Documenti di Didattica
Documenti di Professioni
Documenti di Cultura
Impact of climate change on global malaria distribution
Caricato da
Anggitya PratiwiTitolo originale
Copyright
Formati disponibili
Condividi questo documento
Condividi o incorpora il documento
Hai trovato utile questo documento?
Questo contenuto è inappropriato?
Segnala questo documentoCopyright:
Formati disponibili
Impact of climate change on global malaria distribution
Caricato da
Anggitya PratiwiCopyright:
Formati disponibili
Impact of climate change on global
malaria distribution
Cyril Caminadea,b,1, Sari Kovatsc, Joacim Rocklovd, Adrian M. Tompkinse, Andrew P. Morseb, Felipe J. Colón-Gonzáleze,
Hans Stenlundd, Pim Martensf, and Simon J. Lloydc
a
Institute of Infection and Global Health, Department of Epidemiology and Population Health and bSchool of Environmental Sciences, Department of
Geography and Planning, University of Liverpool, Liverpool L69 7ZT, United Kingdom; cDepartment of Social and Environmental Health Research, London
School of Hygiene and Tropical Medicine, London WC1E 7HT, United Kingdom; dDepartment of Public Health and Clinical Medicine, Epidemiology and Global
Health, Umea University, 901 87 Umea, Sweden; eAbdus Salam International Centre for Theoretical Physics, I-34151Trieste, Italy; and fMaastricht University,
6211 LK, Maastricht, The Netherlands
Edited by Hans Joachim Schellnhuber, Potsdam Institute for Climate Impact Research, Potsdam, Germany, and approved January 10, 2014 (received for review
January 31, 2013)
Malaria is an important disease that has a global distribution and was achieved in the extratropics (Eurasia, northern America,
significant health burden. The spatial limits of its distribution and most of northern Africa, and Australia) where malaria trans-
seasonal activity are sensitive to climate factors, as well as the mission was highly seasonal owing to temperate climatic con-
local capacity to control the disease. Malaria is also one of the few ditions and mainly caused by P. vivax (4). In the early 1970s
health outcomes that has been modeled by more than one WHO abandoned the idea of malaria elimination in the tropics,
research group and can therefore facilitate the first model in- especially in Africa, owing to deficiencies in local public health
tercomparison for health impacts under a future with climate services and the severity of Plasmodium infections in endemic
change. We used bias-corrected temperature and rainfall simula- areas, and replaced it by a control policy using modern control
tions from the Coupled Model Intercomparison Project Phase 5
measures such as vector control through insecticide spraying, use
of bed nets, systematic early detection and treatment of cases.
climate models to compare the metrics of five statistical and
Between 2000 and 2010 the incidence of malaria has fallen by
dynamical malaria impact models for three future time periods
17% globally and by 33% in the African regions. There were
(2030s, 2050s, and 2080s). We evaluated three malaria outcome
655,000 reported malaria deaths in 2010, of which 86% were of
metrics at global and regional levels: climate suitability, additional children under 5 y of age. In 2010, most of the malaria deaths
population at risk and additional person-months at risk across the occurred in Africa (91% of the global burden) and were due to
model outputs. The malaria projections were based on five P. falciparum (98% of infections), which causes the most severe
different global climate models, each run under four emission clinical form of the disease (5).
scenarios (Representative Concentration Pathways, RCPs) and a Malaria is one of the few climate-sensitive health outcomes
single population projection. We also investigated the model- that has been modeled by more than one research group and can
ing uncertainty associated with future projections of populations therefore facilitate a more thorough assessment of possible cli-
at risk for malaria owing to climate change. Our findings show an mate change effects using a multimodel intercomparison. Several
overall global net increase in climate suitability and a net increase global (6, 7) and regional assessments (8–10) have now been
in the population at risk, but with large uncertainties. The model published using a range of malaria impact models and climate
outputs indicate a net increase in the annual person-months at risk scenarios, but with varying results. Some divergence may be due
when comparing from RCP2.6 to RCP8.5 from the 2050s to the to the malaria modeling approaches used in the earlier studies.
2080s. The malaria outcome metrics were highly sensitive to the Previous discussions of the relative merits of biological versus
choice of malaria impact model, especially over the epidemic empirical statistical models have focused on the incomplete pa-
fringes of the malaria distribution. rameterization of the biological models (11). Conversely, statis-
tical models are unable to completely separate out climate and
nonclimate factors that determine the current distribution of
global climate impacts | disease modeling | uncertainty malaria (6). To facilitate comparison of impacts under a range of
climate scenarios and malaria models, a structure is needed that
H ealth priorities vary between countries and also change sig-
nificantly over time. One of the factors that governments are
concerned with preparing for over decadal timescales is the po-
Significance
tential impact that environmental and climate change may have on
health and welfare (1, 2). These impacts are complex and mul- This study is the first multimalaria model intercomparison ex-
tifaceted and include the potential for changing climate to alter ercise. This is carried out to estimate the impact of future cli-
in both time and space the burden of vector-borne diseases, mate change and population scenarios on malaria transmission
including malaria. at global scale and to provide recommendations for the future.
Malaria causes a significant burden of disease at the global Our results indicate that future climate might become more
and regional level (3). Malaria is a mosquito-borne infectious suitable for malaria transmission in the tropical highland
disease caused by parasitic protozoans of the genus Plasmodium regions. However, other important socioeconomic factors such
(vivax, malariae, ovale, knowlesi, and falciparum) and is trans- as land use change, population growth and urbanization, mi-
mitted by female mosquito vectors of the Anopheles species. The gration changes, and economic development will have to be
spatial limits of the distribution and seasonal activity are sensi- accounted for in further details for future risk assessments.
tive to climate factors, as well as the local capacity to control the
disease. In endemic areas where transmission occurs in regular Author contributions: C.C., S.K., J.R., A.M.T., and A.P.M. designed research; C.C., A.M.T.,
long seasons, fatality rates are highest among children who have and S.J.L. performed research; C.C., A.M.T., F.J.C.-G., H.S., and S.J.L. analyzed data; and
C.C., S.K., J.R., A.M.T., and P.M. wrote the paper.
not yet developed immunity to the disease. In epidemic areas
where malaria transmission occurs in short seasons or sporad- The authors declare no conflict of interest.
ically in the form of epidemics it is likely to cause severe fatalities This article is a PNAS Direct Submission.
in all age categories. Following the Global Malaria eradication 1
To whom correspondence should be addressed. E-mail: Cyril.Caminade@liverpool.ac.uk.
program launched by the World Health Organization (WHO) in This article contains supporting information online at www.pnas.org/lookup/suppl/doi:10.
the 1950s, 79 countries eliminated malaria. Most of this progress 1073/pnas.1302089111/-/DCSupplemental.
