Potrebbero piacerti anche
- Cyanotic Heart DiseaseDocumento47 pagineCyanotic Heart Disease87-Saranya MNessuna valutazione finora
- Right Sided Heart FailureDocumento33 pagineRight Sided Heart FailurePaulNessuna valutazione finora
- Cardiovascular Disorders 2Documento78 pagineCardiovascular Disorders 2Erlinda SagadsadNessuna valutazione finora
- Heart Failure: Presented By: Leslie PaguioDocumento38 pagineHeart Failure: Presented By: Leslie PaguioLeslie PaguioNessuna valutazione finora
- Approach To Diagnosis of Congenital Heart DiseasesDocumento85 pagineApproach To Diagnosis of Congenital Heart DiseasesNirav CHOVATIYANessuna valutazione finora
- Congestive Heart FailureDocumento10 pagineCongestive Heart FailurekarenbelnasNessuna valutazione finora
- Case Study: Congestive Heart FailureDocumento7 pagineCase Study: Congestive Heart FailureXI-E / 21 / MARY TRIANANessuna valutazione finora
- 1 - CHDDocumento41 pagine1 - CHDأمـل .Nessuna valutazione finora
- CVS Examination Key PointsDocumento84 pagineCVS Examination Key PointsPrasenjit DasNessuna valutazione finora
- Congenital Cyanotic Heart DiseaseDocumento26 pagineCongenital Cyanotic Heart DiseaseAlokh Saha Raj100% (1)
- Cardiac Heart Failure Guide: Causes, Symptoms & Nursing CareDocumento43 pagineCardiac Heart Failure Guide: Causes, Symptoms & Nursing CareCindy DeliaNessuna valutazione finora
- Understanding Cyanotic Heart DefectsDocumento88 pagineUnderstanding Cyanotic Heart DefectsleenaNessuna valutazione finora
- Heart Failure PAED 604 2023 VileshDocumento34 pagineHeart Failure PAED 604 2023 VileshAvneelNessuna valutazione finora
- V. Complications of CVDDocumento26 pagineV. Complications of CVDJan Federick BantayNessuna valutazione finora
- Cardio HaikuDocumento84 pagineCardio HaikugarifoNessuna valutazione finora
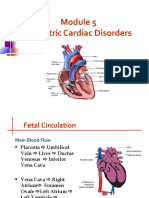
- Pediatric Cardiac Disorders: Fetal Circulation and Congestive Heart FailureDocumento62 paginePediatric Cardiac Disorders: Fetal Circulation and Congestive Heart FailureMarie Queenly Pagaran100% (1)
- CVS ExaminationDocumento85 pagineCVS ExaminationPrasenjit DasNessuna valutazione finora
- Heart Failure RecoveredDocumento43 pagineHeart Failure Recoveredرعد النميريNessuna valutazione finora
- 4 - Heart FailureDocumento20 pagine4 - Heart FailureYuji TanakaNessuna valutazione finora
- PBL-1 (Blue Baby)Documento7 paginePBL-1 (Blue Baby)haniyaayazNessuna valutazione finora
- Pericardial Diseases - Raghad DghaishDocumento32 paginePericardial Diseases - Raghad Dghaish180045Nessuna valutazione finora
- Acynotic DiseaseDocumento55 pagineAcynotic DiseaseTesfamichael AbathunNessuna valutazione finora
- Case Presentation: Congenital Heart DiseaseDocumento37 pagineCase Presentation: Congenital Heart DiseaseKarin Nadia UtamiNessuna valutazione finora
- Congenital Heart DefectsDocumento45 pagineCongenital Heart Defectskathylaine100% (1)
- Cardiovascular DisorderDocumento40 pagineCardiovascular DisorderAmy Del CarmenNessuna valutazione finora
- Heart FailureDocumento4 pagineHeart FailureDane WrightNessuna valutazione finora
- Heart Failure GuideDocumento8 pagineHeart Failure GuideAikoP.NarcisoNessuna valutazione finora
- CHFSP 2005Documento36 pagineCHFSP 2005Andy F MonroeNessuna valutazione finora
- Hypertension For EMS ProvidersDocumento35 pagineHypertension For EMS ProvidersPaulhotvw67100% (5)
- Congenital Heart Disease: Hema Rajendran B.SC (N) NICU Staff NurseDocumento23 pagineCongenital Heart Disease: Hema Rajendran B.SC (N) NICU Staff NurseddNessuna valutazione finora
- Heart Failure Symptoms and SignsDocumento11 pagineHeart Failure Symptoms and SignsRubie Ann TillorNessuna valutazione finora
- By: Darryl Jamison Macon County EMS Training CoordinatorDocumento53 pagineBy: Darryl Jamison Macon County EMS Training Coordinatorsharin143Nessuna valutazione finora
