Potrebbero piacerti anche
- Digitalization in Dentistry CADCAM A ReviewDocumento6 pagineDigitalization in Dentistry CADCAM A ReviewnabeghNessuna valutazione finora
- Computer-Aided Designing and Computer-Aided Manufacturing in ProsthodonticsDocumento60 pagineComputer-Aided Designing and Computer-Aided Manufacturing in Prosthodonticsreshma shaikNessuna valutazione finora
- Cad Cam ReviewDocumento5 pagineCad Cam ReviewnabeghNessuna valutazione finora
- Precision of Intraoral Digital Dental Impressions With ITero and Extraoral Digitization With The ITero and A Model ScannerDocumento8 paginePrecision of Intraoral Digital Dental Impressions With ITero and Extraoral Digitization With The ITero and A Model ScannerAlex BurdeNessuna valutazione finora
- Digital Impressions A New Era in ProsthodonticsDocumento3 pagineDigital Impressions A New Era in Prosthodonticsaziz2007Nessuna valutazione finora
- Is CBCT Necessary For Implant PlacementDocumento5 pagineIs CBCT Necessary For Implant PlacementcopyourpairNessuna valutazione finora
- Digitalalisation in Dentistry PDFDocumento19 pagineDigitalalisation in Dentistry PDF林元敏Nessuna valutazione finora
- PeekDocumento8 paginePeeksalmaNessuna valutazione finora
- IPS E.maxDocumento32 pagineIPS E.maxKhaled ElshabrawyNessuna valutazione finora
- Digital WorkflowsDocumento14 pagineDigital Workflowsmoji_puiNessuna valutazione finora
- Product Focus Implant Overdentures With The LOCATOR Attachment Free Standing Versus Bar ApplicationsDocumento3 pagineProduct Focus Implant Overdentures With The LOCATOR Attachment Free Standing Versus Bar ApplicationsDentalLearningNessuna valutazione finora
- Iti ImplantDocumento8 pagineIti ImplantMuaiyed Buzayan AkremyNessuna valutazione finora
- ZirconiaDocumento8 pagineZirconiaAmitNessuna valutazione finora
- Jung 2018Documento11 pagineJung 2018Sebastien MelloulNessuna valutazione finora
- CAD/CAM Dentistry and Chairside Digital Impression Making: 4 CE CreditsDocumento11 pagineCAD/CAM Dentistry and Chairside Digital Impression Making: 4 CE CreditsShraddha AgarwalNessuna valutazione finora
- IDD CAD CAM Intraoral Scanner Reviews IDS 2019 May UpdateDocumento30 pagineIDD CAD CAM Intraoral Scanner Reviews IDS 2019 May UpdateAndrew VillanuevaNessuna valutazione finora
- Avadent Article Loma LindaDocumento8 pagineAvadent Article Loma LindaRoxana LupuNessuna valutazione finora
- Digital Technologies in DentistryDocumento96 pagineDigital Technologies in Dentistryابو سارةNessuna valutazione finora
- Additive Manufacturing Techniques in Prosthodontics Where Do We Currently Stand A Critical ReviewDocumento11 pagineAdditive Manufacturing Techniques in Prosthodontics Where Do We Currently Stand A Critical ReviewAlex BurdeNessuna valutazione finora
- Rapid Prototyping ReviewDocumento10 pagineRapid Prototyping ReviewvarunNessuna valutazione finora
- 3 D PrintingDocumento4 pagine3 D PrintingProsthodontics DeptNessuna valutazione finora
- Magnification and IlluminationDocumento22 pagineMagnification and Illuminationwhussien7376100% (1)
- Orthodontic Removable AppliancesDocumento159 pagineOrthodontic Removable AppliancesMichaelNessuna valutazione finora
- Porcelain Fused To Metal (PFM) Crowns and Caries in Adjacent TeetDocumento5 paginePorcelain Fused To Metal (PFM) Crowns and Caries in Adjacent Teetbaiq rengganis dewiNessuna valutazione finora
- Functional OcclusionDocumento8 pagineFunctional OcclusionNoor SolikhahNessuna valutazione finora