3286–3291 | PNAS | March 4, 2014 | vol. 111 | no. 9 www.pnas.org/cgi/doi/10.1073/pnas.1302089111
SPECIAL FEATURE
differentiates variability originating from the different inputs and Climate Change (IPCC) assessment report (19). The LMM_RO,
methods in the impact estimates. MARA, and MIASMA models only allow the investigation of
There are limits to the usefulness of modeling changes in fu- climatic suitability for malaria transmission, whereas the fully
ture malaria distribution owing to anthropogenic climate change dynamical VECTRI model considers the impact of climate,
(11) because important drivers of disease transmission are not surface hydrology, and population densities on malaria distribu-
yet included, such as population and vector movement, tech- tion. The UMEA model considers the impact of the gross domestic
nological development, vector and disease control, urbanization, product per capita in combination with climate and population
and land use change (12). Indeed, all future projections of densities to model endemic malaria distribution. The first aim
malaria in a warmer world need to be put in the context of the is to compare past distributions of malaria using the malaria
observed global decline in the disease over the 20th century, models driven by observed climatic and socioeconomic data with
mainly owing to human interventions (13). “observed” malaria endemicity estimates (which include all poten-
Detailed mapping of current transmission is required for tar- tial climatic and socioeconomic effects on malaria distribu-
geting control measures in the present (14). For climate impacts tion). Given the different designs and parameterizations of the
assessment, however, it is important to understand how the malaria impact models (MIM) as they were originally developed
structure and parameterizations of the individual models account
for different regions and scientific objectives, they might signifi-
for any divergent results and to estimate the relative contribution
of climate effects on malaria with respect to intervention and cantly differ from the observed estimates. We then mapped future
other nonclimate effects to assess confidence in future scenarios. climate-based distributions of malaria and estimated populations
This project is part of the Inter-Sectoral Impact Model In- at risk under the new emissions scenarios accounting for pop-
tercomparison Project collaboration that aims to advance un- ulation growth and estimate the relative uncertainty and its evo-
derstanding of impact models by developing methods for lution in time related to the global MIM, the climate model
intercomparison (15). Quantitative estimates of impacts and uncertainty inherit in the driving GCMs and the emission scenario
uncertainties have been produced for a range of socioeconomic uncertainty from the RCPs. An assessment of the different
outcomes, such as agriculture and water resources. The objective malaria models’ sensitivity to climate change was then carried
of the research was to produce a new set of health global impact out before providing final conclusions (further details about in-
assessments using five malaria models: LMM_RO (16), MIASMA dividual MIM outcome can be found in SI Appendix).
(7), VECTRI (17), UMEA (6), and MARA (18) driven by cli-
mate outputs from five global climate models (GCMs) using the Results
four Representative Concentration Pathways (RCPs) emissions Fig. 1 shows observed and simulated malaria distribution for the
scenarios developed for the fifth Intergovernmental Panel on 1900s and the 2000s at the global scale. Before intervention,
ENVIRONMENTAL
SCIENCES
SUSTAINABILITY
SCIENCE
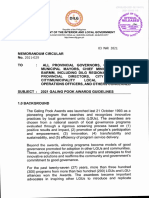
Fig. 1. Observed (A and B) and simulated malaria dis-
tribution (three categories: risk-free in white, unstable/
epidemic in blue, and stable/endemic in red) for five
malaria models (C, D, E, F and G). For the observation
(A and B) all endemic subcategories (hypoendemic,
mesoendemic, hyperendemic, and holoendemic) have
been included in the stable category. The 1900s data
(A) are based on ref. 38 (considers all plasmodium
infections), and the 2000s data (B) are based on ref. 14
(considers only P. falciparum infections). For the simu-
lations, unstable malaria is defined for a length of the
transmission season (LTS) ranging between 1 and 3 mo,
and suitable is defined for LTS above 3 mo (based on
TRMMERAI control runs for the period 1999–2010; SI
Appendix, Fig. S11 shows the CRUTS3.1 control runs).
The TRMMERAI runs are constrained to span 50°N–50°S
owing to the TRMM satellite data availability. For the
UMEA malaria model only estimates of stable malaria
were available.
Caminade et al. PNAS | March 4, 2014 | vol. 111 | no. 9 | 3287
malaria was highly epidemic in north-central Europe, over northern by climate-only parameters need to be put in the context of an
Russia, northern Australia, and in the northeastern United observed decline in malaria endemicity over the 20th century,
States; stable malaria transmission occurred in the Mississippi mainly owing to intervention and related to other socioeconomic
Valley (United States), central and south America, southern factors (SI Appendix, Fig. S1A). The agreement between observed
Africa, India, Malaysia–Indonesia, China, and over a large area and simulated malaria endemicity trends over the 20th century
covering the Middle East and south-central Russia (Fig. 1A). A is restricted to a few regions of Africa (West Africa and a few
similar contemporary map has been produced for the P. falciparum regions over the African highlands) and South America (SI Ap-
parasite (14). Its contemporary distribution is now mainly re- pendix, Fig. S1 B–D vs. A). This does not obviously imply a direct
stricted to the tropics (Fig. 1B), and a large decrease in malaria causality between climate and malaria distribution trends but
endemicity has been observed worldwide, mainly owing to hu- suggests that climate might have partly contributed to the overall
man intervention (13). Malaria has been eliminated in Europe, trends over those regions. Generally, the historical experiments
the United States, Russia, most of China, and Australia and has agree fairly well with the malaria control runs driven by climate
been significantly reduced in Central and South America and observations (SI Appendix, Fig. S2), with a few differences that can
India and, to a lesser extent, over Africa (4). be spotted over India for the HadGem2-ES and IPSLCM5A-LR
Before intervention, the MIASMA model seems to provide experiments, only confirming the validity of the bias correction
the most realistic picture of malaria distribution with respect to technique used with the global climate model data for present-
observations at the global scale (Fig. 1 E vs. A). However, the day conditions.
simulated extension shown over Australia and North America The effect of future climate scenarios on the distribution of
seems relatively unrealistic, and this model does not capture the malaria for all five malaria models is summarized in Fig. 2. The
northward extension over Europe and Russia. This is not sur- maps show changes in the length of the malaria transmission
prising, because all malaria models have been parameterized for season (LTS). Areas where the multimodel agreement is greater
P. falciparum, but the 1900s estimates includes all plasmodium than 60% are hatched. The models show a consistent increase in
species. Stable malaria transmission is consequently restricted to the simulated LTS over the highlands at the regional scale. This
the tropics (Central and South America, Africa, India, Thailand, can be seen over eastern Africa, South Africa, central Angola,
Malaysia, Indonesia, and northern Australia) for the MARA the plateaux of Madagascar, Central America, southern Brazil,
(Fig. 1C), LMM_R0 (Fig. 1D), VECTRI (Fig. 1F), and UMEA eastern Australia, and at the border between India and Nepal.
(Fig. 1G) models during the 2000s. The simulated malaria dis- Conversely, a consistent decrease is shown over tropical regions
tribution patterns are generally consistent with the MAP2007 such as western Africa, the coasts of India, northern Australia,
estimates (14) over the tropics (Fig. 1B) with, however, signifi- Malaysia, and South America. Fig. 3 shows the effect of climate
cant differences per model and per region. All malaria models scenarios on future populations at risk for malaria in Africa. The
simulate endemic malaria transmission over a large area cover- net effect of future climate change (for all emission scenarios) is
ing northern Australia, but malaria has been eradicated in relatively small, with large regional differences. Eastern Africa is
Australia. They also simulate endemic transmission over a large the only region to show significant increases in the person-
area in South America, but this is now restricted to the northern months at risk, but even here the range of results includes some
half of the South American continent. The MARA and VECTRI projections of no net effect. A slight decrease in the population
models provide the most realistic picture for P. falciparum at risk is also shown over western Africa. However, the un-
distribution with respect to the MAP2007 analysis, but they certainty of the malaria modeling method varies greatly in most
generally tend to overestimate malaria endemicity over India, regions (SI Appendix, Fig. S3). A more formal quantification of
Central America, and southern Asia (Laos, Cambodia, Thailand, the future uncertainties was attempted using a linear decompo-
Burma, and southwestern China). The LMM_RO model simu- sition of the variance, and this was displayed as a map for dif-
lates climate to be suitable for P. falciparum transmission in the ferent time slices in the future (SI Appendix, Fig. S4). Generally,
Mississippi Valley (Fig. 1D), and this was observed in the 1900s the largest uncertainties are associated with the methodology
before malaria was eradicated from the North American conti- (e.g., the malaria models used). The uncertainties related to the
nent (Fig. 1A). The results from the malaria impact models driven driving GCMs are large over the northern fringe of the Sahel and
Fig. 2. The effect of climate scenarios on future
malaria distribution: changes in LTS. Each map
shows the results for a different emission scenario
(RCP). The different hues represent change in LTS
between 2069–2099 and 1980–2010 for the ensem-
ble mean of the CMIP5 subensemble. The different
saturations represent signal-to-noise ratio (μ/Sigma)
across the super ensemble (the noise is defined as
one SD within the multi-GCM and multimalaria en-
semble). The hatched area shows the multimalaria
multi-GCM agreement (60% of the models agree on
the sign of changes if the simulated absolute
changes are above 1 mo of malaria transmission).
