisDocumento5 pagineMGT of D Ketoacidosisshabatat2002Nessuna valutazione finora
- grand rounds diabetic ketoacidosis diseaseDocumento52 paginegrand rounds diabetic ketoacidosis diseaseapi-740259455Nessuna valutazione finora
- Acute Hyperkalaemia in AdultsDocumento12 pagineAcute Hyperkalaemia in AdultsMeilina FitrianiNessuna valutazione finora
- Contact Details Name: Hospital Telephone:: Treatment Is Urgent. Do Not DelayDocumento4 pagineContact Details Name: Hospital Telephone:: Treatment Is Urgent. Do Not DelayCaterina PrepelitaNessuna valutazione finora
- In Primary Care: Chronic Kidney Disease (CKD)Documento4 pagineIn Primary Care: Chronic Kidney Disease (CKD)NotForAbuseNessuna valutazione finora
- Treating Canine Diabetic KetoacidosisDocumento3 pagineTreating Canine Diabetic KetoacidosisPetrisor GheorghiuNessuna valutazione finora
- Insulin Algorithm For Type 2 Diabetes in Children and AdultsDocumento6 pagineInsulin Algorithm For Type 2 Diabetes in Children and AdultsOlesiaNessuna valutazione finora
- Joint British Diabetes Societies Inpatient Care Group - The Management of Diabetic Ketoacidosis in Adults - Pathway PosterDocumento1 paginaJoint British Diabetes Societies Inpatient Care Group - The Management of Diabetic Ketoacidosis in Adults - Pathway PosterAllison Nadine MarchandNessuna valutazione finora
- SnakebiteDocumento4 pagineSnakebiteDitha DaraPrimadithaNessuna valutazione finora
- Neurotoxic Snake Bite PoisoningDocumento3 pagineNeurotoxic Snake Bite PoisoningChoirotun HisanNessuna valutazione finora
- Sepsis Syndrome Paper PublishedDocumento6 pagineSepsis Syndrome Paper PublishedChoirotun HisanNessuna valutazione finora
- Journal of Pediatric Gastroenterology & Nutrition Volume 64 Issue 5 2017 (Doi 10.1097/MPG.0000000000001451) Dogra, Shivani Thakur, Anup Garg, Pankaj Kler, Neelam - Effect of Differential EnteralDocumento7 pagineJournal of Pediatric Gastroenterology & Nutrition Volume 64 Issue 5 2017 (Doi 10.1097/MPG.0000000000001451) Dogra, Shivani Thakur, Anup Garg, Pankaj Kler, Neelam - Effect of Differential EnteralChoirotun HisanNessuna valutazione finora
- Sepsis Syndrome Paper PublishedDocumento6 pagineSepsis Syndrome Paper PublishedChoirotun HisanNessuna valutazione finora
- Jurnal Treatment Impetigo Dan EktimaDocumento5 pagineJurnal Treatment Impetigo Dan EktimaChoirotun HisanNessuna valutazione finora
- Cureus 0009 00000001588 PDFDocumento4 pagineCureus 0009 00000001588 PDFChoirotun HisanNessuna valutazione finora
- Ludwig's Angina 2Documento4 pagineLudwig's Angina 2SuryaAtmajayaNessuna valutazione finora
- Long-Term Effect of Exercise Therapy and Patient Education On Impairments and Activity Limitations in People With Hip Osteoarthritis Secondary Outcome Analysis of A Randomized Clinical TrialDocumento11 pagineLong-Term Effect of Exercise Therapy and Patient Education On Impairments and Activity Limitations in People With Hip Osteoarthritis Secondary Outcome Analysis of A Randomized Clinical TrialChoirotun HisanNessuna valutazione finora
- Effects of Exercise Programmes On Quality of Life in Osteoporotic and Osteopenic Postmenopausal Women A Systematic Review and Meta-AnalysisDocumento10 pagineEffects of Exercise Programmes On Quality of Life in Osteoporotic and Osteopenic Postmenopausal Women A Systematic Review and Meta-AnalysisChoirotun HisanNessuna valutazione finora
- Impact of Cane Use On Pain, Function, General Health and Energy Expenditure During Gait in Patients With Knee Osteoarthritis A Randomised Controlled TrialDocumento8 pagineImpact of Cane Use On Pain, Function, General Health and Energy Expenditure During Gait in Patients With Knee Osteoarthritis A Randomised Controlled TrialChoirotun HisanNessuna valutazione finora