- Congenital Heart DiseasesDocumento14 pagineCongenital Heart DiseasesEulane Ferrer100% (1)
- Heart Failure Lecture 6Documento39 pagineHeart Failure Lecture 6Nithin SureshNessuna valutazione finora
- NCM 102 Pedia Congestive Heart FailureDocumento184 pagineNCM 102 Pedia Congestive Heart FailureKevin CamilozaNessuna valutazione finora
- Valvular Heart Disease GuideDocumento43 pagineValvular Heart Disease Guideurmila prajapatiNessuna valutazione finora
- Acynotic Heart DiseasesDocumento13 pagineAcynotic Heart DiseasesSimran JosanNessuna valutazione finora
- 01 Cardiovascular IDocumento72 pagine01 Cardiovascular IcoriezaNessuna valutazione finora
- Cardiovascular HO Final GROUP2Documento72 pagineCardiovascular HO Final GROUP2Siraj ShiferawNessuna valutazione finora
- Cardiac Tamponade (Suryani)Documento72 pagineCardiac Tamponade (Suryani)Hamdani UsmanNessuna valutazione finora
- Congestive Heart Failure PDFDocumento11 pagineCongestive Heart Failure PDFpriyanka bhavsarNessuna valutazione finora
- 9, CHF BestDocumento43 pagine9, CHF BestauNessuna valutazione finora
- CME Cyanotic Heart DiseaseDocumento38 pagineCME Cyanotic Heart DiseaseTan Zhi HongNessuna valutazione finora
- Congenital Heart DiseasesDocumento27 pagineCongenital Heart DiseasesJumar ValdezNessuna valutazione finora
- Heart Failure: Presentation by Dr. Tooba ShahbazDocumento30 pagineHeart Failure: Presentation by Dr. Tooba ShahbazTooba ShahbazNessuna valutazione finora
- Heart FailureDocumento44 pagineHeart FailureHarold DiasanaNessuna valutazione finora
- Unit 2 Cardiovasular SystemDocumento49 pagineUnit 2 Cardiovasular SystemdhanashriNessuna valutazione finora
- Heart Failure by IvsDocumento66 pagineHeart Failure by IvsArianne LasamNessuna valutazione finora
- Paeds CardioDocumento28 paginePaeds CardioIman ZalzilahNessuna valutazione finora
- ucu-CHDs_240114_230618 (2)Documento68 pagineucu-CHDs_240114_230618 (2)BrianNessuna valutazione finora
- Heart FailureDocumento44 pagineHeart FailureSalman Habeeb100% (6)
- Congestive Heart FailureDocumento39 pagineCongestive Heart FailureEthiopia TekdemNessuna valutazione finora
- (I..) KMU Peads CardicDocumento88 pagine(I..) KMU Peads CardicMuhammadNessuna valutazione finora
- Congenital Heart DiseasesDocumento121 pagineCongenital Heart DiseasesJayvee V. De GuzmanNessuna valutazione finora
- Case PresentationDocumento16 pagineCase PresentationAnuja NairNessuna valutazione finora
- Cardiovascular DiseasesDocumento4 pagineCardiovascular DiseasesAshley Nicole LimNessuna valutazione finora
- Congenital Heart DiseaseDocumento38 pagineCongenital Heart DiseaseSnIP StandredNessuna valutazione finora
- Medicine in Brief: Name the Disease in Haiku, Tanka and ArtDa EverandMedicine in Brief: Name the Disease in Haiku, Tanka and ArtValutazione: 5 su 5 stelle5/5 (1)
- Fluid and Electrolytes for Nursing StudentsDa EverandFluid and Electrolytes for Nursing StudentsValutazione: 5 su 5 stelle5/5 (12)
- The Ideal Heart Healthy Diet Cookbook; The Superb Diet Guide To Lower Your Blood Pressure And Cholesterol Levels With Nutritious Low Sodium Low Fat RecipesDa EverandThe Ideal Heart Healthy Diet Cookbook; The Superb Diet Guide To Lower Your Blood Pressure And Cholesterol Levels With Nutritious Low Sodium Low Fat RecipesNessuna valutazione finora
- Renal Disease Diet PlansDocumento7 pagineRenal Disease Diet Plansnicoleangela ubasroselloNessuna valutazione finora
- Ruminal Acidosis.pdf - Google ДискDocumento56 pagineRuminal Acidosis.pdf - Google ДискDVM 700Nessuna valutazione finora
- NEBOSH HSE Certification in Health and Safety Leadership ExcellenceDocumento18 pagineNEBOSH HSE Certification in Health and Safety Leadership ExcellenceRahul Siwakoti100% (1)
