Potrebbero piacerti anche
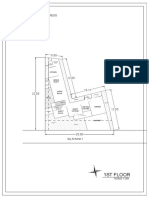
- 1St Floor: House On Paus Schematic Plan ProgressDocumento2 pagine1St Floor: House On Paus Schematic Plan Progressfiora.ladesvitaNessuna valutazione finora
- Gibson 2010Documento19 pagineGibson 2010fiora.ladesvitaNessuna valutazione finora
- Determinants of Delay in Care Seeking Among Children Under Five With Fever in Dodoma Region, Central Tanzania: A Cross-Sectional StudyDocumento10 pagineDeterminants of Delay in Care Seeking Among Children Under Five With Fever in Dodoma Region, Central Tanzania: A Cross-Sectional Studyfiora.ladesvitaNessuna valutazione finora
- Sex Differences in Cancer Risk and Survival: A Swedish Cohort StudyDocumento11 pagineSex Differences in Cancer Risk and Survival: A Swedish Cohort Studyfiora.ladesvitaNessuna valutazione finora
- Childhood Illness Prevalence and Health Seeking Behavior Patterns in Rural TanzaniaDocumento12 pagineChildhood Illness Prevalence and Health Seeking Behavior Patterns in Rural Tanzaniafiora.ladesvitaNessuna valutazione finora
- 2015 Conference 10Documento11 pagine2015 Conference 10fiora.ladesvitaNessuna valutazione finora
- Medicalscience: EcancerDocumento7 pagineMedicalscience: Ecancerfiora.ladesvitaNessuna valutazione finora
- Caring: Prof. Dr. Budi Anna Keliat, MappscDocumento59 pagineCaring: Prof. Dr. Budi Anna Keliat, Mappscfiora.ladesvitaNessuna valutazione finora
- Ambulatory Care Nursing: Coming Soon!Documento16 pagineAmbulatory Care Nursing: Coming Soon!fiora.ladesvitaNessuna valutazione finora
- Assessment Rating ScaleDocumento8 pagineAssessment Rating Scalefiora.ladesvitaNessuna valutazione finora
- Anderson2004 PDFDocumento7 pagineAnderson2004 PDFfiora.ladesvitaNessuna valutazione finora
- Sistematic Review HoneyDocumento159 pagineSistematic Review Honeyfiora.ladesvitaNessuna valutazione finora
- Living With Kidney DiseaseDocumento96 pagineLiving With Kidney Diseasefiora.ladesvitaNessuna valutazione finora
- Idiom Meaning Examples: Toefl PreparationDocumento4 pagineIdiom Meaning Examples: Toefl Preparationfiora.ladesvitaNessuna valutazione finora
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (74)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- Chapter 20 Extrahepatic Biliary Tract and Gall BladderDocumento63 pagineChapter 20 Extrahepatic Biliary Tract and Gall BladderMACON824Nessuna valutazione finora
- Clinical Manifestations and Assessment of Respiratory Disease 5th Edition Jardins Test BankDocumento9 pagineClinical Manifestations and Assessment of Respiratory Disease 5th Edition Jardins Test Banksarahpalmerotpdkjcwfq100% (26)
- General Census Nov 13Documento8 pagineGeneral Census Nov 13Mark Angelo PonferradoNessuna valutazione finora
- KOICA Application FormDocumento12 pagineKOICA Application Formdeni100% (1)
- Oxoid 2012-13Documento84 pagineOxoid 2012-13Athar AbbasNessuna valutazione finora
- Nutrition in Neurosurgery 2Documento13 pagineNutrition in Neurosurgery 2Mimakos CyberNessuna valutazione finora
- Rds CaseDocumento42 pagineRds Casegebby puspitaNessuna valutazione finora
- Counselling Plab2Aspired19Documento137 pagineCounselling Plab2Aspired19osamaeNessuna valutazione finora