3288 | www.pnas.org/cgi/doi/10.1073/pnas.1302089111 Caminade et al.
SPECIAL FEATURE
southward shift of the epidemic belt and a northward shift over
A southern Africa (consistent with ref. 10). As LTS decreases sig-
Southern Africa (millions)
30 200
Central Africa (millions)
20 150 nificantly over South America (Fig. 2) those models tend to
10 100 simulate a shift from endemic to epidemic transmission over this
0 50
region in the future climate. SI Appendix, Figs. S6–S10 describe
-10 0
changes in endemic malaria transmission for the different
-20 -50
malaria models for the 2080s under the rcp85 emission scenario.
All malaria models consistently simulate climate to become in-
p2
p4
p6
p8
p2
p4
p6
p8
p2
p4
p6
p8
p2
p4
p6
p8
p2
p4
p6
p8
p2
p4
p6
p8
rc
rc
rc
rc
rc
rc
rc
rc
rc
rc
rc
rc
rc
rc
rc
rc
rc
rc
rc
rc
rc
rc
rc
rc
2020s 2050s 2080s 2020s 2050s 2080s creasingly suitable for malaria transmission over the African
highlands. Generally, the MIASMA malaria model tends to
200 simulate an increase in climate suitability for endemic malaria
Western Africa (millions)
Eastern Africa (millions)
200
0
150
transmission over central Europe and North America in the fu-
-200
ture. The UMEA model simulates endemic transmission over arid
100
areas such as the northern edge of the Sahel and over the Middle
-400 50
East and central Australia (unrealistic changes given the aridity of
-600 0 those regions). MARA tends to simulate suitable future climate
conditions for endemic transmission over the northern edge of the
p2
p4
p6
p8
p2
p4
p6
p8
p2
p4
p6
p8
p2
p4
p6
p8
p2
p4
p6
p8
p2
p4
p6
p8
rc
rc
rc
rc
rc
rc
rc
rc
rc
rc
rc
rc
rc
rc
rc
rc
rc
rc
rc
rc
rc
rc
rc
rc
2020s 2050s 2080s 2020s 2050s 2080s Sahel, southern Africa, western India, and southwestern China.
The most sophisticated malaria models (LMM_RO and VECTRI)
behave similarly; a large area over South America, northern
Australia, the northern Sahel, southern Africa, India, Laos,
B Vietnam, Thailand, and Cambodia is simulated to become un-
Southern Africa (10*8)
4 10
Central Africa (10*8)
2
suitable for endemic malaria transmission in the future. How-
0
5
ever, those changes are sensitive to the driving GCMs, especially
-2
0 near the edges of the current malaria distribution.
-4 -5
-6 -10
Discussion
The results of this multimalaria model, multi-GCM, multi-
p2
p4
p6
p8
p2
p4
p6
p8
p2
p4
p6
p8
p2
p4
p6
p8
p2
p4
p6
p8
p2
p4
p6
p8
rc
rc
rc
rc
rc
rc
rc
rc
rc
rc
rc
rc
rc
rc
rc
rc
rc
rc
rc
rc
rc
rc
rc
rc
2020s 2050s 2080s 2020s 2050s 2080s scenario intercomparison exercice are consistent with previous
studies in indicating that the most significant climate change
10 25 effects are confined to specific regions (highlands in Africa and
Western Africa (10*8)
Eastern Africa (10*8)
0 20 parts of South America and southeastern Asia); in other regions
ENVIRONMENTAL
-10
15 climate change is likely to have no or a lesser effect on malaria
owing to other important socioeconomic factors. Large uncer-
SCIENCES
-20
10
-30
5 tainties are present in the multimodel ensemble, especially over
-40
0 the epidemic fringes of the current malaria distribution. The
impact of climate change on future malaria must be seen in the
p2
p4
p6
p8
p2
p4
p6
p8
p2
p4
p6
p8
p2
p4
p6
p8
p2
p4
p6
p8
p2
p4
p6
p8
rc
rc
rc
rc
rc
rc
rc
rc
rc
rc
rc
rc
rc
rc
rc
rc
rc
rc
rc
rc
rc
rc
rc
rc
2020s 2050s 2080s 2020s 2050s 2080s current context of a decline in malaria at global scale (13);
however, there are concerns about future support for national-
level malaria control efforts (4).
Fig. 3. The estimated population at risk owing to climate change impacts on Climate-induced effects are more consistent with the observed
SUSTAINABILITY
malaria distribution for three time periods for four selected regions in Africa. (A)
changes over a few regions of Africa and South America. Cli-
SCIENCE
Additional population at risk for malaria owing to climate change based on the
mate change may have significant impacts in the east African
MARA, MIASMA, LMM, VECTRI, and UMEA models. (B) Additional person-months
at risk for malaria based on the MARA, MIASMA, LMM, and VECTRI models.
highland region in the future, where the population at risk is
large. This corroborates with the assessment “Human health,
already compromised by a range of factors, could be further
over Brazil. This is consistent with the diverging rainfall projec- negatively impacted by climate change and climate variability,
tions shown by the various GCMs over those regions. The uncer- e.g., malaria in southern Africa and the East African highlands
tainties related to the emission scenarios are relatively small, but (high confidence)” that was published in the Fourth Assessment
they grow as a function of time (especially over South America Report of the IPCC (20). Generally greater climate impacts
across the multimodel ensemble are shown under the higher
and central Africa).
emission scenario (RCP8.5) for the end of the 21st century.
Given those uncertainties, the different malaria model sensi-
There is no clear agreement between models at the lower rate of
tivities to climate change are further investigated for epidemic
warming and for near-term projections.
