Potrebbero piacerti anche
- Toxin-Inducedacute Delirium: Alice Cai,, Xuemei CaiDocumento18 pagineToxin-Inducedacute Delirium: Alice Cai,, Xuemei CaiVivi DeviyanaNessuna valutazione finora
- 10 - Disorders of Consciousness and Language I (Coma and Confusional States) LectureDocumento119 pagine10 - Disorders of Consciousness and Language I (Coma and Confusional States) LectureRanjit SharmaNessuna valutazione finora
- Approach To AMSDocumento26 pagineApproach To AMSAmal HashimNessuna valutazione finora
- 10-10-2017 Sindroma Delirium Neuro. DR Hadi SP.SDocumento21 pagine10-10-2017 Sindroma Delirium Neuro. DR Hadi SP.SSaski salsaaNessuna valutazione finora
- Alzheimers DiseaseDocumento11 pagineAlzheimers DiseaseCHRISTIAN RAY ALPAS PASILIAONessuna valutazione finora
- 10-10-2017 Sindroma Delirium Neuro. DR Hadi SP.SDocumento21 pagine10-10-2017 Sindroma Delirium Neuro. DR Hadi SP.SSaski salsaaNessuna valutazione finora
- Metabolic Coma DRDocumento32 pagineMetabolic Coma DRKintan UtamiNessuna valutazione finora
- Dr. Hadi Widjaja, Mbiomed, Sps Neurologist - Siloam Hospital KupangDocumento23 pagineDr. Hadi Widjaja, Mbiomed, Sps Neurologist - Siloam Hospital KupangChrysthien MarumataNessuna valutazione finora
- Ischemic Stroke: The Normal Blood Supply To The Brain Is DisruptedDocumento5 pagineIschemic Stroke: The Normal Blood Supply To The Brain Is DisruptedMelchora Lea Castro SorianoNessuna valutazione finora
- Neurology MnemonicsDocumento11 pagineNeurology MnemonicsOstaz100% (1)
- Seizure PathophysiologyDocumento3 pagineSeizure PathophysiologyPaula Nantes Nazareth55% (11)
- Metabolik EncelophatyDocumento8 pagineMetabolik EncelophatyfkiaNessuna valutazione finora
- UnconsciousnessDocumento80 pagineUnconsciousnessDivya SomanNessuna valutazione finora
- Cognitive Disorders: P.Tembo Mental HealthDocumento17 pagineCognitive Disorders: P.Tembo Mental HealthGift MwapeNessuna valutazione finora
- Neurological Coma: Zainuddin Arpandy, SP.S Neurology Department of Ulin Hospital BanjarmasinDocumento24 pagineNeurological Coma: Zainuddin Arpandy, SP.S Neurology Department of Ulin Hospital BanjarmasinDwi Rezky AmaliaNessuna valutazione finora
- Step 2 CS Differential DiagnosesDocumento4 pagineStep 2 CS Differential DiagnosesnaimNessuna valutazione finora
- Approach To Unconsious PTDocumento62 pagineApproach To Unconsious PTHussain AzharNessuna valutazione finora
- COMA Dan Penurunan KesadaranDocumento40 pagineCOMA Dan Penurunan KesadaranAhmad Shafwan NatsirNessuna valutazione finora
- Metabolic EncephalopathiesDocumento10 pagineMetabolic EncephalopathiesSrinath M VNessuna valutazione finora
- Uremic EncephalophatyDocumento48 pagineUremic EncephalophatySindi LadayaNessuna valutazione finora
- Alhkohol PDFDocumento11 pagineAlhkohol PDFNurmawati AtNessuna valutazione finora
- Coma 1n Infancy and Childhood: Neurology, of of VirginiaDocumento4 pagineComa 1n Infancy and Childhood: Neurology, of of VirginiaAya YokaNessuna valutazione finora
- Examination of The Comatose PatientDocumento9 pagineExamination of The Comatose Patientakrw90Nessuna valutazione finora
- DementiaDocumento38 pagineDementiarajikakurupNessuna valutazione finora
- Seizure-Case StudyDocumento6 pagineSeizure-Case StudyELaine ELena TiongsonNessuna valutazione finora
- Stroke Syndromes and Localization 2007Documento56 pagineStroke Syndromes and Localization 2007SaintPaul Univ100% (1)
- 8) Delirium and AMS - dc.9.2.16Documento54 pagine8) Delirium and AMS - dc.9.2.16Jade LoberianoNessuna valutazione finora
- 1n2 OrganicSD-drshakyaDocumento26 pagine1n2 OrganicSD-drshakyaUMESH KANDELNessuna valutazione finora
- CollapseDocumento46 pagineCollapseChananNessuna valutazione finora
- Peripheral Neuropathy: By: R'Syah ESI NeurologistDocumento39 paginePeripheral Neuropathy: By: R'Syah ESI Neurologistraynhard b. fandres100% (2)
- Monic 2Documento106 pagineMonic 2Life PediaNessuna valutazione finora
- Unit 3 Nervous SystemDocumento58 pagineUnit 3 Nervous SystemdhanashriNessuna valutazione finora
- Cerebral Calcifications As A Differential Diagnosis of Psychiatric DisordersDocumento17 pagineCerebral Calcifications As A Differential Diagnosis of Psychiatric DisordersMurillo NevesNessuna valutazione finora