- Cone-Beam Computer TomographyDocumento79 pagineCone-Beam Computer Tomographyjohn suryavardhan100% (1)
- Cad CamDocumento5 pagineCad CamsauriuaNessuna valutazione finora
- All-On-4, For PatientsDocumento28 pagineAll-On-4, For PatientsmmsbabakNessuna valutazione finora
- DENTURES Urs VladimirDocumento7 pagineDENTURES Urs VladimircristianNessuna valutazione finora
- Applied Anatomy Related To Complete Denture-Maxilla MandibleDocumento57 pagineApplied Anatomy Related To Complete Denture-Maxilla MandibleRen Jye ChongNessuna valutazione finora
- Occlusal Considerations in ImplantDocumento11 pagineOcclusal Considerations in ImplantRolzilah RohaniNessuna valutazione finora
- Concepts of Arrangement of Artifical Teeth, SelectiveDocumento7 pagineConcepts of Arrangement of Artifical Teeth, SelectiveAmar BhochhibhoyaNessuna valutazione finora
- A Clinical Guide To Orthodontics - J. Sandy (2004) WW PDFDocumento77 pagineA Clinical Guide To Orthodontics - J. Sandy (2004) WW PDFAntonela CeremușNessuna valutazione finora
- Atraumatic Restorative Treatment: Restorative ComponentDocumento11 pagineAtraumatic Restorative Treatment: Restorative ComponentYu Yu Victor ChienNessuna valutazione finora
- Esthetic Analysis of The SmileDocumento7 pagineEsthetic Analysis of The SmileNitin H.c.Nessuna valutazione finora
- Does Platform Switching Really Prevent Crestal Bone Loss Around Implants?Documento46 pagineDoes Platform Switching Really Prevent Crestal Bone Loss Around Implants?manujohnsNessuna valutazione finora
- Digital Wax Up in DentistryDocumento14 pagineDigital Wax Up in Dentistrybanea costin100% (1)
- Advance in MaterialsDocumento10 pagineAdvance in Materialssami robalinoNessuna valutazione finora
- Immediate Complete Denture ImpressionsDocumento12 pagineImmediate Complete Denture ImpressionsToDownload81Nessuna valutazione finora
- Use of Operating Microscope in EndodonticsDocumento42 pagineUse of Operating Microscope in Endodonticsgiribarch100% (1)
- Prosthetic Complication of Dental ImplantsDocumento42 pagineProsthetic Complication of Dental ImplantsDr. Abdulsalam Awas Dental Center0% (1)
- 2 Straumann Implants TLDocumento41 pagine2 Straumann Implants TLjoephinNessuna valutazione finora
- 1proteza Partiala Mobilizabila, Nevoia Clinica de Inovare 2017 Journal of Prosthetic DentistryDocumento8 pagine1proteza Partiala Mobilizabila, Nevoia Clinica de Inovare 2017 Journal of Prosthetic DentistrydanielaNessuna valutazione finora
- History of ProsthodonticsDocumento121 pagineHistory of ProsthodonticsArthi Ramalingam aNessuna valutazione finora
- Periodontal Plastic and Esthetic SurgeryDocumento173 paginePeriodontal Plastic and Esthetic SurgerySaman MohammadzadehNessuna valutazione finora
- MVT Varsitile +Documento28 pagineMVT Varsitile +drimtiyaz123Nessuna valutazione finora
- Vsip - Info - Anterior Wax Up PDF Free PDFDocumento3 pagineVsip - Info - Anterior Wax Up PDF Free PDFMekideche dental officeNessuna valutazione finora
- 2003-09 Magnification (Endod. Practice)Documento8 pagine2003-09 Magnification (Endod. Practice)Puscas IulianaNessuna valutazione finora
- Review Peek PDFDocumento11 pagineReview Peek PDFAlexandra Dumitrache100% (1)
- Surgical EndoDocumento16 pagineSurgical EndoTraian IlieNessuna valutazione finora
- Fixed Orthodontic Appliances: A Practical GuideDa EverandFixed Orthodontic Appliances: A Practical GuideValutazione: 1 su 5 stelle1/5 (1)