(SI Appendix, Fig. S5) and endemic transmission zones (SI Ap- This assessment has made an important advance in describing
pendix, Figs. S6–S10). SI Appendix, Fig. S5 compares the future the uncertainty associated with future climate change impacts on
(2080s) and recent location of the simulated malaria epidemic global malaria distributions. Impacts on malaria transmission are
belt based on the rcp85 scenario. The LMM_RO and MIASMA considered an important consequence of future climate change,
models tend to simulate a northward shift of the malaria epi- although it should be recognized that changes in malaria are
demic belt over central-northern Europe, Russia, northern Asia, unlikely to be a major contributor to modifications in the total
and northern America. This is unlikely to translate to increased burden of disease owing to global climate change (2). Projections
malaria morbidity in reality provided that health surveillance of land use change, population growth, migration changes, and
systems in these regions maintain their capacity to identify and economic development were neglected in these models, all of
suppress primary imported infections efficiently. However, in- which will alter the potential transmission bounds set by climate
creasingly suitable climatic conditions might likely increase the (13). The direct and indirect knock-on effects of climate change
incidence of autochthonous malaria cases in developed countries (on social, economic, political, and land use changes) and other
where competent malaria vectors are present, and those au- nonclimatic disease driver changes will ultimately affect the
tochthonous cases generally have high fatality rates. Over the changing vulnerability of the population and its ability to cope
Sahel, the MIASMA and MARA model simulate a northward with and respond to disease burdens (21); this should be accounted
shift of the epidemic belt, whereas the most sophisticated dy- for in a full assessment. In addition, the malaria parasite and
namical models such as VECTRI and LMM_RO simulate a its vector may adapt to evolving environmental conditions over
Caminade et al. PNAS | March 4, 2014 | vol. 111 | no. 9 | 3289
time, questioning the present approach of applying the pres- the VECTRI model could include the impact of future population growth and
ent temperature-dependent life cycle rates (dynamical mod- urbanization on transmission intensity, these factors were inhibited in this
els) or climatic disease bounds (statistical models) to future study to ensure the experiment assumptions are equal for all models. The
climate conditions (22). As the biological models develop further in model is designed for regional to continental scales at high spatial reso-
complexity to incorporate these effects, disparity between the im- lutions of up to 5–10 km. VECTRI is the only full dynamical model partici-
pating in the study operating on a daily time step and accounting for
pact models may widen rather than reduce, raising the issue of
subseasonal variations in climate. As a consequence the VECTRI model is the
whether the simplest models should remain in future impact
only one that requires a representation of human migration to transport
modeling ensembles. Further research on modeling malaria malaria parasites to new regions that may become suitable for future
should also be undertaken at regional or national scales, with transmission. Migration was estimated by mixing population with a co-
validated models, to identify more accurately those populations efficient equivalent to 1% population exchange per year. For full details of
most at risk, based on regional environmental and socioeconomic the models mathematical framework and its evaluation see ref. 17. For
changes (23). Many factors will determine the time at which in- VECTRI, LTS = 1 for a given month if EIR > 0.01 d−1.
dividual countries achieve the capacity to control the disease. UMEA statistical model (model 4). The malaria model is a spatial empirical-
These will need to be addressed in future assessments of the statistical model created at the Umea University (6). The malaria model uses
potential impact of climate change on global malaria. climate and socioeconomic factors to determine the spatial distribution of
endemic malaria (P. falciparum) transmission. Generalized additive logistic
Materials and Methods regression models were used to empirically estimate the relationship be-
MIM Descriptions. All malaria models have been parameterized to simulate tween endemic malaria transmission and climatic factors on a global scale
P. falciparum transmission. A common metric was used to intercompare all using the output of the Malaria Atlas Project Bayesian statistical model,
malaria models. The LTS of malaria was calculated for each MIM based on which combines malaria survey data with environmental and climate pre-
different assumptions (details are given in the following). To avoid spurious dictors to provide a gridded malaria analysis for 2010 (28). Flexible nonlinear
results from small changes in low transmission regions, a minimum of 4 mo relationship and interaction between climate factors on the probability of
of continuous transmission were required to indicate whether the climate malaria transmission were initially established and compared with simpler
was suitable for malaria in a given year. Thus, we defined climate suitability models to find a simple model with good fit. For UMEA, only binary CS
(CS) for malaria such as CS = 1 if LTS > 3 mo. Unstable transmission was estimates were available.
defined for 1 < LTS ≤ 3. For UMEA, only estimates of stable transmission MIASMA model (model 5). The malaria module of the MIASMA model incor-
were available. porates temperature effects on the survival probability and biting frequency
LMM_RO monthly model (model 1). The model used here is a simplified version of of mosquitoes (7). The various temperature-dependent relationships are
the vector transmission potential model formulated by Jones (16) and uses aggregated into the entomological version of the equation for R0. Owing
monthly rainfall and temperature data as inputs. The number of emerging to the lack of data on several key parameters, these are set as biologically
adult mosquitoes at the beginning of each month is taken to be pro- plausible constants, allowing the calculation of the critical vector density
portional to the rain falling during the previous month. The mosquito required for sustainable disease transmission (e.g., R0 >1). This threshold is
population is then combined with the biting rate, sporogonic cycle length, lower under more suitable climate conditions. The inverse of the critical
and survival probability calculated from monthly temperatures, together density threshold, the ‘transmission potential’ (TP), is used as a relative
with the other parameters provided as input to the model, to derive the measure of transmission intensity under different climatic conditions. The
reproduction ratio, R0. If R0 > 1 then malaria transmission occurs for a given model assumes that a minimum level of monthly rainfall of 80 mm is es-
month. The derivation of R0 is based on the transmission model component sential for malaria transmission, based on the value used in the MARA
of the full LMM (Liverpool Malaria Model), which is a weather-driven, project (18, 29). In this assessment, the modeled distribution is not con-
mathematical–biological model of malaria that was originally formulated by strained by the current distribution of malaria vectors (7). For MIASMA,
Hoshen and Morse (24) and has been applied at national and regional scales. LTS = 1 for a given month if TP > 0.
The full LMM model uses daily rainfall and temperature data as inputs. It has
been successfully validated against a 20-y clinical record for Botswana (25). Climate and Population Scenario Data. The Coupled Model Intercomparison
For LMM_RO, LTS = 1 for a given month if Ro > 1. Project Phase 5 (CMIP5) project is collaboration among climate modelers to
MARA model (model 2). The MARA seasonality model was original derived to produce a consistent set of climate model outputs for the RCP emissions
map start and end months of the malaria transmission season for locations in scenarios. The CMIP experimental design is described in ref. 30. The CMIP5
Africa based on monthly long-term averages of rainfall and temperature (18). output was bias-corrected by the Potsdam Institute for Climate Impact Re-
It was modified (16) to create a simple model of seasonal malaria trans- search (31) for this project to ensure statistical agreement with the observed
mission. The basic requirements of the model are 3 mo of rainfall at a min- Watch Forcing Data dataset over the period 1960–1999. All climate scenarios
imum value (60 mm) together with a catalyst month specified by another were mapped to a uniform half-degree grid. The RCP emission scenarios
minimum rainfall value (80 mm). Temperature is constrained to be greater (RCP2.6, RCP4.5, RCP6, and RCP8) represent a range of climate forcings.
than a threshold value (19.5 °C) plus a seasonality index calculated from the Climate scenarios were available for all RCPs and for five global climate
SD of the monthly rainfall. The resulting output is either “on,” indicating the models: HadGem2-ES, IPSL-CM5A-LR, MIROC-ESM-CHEM, GFDL-ESM2M, and
malaria season is in progress, or “off,” indicating one or more of the con- NorESM1-M. The five models were selected to give a wide range of tem-
ditions have not been met. For MARA, LTS is a direct output of the model. perature and rainfall changes, rather than a representation of the likelihood
VECTRI model (model 3). VECTRI is a mathematical model for malaria trans- of future climate change (15). Climate data were available to 2100; however,
mission that accounts for the impact of temperature and rainfall variability on malaria integrations were undertaken for three time slices (30-y averages):
the development cycles of the malaria vector in its larval and adult stage, and 2020s (2005–2035), 2050s (2035–2065), and 2080s (2069–2099), with the ex-
also of the parasite itself. The parameterizations for the biological processes ception of VECTRI, which instead conducted century-long integrations from
are taken from the literature for the Anopheles gambiae vector and the the present to 2100 using daily climate data.