- II-E Altered PerceptionDocumento16 pagineII-E Altered PerceptionDharylle CariñoNessuna valutazione finora
- Assessment & Specific Managements: Alcohol UseDocumento34 pagineAssessment & Specific Managements: Alcohol UseChris Jardine LiNessuna valutazione finora
- Hypoxia Ischemic Encephalopathy and Congenital AnomaliesDocumento36 pagineHypoxia Ischemic Encephalopathy and Congenital AnomaliesVarna MohanNessuna valutazione finora
- Module 2 - Acute Non Traumatic WeaknessDocumento55 pagineModule 2 - Acute Non Traumatic WeaknessRick RanitNessuna valutazione finora
- Chorea in Children: Etiology, Diagnostic Approach and ManagementDocumento20 pagineChorea in Children: Etiology, Diagnostic Approach and ManagementArepalli Santhosh100% (1)
- EpilepsyDocumento37 pagineEpilepsyMakojoa KatisoNessuna valutazione finora
- Definitions and Descriptions of Altered Mental StatusDocumento6 pagineDefinitions and Descriptions of Altered Mental StatusMicah LatosaNessuna valutazione finora
- Subarachnoid HemorrhageDocumento2 pagineSubarachnoid Hemorrhagevfsqp9zxgqNessuna valutazione finora
- Epilepsy-Students 2016Documento85 pagineEpilepsy-Students 2016Alberto MayorgaNessuna valutazione finora
- Seizure Disorders and Management in Primary Health CareDocumento83 pagineSeizure Disorders and Management in Primary Health CareChidi MbatuegwuNessuna valutazione finora
- Ataxia PresentationDocumento11 pagineAtaxia PresentationS RiarNessuna valutazione finora
- Arbd Feb 2023Documento25 pagineArbd Feb 2023S. LeighNessuna valutazione finora
- Acute ComaDocumento16 pagineAcute ComaDean AccountNessuna valutazione finora
- Initial Diagnosis and Management of ComaDocumento17 pagineInitial Diagnosis and Management of Comaguugle gogleNessuna valutazione finora
- 2n2 OrganicSD-drshakyaDocumento20 pagine2n2 OrganicSD-drshakyaUMESH KANDELNessuna valutazione finora
- Confusion MetabolicDocumento43 pagineConfusion MetabolicYoumna ShaabanNessuna valutazione finora
- Metabolic Encephalopathy and Metabolic ComaDocumento14 pagineMetabolic Encephalopathy and Metabolic ComaqlinlynNessuna valutazione finora
- TBI ZamDocumento67 pagineTBI ZamnafisyarifahNessuna valutazione finora
- NCM 116: Neurologic Dysfunctions: Joyce Bernadette P. Andot - Anna Delle Nicole P. Aranding, BSN-IIIDocumento46 pagineNCM 116: Neurologic Dysfunctions: Joyce Bernadette P. Andot - Anna Delle Nicole P. Aranding, BSN-IIIMercy Anne EcatNessuna valutazione finora
- Perinatal Asphyxia - Outline of Pathophysiology and Recent Trends in ManagementDocumento31 paginePerinatal Asphyxia - Outline of Pathophysiology and Recent Trends in Managementokwadha simionNessuna valutazione finora
- Epilepsy PD 501Documento30 pagineEpilepsy PD 501Amna LuqmanNessuna valutazione finora
- Disorders of Autonomic Nervous System: Chair PersonsDocumento37 pagineDisorders of Autonomic Nervous System: Chair PersonswarunkumarNessuna valutazione finora
- 002 - Cerebellum PDFDocumento45 pagine002 - Cerebellum PDFLucas Victor AlmeidaNessuna valutazione finora
- Endocrine Disorders and The Neurologic ManifestationsDocumento49 pagineEndocrine Disorders and The Neurologic ManifestationsRahmawati HamudiNessuna valutazione finora
- Epilepsy 1Documento51 pagineEpilepsy 1Deepa SeiraNessuna valutazione finora
- Hypocalcemia - Diagnosis and Treatment - Endotext - NCBI BookshelfDocumento31 pagineHypocalcemia - Diagnosis and Treatment - Endotext - NCBI Bookshelfgalnaresdaniela7Nessuna valutazione finora
- Evaluation and Treatment of Urinary Incontinence in WomenDocumento1 paginaEvaluation and Treatment of Urinary Incontinence in Womenizzati94Nessuna valutazione finora
- Rogers2019 Article RiskOverdiagnosisAndEthicalJusDocumento18 pagineRogers2019 Article RiskOverdiagnosisAndEthicalJusizzati94Nessuna valutazione finora
- DonotcrushDocumento16 pagineDonotcrushapi-278913876Nessuna valutazione finora
- Antibiotic Cross-Sensitivity Chart PDFDocumento1 paginaAntibiotic Cross-Sensitivity Chart PDFanareadsNessuna valutazione finora
- 2012 Guía para El Manejo de HipotiroidismoDocumento36 pagine2012 Guía para El Manejo de Hipotiroidismomod_naiveNessuna valutazione finora
- Suspected Stroke: Clinical Management Guideline ForDocumento1 paginaSuspected Stroke: Clinical Management Guideline Forizzati94Nessuna valutazione finora