- Titanium in Dentistry: Historical Uses, Current Applications, and Future OutlookDocumento7 pagineTitanium in Dentistry: Historical Uses, Current Applications, and Future OutlookPabloNessuna valutazione finora
- 3d Printing in Fixed ProsthodonticsDocumento5 pagine3d Printing in Fixed ProsthodonticsCherifNessuna valutazione finora
- Cad/Cam Complete Dentures: A Review of Two Commercial: Fabrication SystemsDocumento10 pagineCad/Cam Complete Dentures: A Review of Two Commercial: Fabrication SystemsEugenStanciuNessuna valutazione finora
- Bopt PanizDocumento9 pagineBopt PanizIvan CarreraNessuna valutazione finora
- Increasing Vertical DimensionDocumento13 pagineIncreasing Vertical DimensionSiva KumarNessuna valutazione finora
- Anatomy, Modeling and Biomaterial Fabrication for Dental and Maxillofacial ApplicationsDa EverandAnatomy, Modeling and Biomaterial Fabrication for Dental and Maxillofacial ApplicationsNessuna valutazione finora
- Basic Level of Dental Resins - Material Science & Technology: 4th Edition, 2nd VersionDa EverandBasic Level of Dental Resins - Material Science & Technology: 4th Edition, 2nd VersionNessuna valutazione finora
- 3-Dent Update 2014 41 657-657Documento2 pagine3-Dent Update 2014 41 657-657Najeeb UllahNessuna valutazione finora
- An Overview of Preformed Metal Crown Part 1Documento5 pagineAn Overview of Preformed Metal Crown Part 1Najeeb UllahNessuna valutazione finora
- BridgesDocumento3 pagineBridgesNajeeb UllahNessuna valutazione finora
- 3-Dent Update 2014 41 657-657Documento2 pagine3-Dent Update 2014 41 657-657Najeeb UllahNessuna valutazione finora
- Alternativas A TotalesDocumento12 pagineAlternativas A TotalesJuan Jose Stuven RodriguezNessuna valutazione finora
- An Overview of Dental Adhesive Systems and The Dynamic Tooth-Adhesive InterfaceDocumento19 pagineAn Overview of Dental Adhesive Systems and The Dynamic Tooth-Adhesive InterfaceLynda M. NaranjoNessuna valutazione finora
- Occlusal therapy opinion leaderDocumento1 paginaOcclusal therapy opinion leaderNajeeb UllahNessuna valutazione finora
- Guidelines For A Minimum Acceptable Protocol For The Construction of Complete DenturesDocumento9 pagineGuidelines For A Minimum Acceptable Protocol For The Construction of Complete DenturesNajeeb UllahNessuna valutazione finora
- DR Dominic Leung - Connection of Dental Implants To Natural TeethDocumento62 pagineDR Dominic Leung - Connection of Dental Implants To Natural TeethNajeeb UllahNessuna valutazione finora
- Fundamentals of Occlusion Part 1Documento12 pagineFundamentals of Occlusion Part 1Najeeb UllahNessuna valutazione finora
- A Treatment Protocol For Restoring Occlusal Vertical Dimension Using An Overlay RPDDocumento6 pagineA Treatment Protocol For Restoring Occlusal Vertical Dimension Using An Overlay RPDFaheemuddin MuhammadNessuna valutazione finora
- Acetel ResinDocumento4 pagineAcetel ResinNajeeb UllahNessuna valutazione finora
- All Ceramic Inlays and Onlays For Posterior TeethDocumento11 pagineAll Ceramic Inlays and Onlays For Posterior TeethNajeeb Ullah100% (1)
- Occlusal Splints: Dr. Saloni Dalal, Dr. Omkar Shetty, Dr. Gaurang MistryDocumento6 pagineOcclusal Splints: Dr. Saloni Dalal, Dr. Omkar Shetty, Dr. Gaurang MistryNajeeb UllahNessuna valutazione finora