P. falciparum species of the parasite. Temperature affects the sporogonic To evaluate the respective bias-corrected baseline integrations, additional
and gonotrophic cycle development rates according to the standard degree- malaria integrations were conducted using two sets of gridded observed
day model, and higher temperature increases the mortality rates for adult climate datasets. The first set used temperature and precipitation from the
vectors (18). Rainfall effects on transmission are represented by a simple, Climatic Research Unit (CRU) dataset v3.1 (32) for a period very close to the
physically based model of surface pool hydrology, whereby rainfall increases historical integrations 1980–2009. Because the CRU data were only available
available breeding sites that subsequently decay through evaporation and at monthly timescale, the VECTRI model was excluded from this analysis. The
infiltration, and intense rain events decrease early-stage larvae through second set of integrations used the Tropical Rainfall Measuring Mission
flushing (26). In reality, land surface properties also modify the availability of (TRMM) 3B42 dataset (33) with precipitation retrievals based on microwave
breeding sites, but VECTRI does not presently model these. VECTRI accounts and precipitation radar observations, supplemented with infrared in-
for human population density in the calculation of biting rates. Higher formation when the former was unavailable. The temperature information
population densities lead to a dilution effect, resulting in lower parasite was derived from the interim reanalysis of the European Centre for Medium-
ratios (PRs) in urban and peri-urban environments compared with nearby Range Weather Forecasts (34). Both observed climate datasets (CRUTS3.1
rural locations. In this respect the model is able to reproduce the reduction and TRMMERAI) were aggregated to the half-degree grid of the CMIP5
in entomological inoculation rates (EIR) and PR with increasing population climate data. Malaria integrations were also conducted for the modeled
density that has been widely observed in African field studies (27). Although baseline period (historical) for each GCM (1980–2010).
3290 | www.pnas.org/cgi/doi/10.1073/pnas.1302089111 Caminade et al.
SPECIAL FEATURE
For the assessment of future populations at risk for malaria we used climate baseline datasets and GCM modeled baselines and compared those
a single population projection from the new Shared Socio-economic Pathway outputs with other published malaria endemicity maps based on ref. 13.
(SSP) set of socio-economic scenarios (35). We used the SSP2 population Preintervention malaria endemicity estimates are based on a major synthesis
scenario, which projects a population of 9.5 billion people in 2055 (36). The of historical records, documents, and maps of a variety of malariometric
national projections for 193 countries were converted to a gridded pop- indices for the four major Plasmodium species (malariae, ovalae, vivax, and
ulation product by first deriving a population map for 2000 scaling the falciparum) that was conducted by Lysenko (38). Recent malaria ende-
gridded Gridded Population of the World v3 dataset (37) to match the na- micity estimates (P. falciparum) have been derived from the Malaria Atlas
tional totals. This distribution was then projected into the future using na-
Project (MAP) for comparison purposes (14). The MAP dataset is an analysis
tional average projections to scale each grid point. A small number of
integrating survey data with environmental and socioeconomic predictors
countries not present in the dataset were assigned the global-mean pop-
in a Bayesian model to produce a “best guess” of mapped malaria ende-
ulation growth rate over the next century. The reference years for the
micity at global scale. These datasets were digitized from the original
population data were as follows: current climate, 2000; 2020s, 2020; 2050s,
2050; and 2080s, 2085 population. papers. This allows a comparison with the malaria model outputs for which
the epidemic and stable transmission regions are defined for a criterion
Estimating Populations at Risk for Malaria. We estimated two population based on LTS.
outcomes. The population at risk for malaria (PAR) was defined as the
population present in an area where the climate was suitable for malaria Supplementary Information. Further details about the MIM validation, the
transmission (averaged CS > 0.5). Person months at risk (PMAR) were cal- estimation of the uncertainties in the super ensemble, and changes in en-
culated as the length of the transmission season multiplied by the pop- demic and epidemic transmission for each MIM are provided in SI Appendix.
ulation living in the grid cell. The climate change attributable PAR and
PMAR were estimated as the difference between future population at risk ACKNOWLEDGMENTS. The Inter-Sectoral Impact Model Intercomparison
for a given scenario compared with the population at risk under the current Project Fast Track project was funded by the German Federal Ministry of
modeled climate. It was not possible to estimate PMAR for the UMEA model, Education and Research with project funding reference number 01LS1201.
which only produces annually averaged CS binary outputs. All estimates A.P.M., C.C., and F.J.C.-G. were jointly funded by the European Union
FP7 Quantifying Weather and Climate Impacts on Health in Developing
were aggregated to world regions (15).
Countries (QWeCI) and HEALTHY FUTURES projects. C.C. and A.P.M. also
acknowledge funding support from the End-to-End Quantification of
Model Validation. To attempt some validation of the different malaria Uncertainty for Impacts Prediction (EQUIP) Natural Environmental Re-
models, we compared the output of the malaria models for the two observed search Council Project NE/H003487/1.
1. Costello A, et al. (2009) Managing the health effects of climate change. Lancet 20. Confalonieri U, et al. (2007) Human health. Climate Change 2007: Impacts, Adapta-
373(9676):1693–1733. tion and Vulnerability. Contribution of Working Group II to the Fourth Assessment
2. McMichael AJ, et al. (2004) Climate change. Comparative Quantification of Health Report of the Intergovernmental Panel on Climate Change, eds Parry ML, et al.
Risks: Global and Regional Burden of Disease Due to Selected Major Risk Factors, eds (Cambridge Univ Press, Cambridge, UK), pp 391–431.
Ezzati M, et al. (World Health Organization, Geneva), Vol 2, pp 1543–1649. 21. McMichael AJ, Woodruff RE, Hales S (2006) Climate change and human health:
ENVIRONMENTAL
3. Murray CJ, et al. (2012) Global malaria mortality between 1980 and 2010: A systematic present and future risks. Lancet 367(9513):859–869.
22. Hoffmann AA, Sgrò CM (2011) Climate change and evolutionary adaptation. Nature
SCIENCES
analysis. Lancet 379(9814):413–431.
4. Feachem RG, et al. (2010) Shrinking the malaria map: Progress and prospects. Lancet 470(7335):479–485.
376(9752):1566–1578. 23. Bouma MJ, Baeza A, terVeen A, Pascual M (2011) Global malaria maps and climate
5. WHO (2011) World Malaria Report 2011 (World Health Organization, Geneva), pp 1–248. change: A focus on East African highlands. Trends Parasitol 27(10):421–422.
6. Beguin A, et al. (2011) The opposing effects of climate change and socio-economic de- 24. Hoshen MB, Morse AP (2004) A weather-driven model of malaria transmission. Malar
velopment on the global distribution of malaria. Glob Environ Change 21(4):1209–1214. J 3:32.
7. van Lieshout M, et al. (2004) Climate change and malaria: Analysis of the SRES climate 25. Jones A, Morse AP (2010) Application and validation of a seasonal ensemble pre-
and socio-economic scenarios. Glob Environ Change 14(1):87–99. diction system using a dynamic malaria model. J Clim 23:4202–4215.
8. Snow RW, Hay S, Marsh K (2006) Report T5.8: Malaria in Africa: Sources, risks, drivers 26. Paaijmans KP, Wandago MO, Githeko AK, Takken W (2007) Unexpected high losses of
SUSTAINABILITY
and disease burden 2005–2030. Infectious Diseases: Preparing for the Future (Office Anopheles gambiae larvae due to rainfall. PLoS ONE 2(11):e1146.