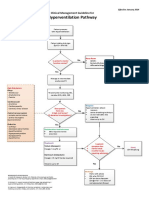
- Hyperventilation CMGDocumento1 paginaHyperventilation CMGizzati94Nessuna valutazione finora
- EE1108 Exercise 2 AnswersDocumento8 pagineEE1108 Exercise 2 Answersizzati94Nessuna valutazione finora
- EG1108 Handout 3-03 (Stored Energy in Capacitor)Documento1 paginaEG1108 Handout 3-03 (Stored Energy in Capacitor)izzati94Nessuna valutazione finora
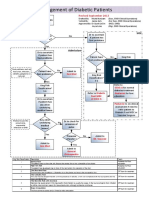
- Management of Diabetic Foot PatientsDocumento1 paginaManagement of Diabetic Foot Patientsizzati94Nessuna valutazione finora
- Appendix A: Review of Complex NumbersDocumento10 pagineAppendix A: Review of Complex Numbersizzati94Nessuna valutazione finora
- EggsDocumento1 paginaEggsizzati94Nessuna valutazione finora
- URTI (Objectives and Readings)Documento1 paginaURTI (Objectives and Readings)izzati94Nessuna valutazione finora
- New Century Health Clinic Ch.4Documento2 pagineNew Century Health Clinic Ch.4Natasha Rahman0% (2)
- Gestational Diabetes Mellitus: Science in MedicineDocumento7 pagineGestational Diabetes Mellitus: Science in MedicinerizqarrNessuna valutazione finora
- Cdi7 Week 3Documento1 paginaCdi7 Week 3Roger GAMINGNessuna valutazione finora
- MPDS Codes PDFDocumento19 pagineMPDS Codes PDFjared999Nessuna valutazione finora
- Chest Physiotherapy For Pneumonia in ChildrenDocumento30 pagineChest Physiotherapy For Pneumonia in ChildrenristaseptiawatiningsihNessuna valutazione finora
- Entrevista BjornDocumento11 pagineEntrevista BjornMirza GlusacNessuna valutazione finora
- Meropenem Drug StudyDocumento2 pagineMeropenem Drug StudyKullin Rain100% (1)
- Tarah Viviano Revised Resume 2016Documento2 pagineTarah Viviano Revised Resume 2016api-314537209Nessuna valutazione finora
- Exodontia PedodonticsDocumento35 pagineExodontia PedodonticsFourthMolar.comNessuna valutazione finora
- Gestational DiabetesDocumento42 pagineGestational Diabetesjohn jumborock100% (1)
- PDEA S Register 2-14 FormDocumento12 paginePDEA S Register 2-14 FormAngelito BALUYOT JRNessuna valutazione finora
- Cdem 17march WebDocumento24 pagineCdem 17march WebRicardo Jonathan Ayala GarciaNessuna valutazione finora
- DR Ahamad Hassan Stroke MimicsDocumento23 pagineDR Ahamad Hassan Stroke MimicskselvieNessuna valutazione finora
- BSC Nursing: Medical Surgical Nursing - I Unit V - Disorders of The Cardio Vascular SystemDocumento36 pagineBSC Nursing: Medical Surgical Nursing - I Unit V - Disorders of The Cardio Vascular SystemPoova RagavanNessuna valutazione finora
- Basic Life Support (BLS)Documento49 pagineBasic Life Support (BLS)Sukhbir KaurNessuna valutazione finora
- Recommended Procedures For Doctors and Nurse in The Management of Kawasaki DiseaseDocumento34 pagineRecommended Procedures For Doctors and Nurse in The Management of Kawasaki DiseaseJOSHUA DICHOSONessuna valutazione finora
- Cattle Diseases Farmers GuideDocumento77 pagineCattle Diseases Farmers GuideDivyajyoti DevaNessuna valutazione finora
- RH IncompatibilityDocumento3 pagineRH IncompatibilityMima Fatimah LuthfieNessuna valutazione finora
- Cleaning and Disinfecting Hemodialysis Machines and StationsDocumento14 pagineCleaning and Disinfecting Hemodialysis Machines and Stationsarun melepurackalNessuna valutazione finora
- Oral Lymphoma PDFDocumento11 pagineOral Lymphoma PDFIcha Aisya AisyaNessuna valutazione finora
- DesenteryDocumento3 pagineDesenteryAby Gift AnnNessuna valutazione finora
- Curriculum Vitae2011Documento2 pagineCurriculum Vitae2011Rafik MargaryanNessuna valutazione finora
- Factors in The Relationship Between Epilepsy and Behavioral DisordersDocumento19 pagineFactors in The Relationship Between Epilepsy and Behavioral DisordersEdya YopiNessuna valutazione finora
- Patient Safety: An Introduction: Jhessie L. Abella, RN, RM, MAN, CpsoDocumento22 paginePatient Safety: An Introduction: Jhessie L. Abella, RN, RM, MAN, Cpsoprinsepejesse100% (1)
- Case Report Rehabilitation Program in A Patient With Bilateral Arthroplasty For Hip OsteoarthritisDocumento26 pagineCase Report Rehabilitation Program in A Patient With Bilateral Arthroplasty For Hip OsteoarthritisNatalia LoredanaNessuna valutazione finora
