Potrebbero piacerti anche
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (587)
- JSCBXCCGHXJBNCB JHNN XHDCJDocumento1 paginaJSCBXCCGHXJBNCB JHNN XHDCJNilaFitriOlaNessuna valutazione finora
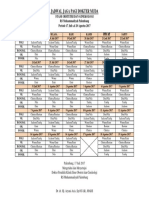
- Jadwal Jaga Pagi Dokter Muda: Stase Obstetri Dan Ginekologi RS Muhammadiyah Palembang Periode 17 Juli S.D 20 Agustus 2017Documento1 paginaJadwal Jaga Pagi Dokter Muda: Stase Obstetri Dan Ginekologi RS Muhammadiyah Palembang Periode 17 Juli S.D 20 Agustus 2017NilaFitriOlaNessuna valutazione finora
- XXZDocumento1 paginaXXZNilaFitriOlaNessuna valutazione finora
- Dapus RadDocumento2 pagineDapus RadNilaFitriOlaNessuna valutazione finora
- Follow Up TanggDocumento6 pagineFollow Up TanggNilaFitriOlaNessuna valutazione finora
- Follow Up TanggDocumento6 pagineFollow Up TanggNilaFitriOlaNessuna valutazione finora
- Dapus RadDocumento2 pagineDapus RadNilaFitriOlaNessuna valutazione finora
- Jco 2015 60 9347Documento10 pagineJco 2015 60 9347NilaFitriOlaNessuna valutazione finora
- Diagnosis Management AndPreventionofRabiesDocumento10 pagineDiagnosis Management AndPreventionofRabiesNilaFitriOlaNessuna valutazione finora
- Daftar PustakaDocumento2 pagineDaftar PustakaRetza Prawira PutraNessuna valutazione finora
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (399)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (73)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2219)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (265)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (119)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- Aurum Metallicum - Picture of A Homeopathic RemedyDocumento8 pagineAurum Metallicum - Picture of A Homeopathic Remedyisadore71% (7)
- Top 10 Pharma Companies in India 2022Documento8 pagineTop 10 Pharma Companies in India 2022Royal MarathaNessuna valutazione finora
- Pahs Mbbs Information BookletDocumento18 paginePahs Mbbs Information BookletKishor BajgainNessuna valutazione finora
- ArrhythmiaDocumento31 pagineArrhythmiaAbdallah Essam Al-ZireeniNessuna valutazione finora
- XxssDocumento13 pagineXxssfkhunc07Nessuna valutazione finora
- Cir 0000000000000899Documento25 pagineCir 0000000000000899hanifa ambNessuna valutazione finora
- CPR and Aed: Quiz #2 ResultsDocumento2 pagineCPR and Aed: Quiz #2 ResultsNathan WhiteNessuna valutazione finora
- Try Out Paket BDocumento13 pagineTry Out Paket BDian Purnama Dp'TmNessuna valutazione finora
- Types of Casts and Their IndicationsDocumento3 pagineTypes of Casts and Their IndicationsPhylum ChordataNessuna valutazione finora
- Cure - Family Health MatterzDocumento14 pagineCure - Family Health MatterzGeorge AniborNessuna valutazione finora
- A Case-Based Guide To Clinical Endocrinology (October 23, 2015) - (1493920588) - (Springer)Documento434 pagineA Case-Based Guide To Clinical Endocrinology (October 23, 2015) - (1493920588) - (Springer)AbdulraHman KhalEd100% (2)
- Atlas de Acupuntura (Ingles)Documento16 pagineAtlas de Acupuntura (Ingles)Medicina Tradicional China - Grupo LeNessuna valutazione finora
- Framingham Risk Score SaDocumento8 pagineFramingham Risk Score Saapi-301624030Nessuna valutazione finora
- IMSS Nursing Knowledge ExamDocumento11 pagineIMSS Nursing Knowledge ExamScribdTranslationsNessuna valutazione finora
- Smell & TasteDocumento4 pagineSmell & Tasteminji_DNessuna valutazione finora
- Sample 20715Documento16 pagineSample 20715Sachin KumarNessuna valutazione finora
- Maximum Marks: 100Documento35 pagineMaximum Marks: 100Yu HoyanNessuna valutazione finora
- Mink Dissection InstructionsDocumento15 pagineMink Dissection InstructionsMark PenticuffNessuna valutazione finora
- Boys Centile ChartDocumento1 paginaBoys Centile ChartElma AprilliaNessuna valutazione finora
- Minimizing Social Desirability Bias in Measuring Sensitive Topics: The Use of Forgiving Language in Item DevelopmentDocumento14 pagineMinimizing Social Desirability Bias in Measuring Sensitive Topics: The Use of Forgiving Language in Item DevelopmentKillariyPortugalNessuna valutazione finora
- 12-Channel ECG SpecsDocumento5 pagine12-Channel ECG SpecsNai PaniaiNessuna valutazione finora
- Study The Herbalism of Thyme LeavesDocumento7 pagineStudy The Herbalism of Thyme Leavespronto4meNessuna valutazione finora
- A Brief History of Evidence-Based Medicine in Four PeriodsDocumento31 pagineA Brief History of Evidence-Based Medicine in Four PeriodsSaad MotawéaNessuna valutazione finora
- Dressing and BandagingDocumento5 pagineDressing and BandagingMaricar Gallamora Dela CruzNessuna valutazione finora
- Young FrankensteinDocumento109 pagineYoung FrankensteinColleen Hawks-Pierce83% (6)
- How to prepare your Asil for fightingDocumento16 pagineHow to prepare your Asil for fightingcinna01Nessuna valutazione finora
- Zingiber Officinale MonographDocumento5 pagineZingiber Officinale Monographc_j_bhattNessuna valutazione finora
- NCP OrthoDocumento2 pagineNCP OrthoJeyser T. GamutiaNessuna valutazione finora
- Isolating Staphylococcus SPDocumento4 pagineIsolating Staphylococcus SPHani HairullaNessuna valutazione finora
- Ducharme Et Al, 1996Documento20 pagineDucharme Et Al, 1996GokushimakNessuna valutazione finora