Potrebbero piacerti anche
- Tablet 3Documento6 pagineTablet 3Nurul Hilma RidwanNessuna valutazione finora
- EN Uji Efektivitas Sediaan Gel Fraksi Etil PDFDocumento10 pagineEN Uji Efektivitas Sediaan Gel Fraksi Etil PDFNurul Hilma RidwanNessuna valutazione finora
- 251-Article Text-487-1-10-20180227Documento6 pagine251-Article Text-487-1-10-20180227Nurul Hilma RidwanNessuna valutazione finora
- Vitaminb6 PangbornDocumento5 pagineVitaminb6 PangbornRio MairsyaNessuna valutazione finora
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (73)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- Repair of Small Household Appliances and Power ToolsDocumento315 pagineRepair of Small Household Appliances and Power ToolsahmadnawazjaswalNessuna valutazione finora
- Life Buds: Audiophile Wireless Earbuds With Immersive Single Point Source AudioDocumento2 pagineLife Buds: Audiophile Wireless Earbuds With Immersive Single Point Source AudioCecy LucasNessuna valutazione finora
- Theories of International TradeDocumento33 pagineTheories of International Tradefrediz79Nessuna valutazione finora
- Sharp AR-C172M ServiceM EN PDFDocumento308 pagineSharp AR-C172M ServiceM EN PDFpiaggio_nrgNessuna valutazione finora
- GCE Composite 1306 v4 PDFDocumento28 pagineGCE Composite 1306 v4 PDFParapar ShammonNessuna valutazione finora
- Books Confirmation - Sem VII - 2020-2021 PDFDocumento17 pagineBooks Confirmation - Sem VII - 2020-2021 PDFRaj Kothari MNessuna valutazione finora
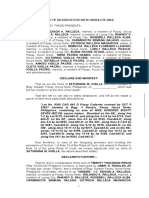
- DEED OF ADJUDICATION WITH ABSOLUTE SALE - VigillaDocumento3 pagineDEED OF ADJUDICATION WITH ABSOLUTE SALE - VigillaAlfred AglipayNessuna valutazione finora
- New Champlain Bridge: Final Report Summary (English)Documento82 pagineNew Champlain Bridge: Final Report Summary (English)andyrigaNessuna valutazione finora
- Arts Q1W3Documento44 pagineArts Q1W3LEILANI PELISIGASNessuna valutazione finora
- Case Analysis: A Simple Strategy at Costco: Informative Background InformationDocumento15 pagineCase Analysis: A Simple Strategy at Costco: Informative Background InformationFred Nazareno CerezoNessuna valutazione finora
- Rule: Steel Import Monitoring and Analysis SystemDocumento8 pagineRule: Steel Import Monitoring and Analysis SystemJustia.comNessuna valutazione finora
- Gas Agency Management SystemDocumento78 pagineGas Agency Management SystemManish Sharma100% (2)
- Batch 2 SEC Online Test AnswersDocumento5 pagineBatch 2 SEC Online Test AnswersBhairav YouthsNessuna valutazione finora
- 70 Fernando Medical Enterprise Vs Wesleyan University PDFDocumento2 pagine70 Fernando Medical Enterprise Vs Wesleyan University PDFTon Ton CananeaNessuna valutazione finora
- Bureau of Indian Standards Conformity Assessment Scheme For Milk and Milk ProductsDocumento51 pagineBureau of Indian Standards Conformity Assessment Scheme For Milk and Milk Productsatvenu16160Nessuna valutazione finora
- MCQ Criminal Law 1Documento18 pagineMCQ Criminal Law 1Clark Vincent Ponla0% (1)
- Azhar Marketing Final PPRDocumento9 pagineAzhar Marketing Final PPRafnain rafiNessuna valutazione finora
- T8 B20 NEADS Trip 2 of 3 FDR - Transcript - NEADS Rome NY - DRM 2 - Dat 2 - PG 1-83 - Color-CodedDocumento83 pagineT8 B20 NEADS Trip 2 of 3 FDR - Transcript - NEADS Rome NY - DRM 2 - Dat 2 - PG 1-83 - Color-Coded9/11 Document ArchiveNessuna valutazione finora
- 213-Article Text-620-1-10-20201118Documento6 pagine213-Article Text-620-1-10-20201118Arlin FebriantiNessuna valutazione finora
- The History of The Evening NewsDocumento14 pagineThe History of The Evening NewsWaqas MahmoodNessuna valutazione finora
- Towards Improvement of The Rights and Duties of Mutawalli and Nazir in The Management And..Documento17 pagineTowards Improvement of The Rights and Duties of Mutawalli and Nazir in The Management And..Mutqinah SshiNessuna valutazione finora
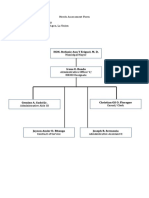
- Needs Assessment Form Company Name: HRMO Address: Sta. Barbara Agoo, La UnionDocumento2 pagineNeeds Assessment Form Company Name: HRMO Address: Sta. Barbara Agoo, La UnionAlvin LaroyaNessuna valutazione finora
- Programa de Formacion: English Dot Works 2Documento4 paginePrograma de Formacion: English Dot Works 2Juan GuerreroNessuna valutazione finora
- The Effect of Cross-Cultural Management On The Performance of Multinational Companies in NigeriaDocumento13 pagineThe Effect of Cross-Cultural Management On The Performance of Multinational Companies in NigeriaPreethu GowdaNessuna valutazione finora
- Philippine Metal Foundries v. CADocumento2 paginePhilippine Metal Foundries v. CAMarcus AureliusNessuna valutazione finora
- Doctrine of Indoor ManagementDocumento4 pagineDoctrine of Indoor ManagementRavi KtNessuna valutazione finora
- BBBB - View ReservationDocumento2 pagineBBBB - View ReservationBashir Ahmad BashirNessuna valutazione finora
- Mba Mini Project ReportDocumento32 pagineMba Mini Project ReportAvneesh KumarNessuna valutazione finora
- Lululemon Sample Case AnalysisDocumento49 pagineLululemon Sample Case AnalysisMai Ngoc PhamNessuna valutazione finora
- National Population PolicyDocumento12 pagineNational Population Policymuthukumar100% (3)