- LidocaineDocumento4 pagineLidocaineAhmad Fauzi100% (1)
- EC Certificate - Production Quality Assurance EC Certificate - Production Quality AssuranceDocumento6 pagineEC Certificate - Production Quality Assurance EC Certificate - Production Quality AssuranceEngr Hamid AliNessuna valutazione finora
- MAPEH 7 Q4 Week 4Documento9 pagineMAPEH 7 Q4 Week 4Maricris ArsibalNessuna valutazione finora
- Comprehensive Clinical Nephrology 7th Edition AL Grawany 2024Documento1.547 pagineComprehensive Clinical Nephrology 7th Edition AL Grawany 2024rozhansedikNessuna valutazione finora
- Joe Dispenza You Are The Placebo PDF 21Documento4 pagineJoe Dispenza You Are The Placebo PDF 21Humaidhan0% (2)
- The Age of Magical Overthinking: Notes on Modern IrrationalityDa EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityValutazione: 4 su 5 stelle4/5 (29)
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDDa EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDValutazione: 5 su 5 stelle5/5 (2)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsDa EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNessuna valutazione finora
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionDa EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionValutazione: 4 su 5 stelle4/5 (404)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedDa EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedValutazione: 5 su 5 stelle5/5 (81)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsDa EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsValutazione: 3.5 su 5 stelle3.5/5 (3)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsDa EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsValutazione: 4.5 su 5 stelle4.5/5 (170)
- Love Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)Da EverandLove Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)Nessuna valutazione finora
- The Obesity Code: Unlocking the Secrets of Weight LossDa EverandThe Obesity Code: Unlocking the Secrets of Weight LossValutazione: 4 su 5 stelle4/5 (6)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsDa EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsValutazione: 5 su 5 stelle5/5 (1)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeDa EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeValutazione: 2 su 5 stelle2/5 (1)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisDa EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisValutazione: 4.5 su 5 stelle4.5/5 (42)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessDa EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessValutazione: 4.5 su 5 stelle4.5/5 (328)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisDa EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisValutazione: 4 su 5 stelle4/5 (1)
- Why We Die: The New Science of Aging and the Quest for ImmortalityDa EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityValutazione: 4 su 5 stelle4/5 (4)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Da EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Valutazione: 4.5 su 5 stelle4.5/5 (110)
- Summary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisDa EverandSummary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisValutazione: 5 su 5 stelle5/5 (8)
- To Explain the World: The Discovery of Modern ScienceDa EverandTo Explain the World: The Discovery of Modern ScienceValutazione: 3.5 su 5 stelle3.5/5 (51)
- When the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisDa EverandWhen the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisValutazione: 3.5 su 5 stelle3.5/5 (2)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaDa EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaValutazione: 4.5 su 5 stelle4.5/5 (266)
- The Marshmallow Test: Mastering Self-ControlDa EverandThe Marshmallow Test: Mastering Self-ControlValutazione: 4.5 su 5 stelle4.5/5 (58)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryDa EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryValutazione: 4 su 5 stelle4/5 (45)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeDa EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeValutazione: 4.5 su 5 stelle4.5/5 (253)