27. Kelly-Hope LA, McKenzie FE (2009) The multiplicity of malaria transmission: a review
SCIENCE
of Science and Innovation, London).
of entomological inoculation rate measurements and methods across sub-Saharan
9. Tanser FC, Sharp B, le Sueur D (2003) Potential effect of climate change on malaria
Africa. Malar J 8(1):19.
transmission in Africa. Lancet 362(9398):1792–1798.
28. Gething PW, et al. (2011) A new world malaria map: Plasmodium falciparum ende-
10. Ermert V, Fink AH, Morse AP, Paeth H (2012) The impact of regional climate change
micity in 2010. Malar J 10:378.
on malaria risk due to greenhouse forcing and land-use changes in tropical Africa.
29. MARA/ARMA Collaboration (1998) Towards an atlas of malaria risk in Africa. First Tech-
Environ Health Perspect 120(1):77–84.
nical Report of the MARA/ARMA Collaboration (MARA/ARMA, Durban, South Africa).
11. Rogers DJ, Randolph SE (2000) The global spread of malaria in a future, warmer
30. Taylor KE, Stouffer RJ, Meehl GA (2012) An overview of CMIP5 and the experiment
world. Science 289(5485):1763–1766.
design. Bull Am Meteorol Soc 93:485–498.
12. Tatem AJ, Guerra CA, Kabaria CW, Noor AM, Hay SI (2008) Human population, urban
31. Hempel S, et al. (2013) A trend-preserving bias correction – the ISI-MIP approach.
settlement patterns and their impact on Plasmodium falciparum malaria endemicity.
Earth System Dynamics 4:49–92.
Malar J 7:218. 32. Mitchell TD, Jones PD (2005) An improved method of constructing a database of monthly
13. Gething PW, et al. (2010) Climate change and the global malaria recession. Nature climate observations and associated high‐resolution grids. Int J Climatol 25:693–712.
465(7296):342–345. 33. Huffman GJ, et al. (2007) The TRMM Multisatellite Precipitation Analysis (TMPA): Quasi-
14. Hay SI, et al. (2009) A world malaria map: Plasmodium falciparum endemicity in 2007. global, multiyear, combined-sensor precipitation estimates at fine scales. J Hydrometeorol
PLoS Med 6(3):e1000048. 8:38–55.
15. Warszawski L, et al. (2014) The Inter-Sectoral Impact Model Intercomparison Project 34. Dee DP, et al. (2011) The ERA‐Interim reanalysis: Configuration and performance of
(ISI-MIP): Project framework. Proc Natl Acad Sci USA 111:3228–3232. the data assimilation system. Q J R Meteorol Soc 137:553–597.
16. Jones A (2007) Seasonal ensemble prediction of malaria in Africa. PhD thesis (Univ of 35. Van Vuuren DP, et al. (2012) A proposal for a new scenario framework to support
Liverpool, Liverpool). research and assessment in different climate research communities. Glob Environ
17. Tompkins AM, Ermert V (2013) A regional-scale, high resolution dynamical malaria Change 22(1):21–35.
model that accounts for population density, climate and surface hydrology. Malar 36. SSP Database (2012) Shared Socioeconomic Pathways database. Available at https://
J 12:65. secure.iiasa.ac.at/web-apps/ene/SspDb.
18. Craig MH, Snow RW, le Sueur D (1999) A climate-based distribution model of malaria 37. Center for International Earth Science Information Network (2005) Gridded Popu-
transmission in sub-Saharan Africa. Parasitol Today 15(3):105–111. lation of the World, Version 3 (GPWv3) Data Collection (Columbia Univ, Palisades, NY).
19. Moss RH, et al. (2010) The next generation of scenarios for climate change research 38. Lysenko AJSI (1968)Geography of Malaria: A Medico-Geographic Profile of an Ancient
and assessment. Nature 463(7282):747–756. Disease, ed Lebedew AW (Academy of Sciences, Moscow), pp 25–146.
Caminade et al. PNAS | March 4, 2014 | vol. 111 | no. 9 | 3291
Potrebbero piacerti anche
- Toxic Vaccines WEB SITES and LinksDocumento78 pagineToxic Vaccines WEB SITES and LinksDr. Heath MotleyNessuna valutazione finora
- Nemesis by Philip RothDocumento16 pagineNemesis by Philip RothHoughton Mifflin Harcourt100% (1)
- PHYSIOTHERAPY IN ICU: MODALITIES FOR CRITICALLY ILL PATIENTSDocumento18 paginePHYSIOTHERAPY IN ICU: MODALITIES FOR CRITICALLY ILL PATIENTS_darkangel26_0% (1)
- Hearing ImpairmentDocumento9 pagineHearing Impairmentmansi singhNessuna valutazione finora
- Climate Change and Vector-Borne Diseases of Public Health SignificanceDocumento8 pagineClimate Change and Vector-Borne Diseases of Public Health SignificanceAriadne Cristina De Antonio100% (1)
- Parasitology-Lec 7 Lung FlukesDocumento5 pagineParasitology-Lec 7 Lung Flukesapi-3743217100% (1)
- 4 Toxemia ExplainedDocumento13 pagine4 Toxemia ExplainedJonas Sunshine CallewaertNessuna valutazione finora
- (Lecture Notes) R D T Farmer - Ross Lawrenson - Epidemiology and Public Health Medicine-Blackwell (2004)Documento200 pagine(Lecture Notes) R D T Farmer - Ross Lawrenson - Epidemiology and Public Health Medicine-Blackwell (2004)Katrina Deanne del Mundo100% (2)
- Climate Change and Infectious DiseasesDocumento2 pagineClimate Change and Infectious DiseasesVirabaseNessuna valutazione finora
- Impetigo: A Bacterial Skin InfectionDocumento13 pagineImpetigo: A Bacterial Skin InfectionTasya SyafhiraNessuna valutazione finora
- Tropical Med Int Health - 2009 - Mendis - From Malaria Control To Eradication The WHO PerspectiveDocumento8 pagineTropical Med Int Health - 2009 - Mendis - From Malaria Control To Eradication The WHO PerspectiveDircia D'silvaNessuna valutazione finora
- Multivariate RegressionDocumento8 pagineMultivariate RegressionAnggitya PratiwiNessuna valutazione finora
- MAERSK FILIPINAS CREWING INC Vs MESINADocumento2 pagineMAERSK FILIPINAS CREWING INC Vs MESINAjojo50166Nessuna valutazione finora
- Environmental Factors Spread Microbial Infections PhilippinesDocumento6 pagineEnvironmental Factors Spread Microbial Infections PhilippinesAbi NeriNessuna valutazione finora
- Pubs Ceccato Gis Remote SensingDocumento16 paginePubs Ceccato Gis Remote SensingKlinik FiraraNessuna valutazione finora
- 1 s2.0 S0001706X17309798 Main PDFDocumento11 pagine1 s2.0 S0001706X17309798 Main PDFsiska pratiwiNessuna valutazione finora
- Modelling Anopheles Gambiae S.S. Population Dynamics With Temperature-And Age-Dependent SurvivalDocumento31 pagineModelling Anopheles Gambiae S.S. Population Dynamics With Temperature-And Age-Dependent SurvivalDuskRiderNessuna valutazione finora
- Statistical Modelling of The E On Malaria Occurrence in Abuja, NigeriaDocumento12 pagineStatistical Modelling of The E On Malaria Occurrence in Abuja, NigeriaShólànké Ezekiel ShówúnmiNessuna valutazione finora