- PCORI Methodology Standards Curriculum Research Questions 3Documento13 paginePCORI Methodology Standards Curriculum Research Questions 3Krizele Acu PagalananNessuna valutazione finora
- Intracardiac Epinephrine Injection During Open Thoracotomy and Circulatory Arrest 2155 6148.1000341Documento2 pagineIntracardiac Epinephrine Injection During Open Thoracotomy and Circulatory Arrest 2155 6148.1000341samuelNessuna valutazione finora
- Pyle Et Al 1995 - Rapid Direct Count E ColiDocumento7 paginePyle Et Al 1995 - Rapid Direct Count E ColiFabio SenaNessuna valutazione finora
- Module 6 IPM & Harmful Effect of Chemical Pesticides.Documento6 pagineModule 6 IPM & Harmful Effect of Chemical Pesticides.Nikhil BijuNessuna valutazione finora
- Failure of Endoscopic Spine SurgeryDocumento6 pagineFailure of Endoscopic Spine SurgeryKaustubh KeskarNessuna valutazione finora
- History of MicrobiologyDocumento5 pagineHistory of MicrobiologyBernadine EliseNessuna valutazione finora
- Worksheet For Perception CoordinationDocumento7 pagineWorksheet For Perception CoordinationRiza Angela BarazanNessuna valutazione finora
- HSC 421 Research PaperDocumento13 pagineHSC 421 Research Paperapi-502687231Nessuna valutazione finora
- Test Bank For College Algebra 12Th Edition by Lial Hornsby Schneider and Daniels Isbn 0134217454 978013421745 Full Chapter PDFDocumento36 pagineTest Bank For College Algebra 12Th Edition by Lial Hornsby Schneider and Daniels Isbn 0134217454 978013421745 Full Chapter PDFdavid.weldon592100% (12)
- Part I: Medical Microbiology Part II: Medical ParasitologyDocumento36 paginePart I: Medical Microbiology Part II: Medical ParasitologyRamakrishna ShanbhogeNessuna valutazione finora
- Presentation4 PDFDocumento36 paginePresentation4 PDFKARISHMA PATHANNessuna valutazione finora
- General Nursing Science 1 2020 PDFDocumento95 pagineGeneral Nursing Science 1 2020 PDFRicardo DomingosNessuna valutazione finora
- Nursing Diagnosis: Risk For Deficient Fluid Volume R/T Traumatic InjuryDocumento2 pagineNursing Diagnosis: Risk For Deficient Fluid Volume R/T Traumatic Injuryarreane yookNessuna valutazione finora
- Chapter 17 Unit IDocumento23 pagineChapter 17 Unit IGlory MimiNessuna valutazione finora
- ICU MSC Logbook-FinalDocumento101 pagineICU MSC Logbook-FinalCwali MohamedNessuna valutazione finora
- 1 s2.0 S2772594422001637 MainDocumento5 pagine1 s2.0 S2772594422001637 MainCatarina CourasNessuna valutazione finora
- Zigmond MJ, Burke RE - Pathophysiology of Parkinson's DiseaseDocumento14 pagineZigmond MJ, Burke RE - Pathophysiology of Parkinson's Diseaseursula_ursula100% (1)
- 1010 Research Paper 1Documento10 pagine1010 Research Paper 1api-442331287Nessuna valutazione finora
- Drug - WikipediaDocumento4 pagineDrug - WikipedianightmareNessuna valutazione finora
- Narcolepsy - Pathophysiology, Diagnosis and Treatment (Ed. Baumann, Bassetti, Scammell)Documento416 pagineNarcolepsy - Pathophysiology, Diagnosis and Treatment (Ed. Baumann, Bassetti, Scammell)kittygotclaws100% (1)
- Grade 6 DLL English 6 q4 Week 3Documento5 pagineGrade 6 DLL English 6 q4 Week 3Evan Mae LutchaNessuna valutazione finora
- Bioinformatics DatabaseDocumento50 pagineBioinformatics DatabasedhanushumakanthaNessuna valutazione finora