Potrebbero piacerti anche
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (120)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (73)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- Disease Detectives NotesDocumento5 pagineDisease Detectives NotesErica Weng0% (1)
- Veterinary Epidemiology (VEP-411)Documento15 pagineVeterinary Epidemiology (VEP-411)Vijay Kumar Anumolu100% (1)
- Erc Cap PDFDocumento299 pagineErc Cap PDFSilvia Ramos YllescasNessuna valutazione finora
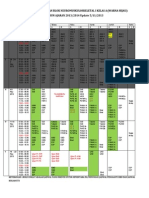
- Jadwal Stase Interna G29 RSMLDocumento7 pagineJadwal Stase Interna G29 RSMLLaura PutriNessuna valutazione finora
- Otitis MediaDocumento84 pagineOtitis MediaAlex MatthewNessuna valutazione finora
- Postdialysis Hypertension: Associated Factors, Patient Profiles, and Cardiovascular MortalityDocumento6 paginePostdialysis Hypertension: Associated Factors, Patient Profiles, and Cardiovascular MortalityLaura PutriNessuna valutazione finora
- Postdialysis Hypertension: Associated Factors, Patient Profiles, and Cardiovascular MortalityDocumento6 paginePostdialysis Hypertension: Associated Factors, Patient Profiles, and Cardiovascular MortalityLaura PutriNessuna valutazione finora
- Guidelines On Chronic Kidney Disease: (NKF K/Doqi)Documento32 pagineGuidelines On Chronic Kidney Disease: (NKF K/Doqi)Laura PutriNessuna valutazione finora
- Surviving Sepsis Hour 1 Bundle InfographDocumento1 paginaSurviving Sepsis Hour 1 Bundle InfographLaura PutriNessuna valutazione finora
- Protein Uri ADocumento12 pagineProtein Uri ALaura PutriNessuna valutazione finora
- Optical Prescription Details August 20XXDocumento3 pagineOptical Prescription Details August 20XXLaura PutriNessuna valutazione finora
- Portable CXR Neonate ScbuDocumento2 paginePortable CXR Neonate ScbuLaura PutriNessuna valutazione finora
- Tanda Khas KulitDocumento7 pagineTanda Khas KulitLaura PutriNessuna valutazione finora
- Morning Report Monday, 5 February 2018: Dept of Neurology G29Documento21 pagineMorning Report Monday, 5 February 2018: Dept of Neurology G29Laura PutriNessuna valutazione finora
- Jadwal Pembelajaran Blok Neuromuskuloskeletal I Kelas A (Warna Hijau) TAHUN AJARAN 2013/2014 Update 5/11/2013Documento3 pagineJadwal Pembelajaran Blok Neuromuskuloskeletal I Kelas A (Warna Hijau) TAHUN AJARAN 2013/2014 Update 5/11/2013Laura PutriNessuna valutazione finora
- Print FriendlyDocumento14 paginePrint FriendlyLaura PutriNessuna valutazione finora
- 2005 Lipid Lowering DrugsDocumento22 pagine2005 Lipid Lowering DrugsLaura PutriNessuna valutazione finora
- Catheter Problem Solving GuideDocumento19 pagineCatheter Problem Solving GuideLaura PutriNessuna valutazione finora
- Kerning and Brudzinski-MeningitaDocumento2 pagineKerning and Brudzinski-MeningitaDobre CristinaNessuna valutazione finora
- Penatalaksanaan: Amirah Muhammad ADocumento8 paginePenatalaksanaan: Amirah Muhammad ALaura PutriNessuna valutazione finora
- Colloidsdengue 11 1 C RDocumento21 pagineColloidsdengue 11 1 C RLaura PutriNessuna valutazione finora
- JNC8 HTNDocumento2 pagineJNC8 HTNTaradifaNurInsi0% (1)
- Jadwal Pembelajaran Blok Neuromuskuloskeletal I Kelas A (Warna Hijau) TAHUN AJARAN 2013/2014 Update 5/11/2013Documento3 pagineJadwal Pembelajaran Blok Neuromuskuloskeletal I Kelas A (Warna Hijau) TAHUN AJARAN 2013/2014 Update 5/11/2013Laura PutriNessuna valutazione finora
- MalariaDocumento2 pagineMalariaLaura PutriNessuna valutazione finora
- Jadwal Pembelajaran Blok Neuromuskuloskeletal I Kelas A (Warna Hijau) TAHUN AJARAN 2013/2014 Update 5/11/2013Documento3 pagineJadwal Pembelajaran Blok Neuromuskuloskeletal I Kelas A (Warna Hijau) TAHUN AJARAN 2013/2014 Update 5/11/2013Laura PutriNessuna valutazione finora