- Spatial-Explicit Modeling of Social Vulnerability To Malaria in East AfricaDocumento16 pagineSpatial-Explicit Modeling of Social Vulnerability To Malaria in East AfricaNaufal MuzaNessuna valutazione finora
- Journal Pone 0193493Documento23 pagineJournal Pone 0193493billycuts6068Nessuna valutazione finora
- Hales 2002Documento5 pagineHales 2002Bilal MalikNessuna valutazione finora
- Climate Adaptation in The Public Health Sector in Africa: Evidence From United Nations Framework Convention On Climate Change National CommunicationsDocumento10 pagineClimate Adaptation in The Public Health Sector in Africa: Evidence From United Nations Framework Convention On Climate Change National CommunicationsAdan Ahmed BulaleNessuna valutazione finora
- 2014 - Gething - MJ - Declining Malaira in Africa - Improving The Measurement of ProgressDocumento5 pagine2014 - Gething - MJ - Declining Malaira in Africa - Improving The Measurement of ProgressnomdeplumNessuna valutazione finora
- ITNs Difficult to Maintain Malaria Prevention AfricaDocumento9 pagineITNs Difficult to Maintain Malaria Prevention AfricaAneeta ann abrahamNessuna valutazione finora
- (Articulo) Epidemiologia - Modelling Plant Diseases EpidemicsDocumento14 pagine(Articulo) Epidemiologia - Modelling Plant Diseases EpidemicsFernanda PenagosNessuna valutazione finora
- Review of COVID On CADocumento14 pagineReview of COVID On CAvit1234Nessuna valutazione finora
- Tompkins 2013Documento24 pagineTompkins 2013ibrahima1968Nessuna valutazione finora
- Malaria 4Documento16 pagineMalaria 4Andres RomeroNessuna valutazione finora
- Stephanie Blueprint-1Documento33 pagineStephanie Blueprint-1kasimmo4444Nessuna valutazione finora
- Achieving Global Malaria Eradication in Changing LandscapesDocumento14 pagineAchieving Global Malaria Eradication in Changing LandscapesWt LópezNessuna valutazione finora
- Spatio-Temporal Variation and Socio-Demographic Characters of Malaria in Chimoio Municipality, MozambiqueDocumento11 pagineSpatio-Temporal Variation and Socio-Demographic Characters of Malaria in Chimoio Municipality, MozambiqueJoão FerrãoNessuna valutazione finora
- 10 1016@j Nonrwa 2019 103081Documento33 pagine10 1016@j Nonrwa 2019 103081ShafaNessuna valutazione finora
- Global Numbers of Infection and Disease Burden of Soil Transmitted Helminth Infections in 2010Documento19 pagineGlobal Numbers of Infection and Disease Burden of Soil Transmitted Helminth Infections in 2010Yuanita ClaraNessuna valutazione finora
- Climate and Health Early WarningDocumento21 pagineClimate and Health Early WarningmeaghandalyNessuna valutazione finora
- Literature Review On Malaria FeverDocumento5 pagineLiterature Review On Malaria Feverafmyervganedba100% (1)
- Mathematical Modelling of Infectious DiseasesDocumento10 pagineMathematical Modelling of Infectious Diseasesbdalcin5512Nessuna valutazione finora
- Reported Incidence of Fever For Under-5 Children in Zambia: A Longitudinal StudyDocumento7 pagineReported Incidence of Fever For Under-5 Children in Zambia: A Longitudinal StudyBassim BirklandNessuna valutazione finora
- 2017Documento15 pagine2017SANDIE SORELLENessuna valutazione finora
- Ain Shams Engineering Journal: O.A. Mokuolu, A.O. Coker, M. Adejumo, M.K.C. SridharDocumento5 pagineAin Shams Engineering Journal: O.A. Mokuolu, A.O. Coker, M. Adejumo, M.K.C. SridharVincent NollanNessuna valutazione finora
- Agent-Based Models of Malaria Transmission: A Systematic ReviewDocumento16 pagineAgent-Based Models of Malaria Transmission: A Systematic ReviewAshish SharmaNessuna valutazione finora
- Lit - Jumbam - 2020 - BMC PH - KAP of Malaria Interventions in Rural ZambiaDocumento15 pagineLit - Jumbam - 2020 - BMC PH - KAP of Malaria Interventions in Rural ZambianomdeplumNessuna valutazione finora
- Science 4Documento2 pagineScience 4Wut PuNessuna valutazione finora
- A Bayesian Spatio-Temporal Analysis of Malaria in The Greater Accra Region of Ghana From 2015 To 2019Documento15 pagineA Bayesian Spatio-Temporal Analysis of Malaria in The Greater Accra Region of Ghana From 2015 To 2019Francisca CatacutanNessuna valutazione finora
- Mbe 16 03 069Documento31 pagineMbe 16 03 069Emmanuel GolohorNessuna valutazione finora
- Global Malaria Infection Risk From Climate ChangeDocumento13 pagineGlobal Malaria Infection Risk From Climate Changegerges8723Nessuna valutazione finora
- ch03 s03 Subch0311Documento28 paginech03 s03 Subch0311michelepositinoNessuna valutazione finora
- 1 s2.0 S1877584522000600 MainDocumento11 pagine1 s2.0 S1877584522000600 MainwanderbragabjjjNessuna valutazione finora
- Control Strategies For Endemic Childhood Scabies: Stephen J. GilmoreDocumento15 pagineControl Strategies For Endemic Childhood Scabies: Stephen J. GilmoreNgennest HimNessuna valutazione finora
- ARTIGO3Documento9 pagineARTIGO3Stephane Rodrigues CarvalhoNessuna valutazione finora
- Erl9 1 014011Documento9 pagineErl9 1 014011Edgar ContrerasNessuna valutazione finora
- s12936 017 2110 7Documento12 pagines12936 017 2110 7M Franck MakongaNessuna valutazione finora
- InglesDocumento6 pagineInglesLavíniaNessuna valutazione finora
- Tugas Prom Gizi12Documento8 pagineTugas Prom Gizi12Krisna AlfianurNessuna valutazione finora
- Dengue Prevalence As An Evidence of Climate Change in Sri LankaDocumento8 pagineDengue Prevalence As An Evidence of Climate Change in Sri LankaSupun Lahiru PrakashNessuna valutazione finora
- Ebi 2005Documento19 pagineEbi 2005Potato WedgesNessuna valutazione finora
- Risa 12831Documento23 pagineRisa 12831BakolonNessuna valutazione finora
- Modelling The Dynamics of Dengue Real Epidemics: Doi:10.1098/rsta.2010.0278Documento15 pagineModelling The Dynamics of Dengue Real Epidemics: Doi:10.1098/rsta.2010.0278p1804212012Nessuna valutazione finora
- Social Justice, Climate Change, and Dengue: Aileen Y. Chang, Douglas O. Fuller, Olveen Carrasquillo, John C. BeierDocumento12 pagineSocial Justice, Climate Change, and Dengue: Aileen Y. Chang, Douglas O. Fuller, Olveen Carrasquillo, John C. BeierSoniJfreeNessuna valutazione finora
- BUENO MAL Potential Geographical Distribution of Anopheles Gambiae Worldwide MALARIA REFERENCIADocumento6 pagineBUENO MAL Potential Geographical Distribution of Anopheles Gambiae Worldwide MALARIA REFERENCIAgerges8723Nessuna valutazione finora
- Desouzaetal 2012climateimpactondiseasescopeDocumento21 pagineDesouzaetal 2012climateimpactondiseasescopewenyouNessuna valutazione finora
- Climate Change and Malaria Predictions Becoming RealityDocumento2 pagineClimate Change and Malaria Predictions Becoming Realitygerges8723Nessuna valutazione finora