- NCM 100 H.A Procedure DPPER 3Documento51 pagineNCM 100 H.A Procedure DPPER 3Richelle Joy Durano RegatunaNessuna valutazione finora
- Tetanus Neonatorum LectureDocumento11 pagineTetanus Neonatorum LectureJackNessuna valutazione finora
- Prokaryotes and Eukaryotes: Strategies and Successes: Michael CarlileDocumento3 pagineProkaryotes and Eukaryotes: Strategies and Successes: Michael CarlileNurul ShazwaniNessuna valutazione finora
- Aids 2013Documento404 pagineAids 2013kovaron80Nessuna valutazione finora
- Movement Disorders Movement DisordersDocumento32 pagineMovement Disorders Movement Disordersreddyrajiv1526Nessuna valutazione finora
- Identification of BacteriaDocumento4 pagineIdentification of BacteriaVasugiNessuna valutazione finora
- Led Light Therapy GuideDocumento23 pagineLed Light Therapy GuidePeter Freimann100% (4)
- Vacuole FunctionDocumento8 pagineVacuole Functionkbansal981Nessuna valutazione finora
- Paragraph Development ExerciseDocumento6 pagineParagraph Development ExerciseSYAFINAS SALAM100% (1)
- Chlorhexidine - An Antiseptic in PeriodonticsDocumento4 pagineChlorhexidine - An Antiseptic in PeriodonticsInternational Organization of Scientific Research (IOSR)Nessuna valutazione finora
- Lecture 8 - 30.12.2022Documento17 pagineLecture 8 - 30.12.2022Adnan Mohammad Adnan HailatNessuna valutazione finora
- 201305283en Capsurefix 5076Documento2 pagine201305283en Capsurefix 5076Bian PurwaNessuna valutazione finora
- Template POMRDocumento8 pagineTemplate POMRPPDS IPD ULMNessuna valutazione finora
- Blood Buffer SystemDocumento10 pagineBlood Buffer Systemmd hasib munsiNessuna valutazione finora
- NCP of CavDocumento3 pagineNCP of CavHenry Roque TagalagNessuna valutazione finora
- Zoology: Zoology Previous Eamcet QuestionsDocumento8 pagineZoology: Zoology Previous Eamcet QuestionsGaganpreetSingh100% (1)
- A Kinesiological Analysis of Shot BY WILLISDocumento16 pagineA Kinesiological Analysis of Shot BY WILLISNoraina AbdullahNessuna valutazione finora
- Modul Anatomi Blok 7Documento27 pagineModul Anatomi Blok 7Dewandaru I A BNessuna valutazione finora
- COPING WITH STRESSDocumento16 pagineCOPING WITH STRESSDionisius KevinNessuna valutazione finora
- Excretory System QuizDocumento17 pagineExcretory System QuizShadab HanafiNessuna valutazione finora
- Rate and RhythmDocumento10 pagineRate and RhythmSamanta Luiza de AraujoNessuna valutazione finora
- Metabolism of DisaccharidesDocumento15 pagineMetabolism of DisaccharidesminaNessuna valutazione finora
- Abdominal SurgeryDocumento166 pagineAbdominal SurgeryIndera VyasNessuna valutazione finora
- Wound CareDocumento14 pagineWound CareKirsten Padilla Chua100% (4)
- Anatomy and Physiology-REVIEWER-Practical ExamDocumento12 pagineAnatomy and Physiology-REVIEWER-Practical ExamDeity Ann ReuterezNessuna valutazione finora
- Mobilization NotesDocumento239 pagineMobilization NotesSuganya Balachandran100% (6)
- Chronic Kidney Disease : Hypertensive and Diabetic Retinopathy in PatientsDocumento7 pagineChronic Kidney Disease : Hypertensive and Diabetic Retinopathy in PatientsAnonymous FgT04krgymNessuna valutazione finora
- The Third International Consensus Definitions For Sepsis and Septic Shock Sepsis-3 - JAMA 2016Documento10 pagineThe Third International Consensus Definitions For Sepsis and Septic Shock Sepsis-3 - JAMA 2016Miguel Angel Quiroz CristobalNessuna valutazione finora
- Worksheet: I) Ii) Iii)Documento4 pagineWorksheet: I) Ii) Iii)Jin MingNessuna valutazione finora