- No Hipertensi Harga (RP) PaketDocumento2 pagineNo Hipertensi Harga (RP) PaketVania Azalia HariyantoNessuna valutazione finora
- Carlosa Es Localized Child Protection PolicyDocumento9 pagineCarlosa Es Localized Child Protection PolicymonalisaNessuna valutazione finora
- Dopunska Lista Lijekova - Po Dijelovima - Web - Stupa Na Snagu - 23 - 06 - 2022Documento256 pagineDopunska Lista Lijekova - Po Dijelovima - Web - Stupa Na Snagu - 23 - 06 - 2022Alma FazlićNessuna valutazione finora
- KHDA - Dar Al Marefa School 2016-2017Documento27 pagineKHDA - Dar Al Marefa School 2016-2017Edarabia.comNessuna valutazione finora
- Dukungan Leadership-LEAN - PPNIDocumento34 pagineDukungan Leadership-LEAN - PPNIBUKU PASIENNessuna valutazione finora
- 952-Article Text-3024-1-10-20221113Documento13 pagine952-Article Text-3024-1-10-20221113Audi GaluhNessuna valutazione finora
- Activity-Based Implementation and Evaluation Plan Summary (Used As SETT Scaffold For Implementation and Evaluation Planning)Documento1 paginaActivity-Based Implementation and Evaluation Plan Summary (Used As SETT Scaffold For Implementation and Evaluation Planning)api-289181874Nessuna valutazione finora
- Thesis On Stress in The WorkplaceDocumento6 pagineThesis On Stress in The WorkplaceScott Donald100% (2)
- History of Movement EducationDocumento4 pagineHistory of Movement EducationMark FernandezNessuna valutazione finora
- AI Ethics: Paula BoddingtonDocumento531 pagineAI Ethics: Paula Boddingtontony pauloNessuna valutazione finora
- Security Assessment &recommendation: PurposeDocumento3 pagineSecurity Assessment &recommendation: PurposeEricka W.Nessuna valutazione finora
- Pilot II: Technical Data SheetDocumento4 paginePilot II: Technical Data SheetSafinahNessuna valutazione finora
- BBMP Birth & Death Certificate FAQsDocumento4 pagineBBMP Birth & Death Certificate FAQsindian250% (1)
- Complementary and Alternative Medicine Bodies, Therapies, Senses (Ruth Barcan)Documento211 pagineComplementary and Alternative Medicine Bodies, Therapies, Senses (Ruth Barcan)lilahgreeny100% (1)
- HBS Cases - Branding YogaDocumento6 pagineHBS Cases - Branding YogaPraveenNessuna valutazione finora
- Module 1 Activity Small Group Discussion Views Homeostasis PDFDocumento6 pagineModule 1 Activity Small Group Discussion Views Homeostasis PDFJosh MagatNessuna valutazione finora
- OPTIMIZE GROUND OPERATIONSDocumento3 pagineOPTIMIZE GROUND OPERATIONSAshwin Leonard100% (3)
- Healing Wonders AppDocumento18 pagineHealing Wonders AppJoanna Atrisk C-LealNessuna valutazione finora
- Paranoid SNDocumento3 pagineParanoid SNmalindaNessuna valutazione finora
- Consensus Statements Febrile SeizuresDocumento7 pagineConsensus Statements Febrile SeizuresMattNessuna valutazione finora
- Limulus Amebocyte Lysate Test (LAL)Documento16 pagineLimulus Amebocyte Lysate Test (LAL)Shahriar ShamimNessuna valutazione finora
- Community Engagement Module 3 Quarter 1 Types of Communities and DifferencesDocumento32 pagineCommunity Engagement Module 3 Quarter 1 Types of Communities and DifferencesROGER88% (33)
- Improve Patient Safety by Reducing Medication ErrorsDocumento95 pagineImprove Patient Safety by Reducing Medication Errorsdev5683Nessuna valutazione finora
- Kritik jurnal kuantitatif surveyDocumento18 pagineKritik jurnal kuantitatif surveyLuthi PratiwiNessuna valutazione finora
- Asthma Guidelines in Philippines PDFDocumento91 pagineAsthma Guidelines in Philippines PDFxtine100% (2)
- Sample Assessment Functional Health PatternsDocumento2 pagineSample Assessment Functional Health Patternskezia_lillyNessuna valutazione finora
- Surgical Intern Manual (For Pre-Intern) QEHDocumento10 pagineSurgical Intern Manual (For Pre-Intern) QEHChris Jardine LiNessuna valutazione finora