- RESEARCH ARTICLEOpen AccessObservational Study: 27 Years of Severemalaria Surveillance in Kilifi, KenyaDocumento9 pagineRESEARCH ARTICLEOpen AccessObservational Study: 27 Years of Severemalaria Surveillance in Kilifi, KenyaLuís MiguelNessuna valutazione finora
- Means of Dispersal - MosquitoDocumento1 paginaMeans of Dispersal - MosquitoBaba KelaNessuna valutazione finora
- Is The Current Decline in Malaria Burden in Sub-Saharan Africa Due To A Decrease in Vector Population?Documento9 pagineIs The Current Decline in Malaria Burden in Sub-Saharan Africa Due To A Decrease in Vector Population?Bawi Cung LianNessuna valutazione finora
- Species Distribution Models Are Inappropriate For COVID-19: CommentDocumento2 pagineSpecies Distribution Models Are Inappropriate For COVID-19: CommenthermalfaroncalNessuna valutazione finora
- Matecconf Iconbee2019 02007Documento6 pagineMatecconf Iconbee2019 02007hermaNessuna valutazione finora
- Fuzzy Association Rule Mining and Classification For The Prediction of Malaria in South Korea (PDFDrive)Documento17 pagineFuzzy Association Rule Mining and Classification For The Prediction of Malaria in South Korea (PDFDrive)Taher JelleliNessuna valutazione finora
- Beyond One Health: From Recognition to ResultsDa EverandBeyond One Health: From Recognition to ResultsJohn A. HerrmannNessuna valutazione finora
- Charting the Next Pandemic: Modeling Infectious Disease Spreading in the Data Science AgeDa EverandCharting the Next Pandemic: Modeling Infectious Disease Spreading in the Data Science AgeNessuna valutazione finora
- Multiple Myeloma and Other Plasma Cell NeoplasmsDa EverandMultiple Myeloma and Other Plasma Cell NeoplasmsMeletios A. DimopoulosNessuna valutazione finora
- Shrestha Et Al 2020 Spatial Distribution of Extreme Precipitation Events and Its Trend in NepalDocumento10 pagineShrestha Et Al 2020 Spatial Distribution of Extreme Precipitation Events and Its Trend in NepalAnggitya PratiwiNessuna valutazione finora
- Aees 8 2 4Documento11 pagineAees 8 2 4Anggitya PratiwiNessuna valutazione finora
- 0016 7169 Geoint 44 04 347Documento7 pagine0016 7169 Geoint 44 04 347Anggitya PratiwiNessuna valutazione finora
- Somers'dDocumento8 pagineSomers'dAnggitya PratiwiNessuna valutazione finora
- Impacts of Climate Changes On Water Resources in Yellow River Basin, ChinaDocumento9 pagineImpacts of Climate Changes On Water Resources in Yellow River Basin, ChinaAnggitya PratiwiNessuna valutazione finora
- Koefisien KorelasiDocumento10 pagineKoefisien KorelasipetriliaNessuna valutazione finora
- Impact of climate change on global malaria distributionDocumento6 pagineImpact of climate change on global malaria distributionAnggitya PratiwiNessuna valutazione finora
- 1 PDFDocumento6 pagine1 PDFAnggitya PratiwiNessuna valutazione finora
- 1Documento14 pagine1Anggitya PratiwiNessuna valutazione finora
- Bias CorrectionDocumento12 pagineBias CorrectionAnggitya PratiwiNessuna valutazione finora
- Spi Program Alternative MethodDocumento16 pagineSpi Program Alternative Methodscience1990Nessuna valutazione finora
- 431 Boundary Layer SlidesDocumento13 pagine431 Boundary Layer SlidesAnggitya PratiwiNessuna valutazione finora
- Quality and Standards and Their Role in Responding To Covid-19Documento18 pagineQuality and Standards and Their Role in Responding To Covid-19Ardhi Novrialdi GintingNessuna valutazione finora
- WHO 2011 Typhoid FeverDocumento39 pagineWHO 2011 Typhoid FeverVizzi Alvi Fitrah NasutionNessuna valutazione finora
- Baiga Ka Ausadhiamarkantak PDFDocumento7 pagineBaiga Ka Ausadhiamarkantak PDFSunNessuna valutazione finora
- Food and Nutrition Need in Emergencies 2003Documento57 pagineFood and Nutrition Need in Emergencies 2003NebojanNessuna valutazione finora
- Case River BlindnessDocumento2 pagineCase River BlindnessMuhd ZawirNessuna valutazione finora
- MDF Lesson ModuleDocumento28 pagineMDF Lesson ModulePeter Philip M. Perez100% (1)
- Culture-Bound Syndromes and The Neglect of Cultural Factors in Psychopathologies Among AfricansDocumento8 pagineCulture-Bound Syndromes and The Neglect of Cultural Factors in Psychopathologies Among AfricansOtto FischerNessuna valutazione finora
- Dysphagia Causes and DiagnosisDocumento46 pagineDysphagia Causes and DiagnosisnanohaniwiekoNessuna valutazione finora
- Assignment On PrionsDocumento22 pagineAssignment On PrionsRinta Moon100% (2)
- Math and You Chapter 4 PDFDocumento50 pagineMath and You Chapter 4 PDFChelsea RoseNessuna valutazione finora
- Be It Ordained by The Sangguniang Panlungsod of The City of San Carlos, Province of Negros Occidental in Regular Session Assembled ThatDocumento7 pagineBe It Ordained by The Sangguniang Panlungsod of The City of San Carlos, Province of Negros Occidental in Regular Session Assembled ThatJayson CalbanNessuna valutazione finora
- Wang Et Al. - 2020 - Time Series Prediction For The Epidemic Trends of COVID-19 Using The Improved LSTM Deep Learning Method Case Stu (2) - AnnotatedDocumento8 pagineWang Et Al. - 2020 - Time Series Prediction For The Epidemic Trends of COVID-19 Using The Improved LSTM Deep Learning Method Case Stu (2) - AnnotatedZipeng WuNessuna valutazione finora
- Historia Del Tratamiento de La Sífilis - SCIELO PDFDocumento14 pagineHistoria Del Tratamiento de La Sífilis - SCIELO PDFBrenda MoralesNessuna valutazione finora
- SLE Care: Systemic Lupus Erythematosus Signs, Symptoms, and Nursing ResponsibilitiesDocumento8 pagineSLE Care: Systemic Lupus Erythematosus Signs, Symptoms, and Nursing ResponsibilitiesampalNessuna valutazione finora
- Toxoplasmosis: Causes, Symptoms & PreventionDocumento27 pagineToxoplasmosis: Causes, Symptoms & PreventionKnjigeNessuna valutazione finora
- MC2021-029 - Galing Pook Awards GuidelinesDocumento13 pagineMC2021-029 - Galing Pook Awards GuidelinesMemvi BaurileNessuna valutazione finora
- Phrasal Verbs 1Documento4 paginePhrasal Verbs 1Steven DaviesNessuna valutazione finora
- Zika Mosquitoes 14845 TrueDocumento7 pagineZika Mosquitoes 14845 Trueapi-301245392Nessuna valutazione finora
- Malaysians' non-compliance with Covid rulesDocumento2 pagineMalaysians' non-compliance with Covid rulesEvol 9897Nessuna valutazione finora
- History of Malaria and Its Control in IndiaDocumento4 pagineHistory of Malaria and Its Control in IndiamuhanuziNessuna valutazione finora
- MacrolidesDocumento9 pagineMacrolidesAnish Kumar ANessuna valutazione finora