- Epididymitis LanjutanDocumento11 pagineEpididymitis LanjutanLaura PutriNessuna valutazione finora
- Unit-I. Epidemiology IntroductionDocumento60 pagineUnit-I. Epidemiology IntroductionAny OneNessuna valutazione finora
- CHN - Vital Statistics 1Documento5 pagineCHN - Vital Statistics 1CARL ANGEL JAOCHICONessuna valutazione finora
- Recording and Presenting Veterinary DataDocumento92 pagineRecording and Presenting Veterinary DataFerahadin Sultan100% (1)
- Take Test: Epidemiology Quiz E2Documento2 pagineTake Test: Epidemiology Quiz E2Viswa VittalNessuna valutazione finora
- Week 4 - Rates, Ratios and Vital StatisticsDocumento16 pagineWeek 4 - Rates, Ratios and Vital StatisticsAly D. De LeonNessuna valutazione finora
- 900 World Fact SheetsDocumento2 pagine900 World Fact SheetsNik rabekNessuna valutazione finora
- BMAT 2008 Section 1Documento28 pagineBMAT 2008 Section 1trueflaseNessuna valutazione finora
- Cohort StudyDocumento20 pagineCohort StudyUlfaNessuna valutazione finora
- EpidemiologyDocumento86 pagineEpidemiologyBirhaneNessuna valutazione finora
- Tutorial 1.1 - Measuring Disease Occurence (Mortality)Documento3 pagineTutorial 1.1 - Measuring Disease Occurence (Mortality)Fovilia Dewi100% (1)
- Alzheimer S Dementia - 2021 - Rahman - Rural Urban Differences in Diagnostic Incidence and Prevalence of Alzheimer SDocumento18 pagineAlzheimer S Dementia - 2021 - Rahman - Rural Urban Differences in Diagnostic Incidence and Prevalence of Alzheimer Sbcjbc7wxxpNessuna valutazione finora
- (Health Indicators) AND AN Overview of DemographyDocumento46 pagine(Health Indicators) AND AN Overview of DemographyquerokeropiNessuna valutazione finora
- Rol - Research DesignDocumento28 pagineRol - Research DesignLaish Christle CapiendoNessuna valutazione finora
- General EpidemiologyDocumento40 pagineGeneral EpidemiologyrajshreeNessuna valutazione finora
- Preventive and Social Medicine: Concept of Health and DiseaseDocumento7 paginePreventive and Social Medicine: Concept of Health and DiseaseskNessuna valutazione finora
- Epi-Chapter 2-3Documento66 pagineEpi-Chapter 2-3Wabela KedirNessuna valutazione finora
- HealthIndicators PPT Chn2 Jan2021Documento119 pagineHealthIndicators PPT Chn2 Jan2021VAL ASHLIE ACEBARNessuna valutazione finora
- Cancer Fact Sheets 15Documento6 pagineCancer Fact Sheets 15Tika IndraNessuna valutazione finora
- Cross Sectional StudiesDocumento8 pagineCross Sectional Studiesflsmvfr nelmamesNessuna valutazione finora
- Tools of Epidemiology by Hamza Rasool NoorkaDocumento8 pagineTools of Epidemiology by Hamza Rasool NoorkaHamza Rasool NoorkaNessuna valutazione finora
- Learning Material-Community Health Nursing ProcessDocumento52 pagineLearning Material-Community Health Nursing Processzebzeb STEMANessuna valutazione finora
- PIIS0002939422004317Documento6 paginePIIS0002939422004317Anca Florina GaceaNessuna valutazione finora
- BCBR HighyieldDocumento72 pagineBCBR HighyieldAdichapuram PHCNessuna valutazione finora
- Practice Questions 1 - YoungDocumento12 paginePractice Questions 1 - Youngejyoung928100% (1)
- M1 Introduction To EpidemiologyDocumento3 pagineM1 Introduction To EpidemiologyMc Philip Gabay DamoclesNessuna valutazione finora
- Measurement of Diseases - LmaDocumento35 pagineMeasurement of Diseases - LmaLim Wei EnNessuna valutazione finora
- Biostat Week 4: Mortality Rate/death RateDocumento3 pagineBiostat Week 4: Mortality Rate/death RateMicah JadeNessuna valutazione finora