- Functional Crown Lengthening Surgery Periodontic and Prosthodontic ConsiderationsDocumento5 pagineFunctional Crown Lengthening Surgery Periodontic and Prosthodontic ConsiderationsNajeeb UllahNessuna valutazione finora
- Geriatric Oral HealthDocumento7 pagineGeriatric Oral HealthDevina VedayumnaNessuna valutazione finora
- Different Pontic Design For Porcelain Fused To Metal Fixed Dental Prosthesis: Contemporary Guidelines and Practice by General Dental PractitionersDocumento5 pagineDifferent Pontic Design For Porcelain Fused To Metal Fixed Dental Prosthesis: Contemporary Guidelines and Practice by General Dental PractitionersNajeeb UllahNessuna valutazione finora
- Oclusion Esquemas Oclusales PDFDocumento6 pagineOclusion Esquemas Oclusales PDFIlseNessuna valutazione finora
- Pakistan771 PDFDocumento2 paginePakistan771 PDFOmer EhsebNessuna valutazione finora
- Newapproachestopain Management: Orrett E. OgleDocumento10 pagineNewapproachestopain Management: Orrett E. OgleNajeeb UllahNessuna valutazione finora
- A Talon Cusp PDFDocumento3 pagineA Talon Cusp PDFNajeeb UllahNessuna valutazione finora
- Abutment Selection in Fixed Partial Denture - A Review: Drug Invention Today January 2018Documento6 pagineAbutment Selection in Fixed Partial Denture - A Review: Drug Invention Today January 2018Najeeb UllahNessuna valutazione finora
- The 100 Most Cited Articles in Prosthodontic Journals: A Bibliometric Analysis of Articles Published Between 1951 and 2019Documento7 pagineThe 100 Most Cited Articles in Prosthodontic Journals: A Bibliometric Analysis of Articles Published Between 1951 and 2019Najeeb UllahNessuna valutazione finora
- Pakistan766 PDFDocumento3 paginePakistan766 PDFNajeeb UllahNessuna valutazione finora
- CPSP Sec 2020 4 27Documento1 paginaCPSP Sec 2020 4 27Najeeb UllahNessuna valutazione finora
- FCPS-II Online Exam Notification September 2020Documento2 pagineFCPS-II Online Exam Notification September 2020Najeeb UllahNessuna valutazione finora
- Interventions To Reduce Stigma Related To Mental Illnesses in Educational Institutes: A Systematic ReviewDocumento17 pagineInterventions To Reduce Stigma Related To Mental Illnesses in Educational Institutes: A Systematic ReviewNajeeb UllahNessuna valutazione finora
- Vincent Trapozzano, New Portrichey, Fla.,And Gordon Winter, PhiladelphiaDocumento7 pagineVincent Trapozzano, New Portrichey, Fla.,And Gordon Winter, PhiladelphiaNajeeb UllahNessuna valutazione finora
- Denture Stomatitis and DMDocumento6 pagineDenture Stomatitis and DMNajeeb UllahNessuna valutazione finora
- UntitledDocumento5 pagineUntitledBunga Erlita RosaliaNessuna valutazione finora
- Technology and Livelihood Education: Agri - Fishery Arts (Agricultural Crops Production) Marketing Agricultural ProductsDocumento14 pagineTechnology and Livelihood Education: Agri - Fishery Arts (Agricultural Crops Production) Marketing Agricultural Productslana del rey100% (1)
- 1136 E01-ML01DP5 Usermanual EN V1.2Documento11 pagine1136 E01-ML01DP5 Usermanual EN V1.2HectorNessuna valutazione finora
- Water Sampling and Borehole Inspection FormsDocumento2 pagineWater Sampling and Borehole Inspection FormsSibanda MqondisiNessuna valutazione finora
- DRM 25Documento14 pagineDRM 25Anantha RajanNessuna valutazione finora
- Cygnus 4plus Operating ManualDocumento141 pagineCygnus 4plus Operating Manualdzul effendiNessuna valutazione finora
- Plenaristas León 2022xDocumento6 paginePlenaristas León 2022xGloria MontielNessuna valutazione finora
