Potrebbero piacerti anche
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5795)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1091)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (74)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- Vacancy Request FormDocumento4 pagineVacancy Request FormmunyekiNessuna valutazione finora
- Marcuse - The Enclave The Citadel and The GhettoDocumento15 pagineMarcuse - The Enclave The Citadel and The GhettoBruno Pepe Russo100% (1)
- Background Verification FormDocumento6 pagineBackground Verification Formsubbujantu0% (1)
- Rob Cum Flyover PDFDocumento1 paginaRob Cum Flyover PDFDHRUV PuneNessuna valutazione finora
- PMC DSR 2017-18 For Rehabilitation of BridgeDocumento5 paginePMC DSR 2017-18 For Rehabilitation of BridgeDHRUV PuneNessuna valutazione finora
- Structures or Bridges Which Are Delete From Inventory of NH 211ZZDocumento2 pagineStructures or Bridges Which Are Delete From Inventory of NH 211ZZDHRUV PuneNessuna valutazione finora
- Public Works Division, Miraj: Government of Maharashtra Public Works Region, Pune Public Works Circle, KolhapurDocumento3 paginePublic Works Division, Miraj: Government of Maharashtra Public Works Region, Pune Public Works Circle, KolhapurDHRUV PuneNessuna valutazione finora
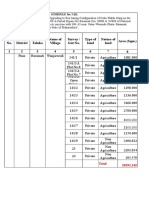
- Area (SQM.) 1 2 3 4 5 6 7 8 Sr. No. Name of District Name of Taluka Name of Village Survey / Gut No. Type of Land Nature of LandDocumento4 pagineArea (SQM.) 1 2 3 4 5 6 7 8 Sr. No. Name of District Name of Taluka Name of Village Survey / Gut No. Type of Land Nature of LandDHRUV PuneNessuna valutazione finora
- Declaration Form 11 NewDocumento1 paginaDeclaration Form 11 NewDHRUV PuneNessuna valutazione finora
- Letter To Pavement Quality Control Mix Design - M40 Grade PDFDocumento2 pagineLetter To Pavement Quality Control Mix Design - M40 Grade PDFDHRUV PuneNessuna valutazione finora
- Amit Dixit: Curriculum VitaeDocumento4 pagineAmit Dixit: Curriculum VitaeSourabh SharmaNessuna valutazione finora
- Three Levels of ManagementDocumento2 pagineThree Levels of ManagementNas NicoleNessuna valutazione finora
- Financial Management Practices On Growth of Small and Medium Enterprises: A Case of Manufacturing Enterprises in Nairobi County, KenyaDocumento13 pagineFinancial Management Practices On Growth of Small and Medium Enterprises: A Case of Manufacturing Enterprises in Nairobi County, KenyaIOSRjournalNessuna valutazione finora
- Management Project SD 1Documento13 pagineManagement Project SD 1Chaitanya KumbharNessuna valutazione finora
- TOPIC 8 Provisions For Non Unionised Employees As Stipulated in The Employment Act, 1955Documento74 pagineTOPIC 8 Provisions For Non Unionised Employees As Stipulated in The Employment Act, 1955LunaNessuna valutazione finora
- Faithless Servant Doctrine: Employer's Right To Recover Compensation From Disloyal EmployeesDocumento10 pagineFaithless Servant Doctrine: Employer's Right To Recover Compensation From Disloyal EmployeesRobert B. FitzpatrickNessuna valutazione finora
- Polygraph ScienceDocumento17 paginePolygraph ScienceAssignmentLab.comNessuna valutazione finora
- Vargas Inc Produces Industrial Machinery Vargas Has A Machining DepartmentDocumento1 paginaVargas Inc Produces Industrial Machinery Vargas Has A Machining DepartmentAmit PandeyNessuna valutazione finora
- CBLM Basic Work in A Team EnvironmentDocumento21 pagineCBLM Basic Work in A Team Environmenternest macalaladNessuna valutazione finora
- Holy Cross of Davao vs. JoaquinDocumento2 pagineHoly Cross of Davao vs. JoaquinAlex Mae Chiu100% (1)
- MBA 402 Assessment2 Answer Template V3Documento6 pagineMBA 402 Assessment2 Answer Template V3awasthisailesNessuna valutazione finora
- EthicsDocumento5 pagineEthicsSwathi AshokNessuna valutazione finora
- H&M CSRDocumento17 pagineH&M CSRphile181289Nessuna valutazione finora
- Global Heritage For Fast-Trac (Tor) Success: HR Interview: New Holland Tractors (India) Pvt. LTDDocumento2 pagineGlobal Heritage For Fast-Trac (Tor) Success: HR Interview: New Holland Tractors (India) Pvt. LTDsandeepNessuna valutazione finora
- 10gfghhj OdtDocumento3 pagine10gfghhj OdtAkhila FrancisNessuna valutazione finora
- Life Satisfaction Literature ReviewDocumento4 pagineLife Satisfaction Literature Reviewaflskeqjr100% (1)
- Cases Compilation LABORDocumento21 pagineCases Compilation LABORdll123Nessuna valutazione finora
- Interview and RocateDocumento1 paginaInterview and RocateIBRAX FFNessuna valutazione finora
- Shuttle Driver PDOT in DALLAS, Texas Careers atDocumento1 paginaShuttle Driver PDOT in DALLAS, Texas Careers atበእርሱ ፈቃድNessuna valutazione finora
- Contemporary Economic Issues Affecting The Filipino EntrepreneurDocumento25 pagineContemporary Economic Issues Affecting The Filipino EntrepreneurMark Anthony AtaizaNessuna valutazione finora
- Nissan ReportDocumento9 pagineNissan ReportAmornrat Ting-Ting SriprajittichaiNessuna valutazione finora
- KS Bull 08 PDFDocumento123 pagineKS Bull 08 PDFfacistsdarkshadowNessuna valutazione finora
- Management Chapter 2Documento28 pagineManagement Chapter 2Sohaib RiazNessuna valutazione finora
- JD - Nomura Global Markets - BM - IIMK - v3 PDFDocumento3 pagineJD - Nomura Global Markets - BM - IIMK - v3 PDFRiturajPaulNessuna valutazione finora
- Career Counseling A Holistic Approach 9th Edition Zunker Test BankDocumento9 pagineCareer Counseling A Holistic Approach 9th Edition Zunker Test Bankdrkevinlee03071984jki100% (33)
- Stephan Strunz 2021 PDFDocumento24 pagineStephan Strunz 2021 PDFDevi Citra Ayu RahmawatiNessuna valutazione finora
- Enhancing Promotion and Career Prospects For Female Employees Student's Name Institutional Affiliation Professor's Name DateDocumento5 pagineEnhancing Promotion and Career Prospects For Female Employees Student's Name Institutional Affiliation Professor's Name Datekenneth kimathiNessuna valutazione finora