- Chemistry 101 - The Complete Notes - Joliet Junior College (PDFDrive)Documento226 pagineChemistry 101 - The Complete Notes - Joliet Junior College (PDFDrive)Kabwela MwapeNessuna valutazione finora
- DAFTAR PUSTAKA Generik vs Branded Drug ReferencesDocumento4 pagineDAFTAR PUSTAKA Generik vs Branded Drug ReferencesRika MardiahNessuna valutazione finora
- Timeline of Internet in The PhilippinesDocumento29 pagineTimeline of Internet in The PhilippinesJhayson Joeshua Rubio100% (1)
- Lecture 6-Design For ShearDocumento14 pagineLecture 6-Design For ShearMarkos DanielNessuna valutazione finora
- Understanding Logistics and Supply Chain Management ConceptsDocumento12 pagineUnderstanding Logistics and Supply Chain Management Conceptsarfat kabraNessuna valutazione finora
- ADII11 Metode Deteksi OutlierDocumento50 pagineADII11 Metode Deteksi Outlier21-A-2-19 Nazli Amaliya RamadhaniNessuna valutazione finora
- 6 Main Rotor Config DesignDocumento44 pagine6 Main Rotor Config DesignDeepak Paul TirkeyNessuna valutazione finora
- REFLEKSI KASUS PLASENTADocumento48 pagineREFLEKSI KASUS PLASENTAImelda AritonangNessuna valutazione finora
- Board of Intermediate & Secondary Education, Lahore: Tahir Hussain JafriDocumento2 pagineBoard of Intermediate & Secondary Education, Lahore: Tahir Hussain Jafridr_azharhayatNessuna valutazione finora
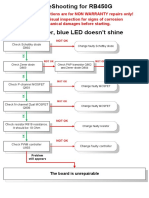
- RB450G Trouble ShootingDocumento9 pagineRB450G Trouble Shootingjocimar1000Nessuna valutazione finora
- Small Healthcare Organization: National Accreditation Board For Hospitals & Healthcare Providers (Nabh)Documento20 pagineSmall Healthcare Organization: National Accreditation Board For Hospitals & Healthcare Providers (Nabh)Dipti PatilNessuna valutazione finora
- Smell Detectives: An Olfactory History of Nineteenth-Century Urban AmericaDocumento35 pagineSmell Detectives: An Olfactory History of Nineteenth-Century Urban AmericaUniversity of Washington PressNessuna valutazione finora
- Information HandoutsDocumento6 pagineInformation HandoutsPooja Marwadkar TupcheNessuna valutazione finora
- Ivy DLP 2nd Quart CotDocumento4 pagineIvy DLP 2nd Quart CotJhim CaasiNessuna valutazione finora
- 199-Article Text-434-1-10-20200626Documento11 pagine199-Article Text-434-1-10-20200626ryan renaldiNessuna valutazione finora
- Mohammad Abu-Radi ResumeDocumento4 pagineMohammad Abu-Radi ResumeMohammad Abu-RadiNessuna valutazione finora
- Develop Network Monitoring System IP Subnet CalculatorDocumento23 pagineDevelop Network Monitoring System IP Subnet CalculatorabiramanNessuna valutazione finora
- CHB1 Assignmen5Documento2 pagineCHB1 Assignmen5anhspidermenNessuna valutazione finora
- MAPEH 6- WEEK 1 ActivitiesDocumento4 pagineMAPEH 6- WEEK 1 ActivitiesCatherine Renante100% (2)
- 16SEE - Schedule of PapersDocumento36 pagine16SEE - Schedule of PapersPiyush Jain0% (1)
- Teodorico M. Collano, JR.: ENRM 223 StudentDocumento5 pagineTeodorico M. Collano, JR.: ENRM 223 StudentJepoyCollanoNessuna valutazione finora
- Crafting and Executing StrategyDocumento33 pagineCrafting and Executing Strategyamoore2505Nessuna valutazione finora
- The Importance of WritingDocumento4 pagineThe Importance of WritingBogdan VasileNessuna valutazione finora
- Engine Controls (Powertrain Management) - ALLDATA RepairDocumento5 pagineEngine Controls (Powertrain Management) - ALLDATA RepairXavier AlvarezNessuna valutazione finora