Potrebbero piacerti anche
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (74)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- Water Supply Design ManualDocumento4 pagineWater Supply Design ManualAnguzu Olega BrevisNessuna valutazione finora
- Social Aspect TR4 Cidanau Dam Reg 1Documento7 pagineSocial Aspect TR4 Cidanau Dam Reg 1Dwi CahyoNessuna valutazione finora
- Kahramaa TariffDocumento1 paginaKahramaa Tariffwesleyjames007Nessuna valutazione finora
- Waterborne Sanitation Design Guide - SJ VV & M V Dijk PDFDocumento288 pagineWaterborne Sanitation Design Guide - SJ VV & M V Dijk PDFjarrydNessuna valutazione finora
- Chap4 Water Supply HandbookDocumento42 pagineChap4 Water Supply HandbooksimoniaNessuna valutazione finora
- Water Treatement System Fot BoreholeDocumento6 pagineWater Treatement System Fot BoreholeChijioke ObiNessuna valutazione finora
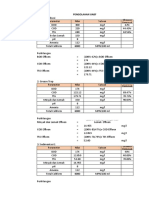
- Excel PerhitunganDocumento15 pagineExcel PerhitunganFirman MuhNessuna valutazione finora
- Pwsid: Metropolitan 2591: SystemDocumento4 paginePwsid: Metropolitan 2591: SystemMonica DiazNessuna valutazione finora
- Design Seminar - Plumbing PDFDocumento80 pagineDesign Seminar - Plumbing PDFJulan Castro100% (1)
- Bub 2014 & Regular 2014Documento82 pagineBub 2014 & Regular 2014Rohaina SapalNessuna valutazione finora
- Makalah (English)Documento6 pagineMakalah (English)Berlyan BesoniNessuna valutazione finora
- 20% 2012Documento172 pagine20% 2012jojazz74Nessuna valutazione finora
- MGT269 Group Project 1 (Group 2) - Proposal of Report)Documento4 pagineMGT269 Group Project 1 (Group 2) - Proposal of Report)Rules of Survival MALAYSIANessuna valutazione finora
- Malaysia Water SupplyDocumento7 pagineMalaysia Water SupplyAmir IejieNessuna valutazione finora
- ROCHEM Alemania Tratamiento Lixiviados de Rellenos Sanitarios Brochure Leachate-Leaflet-20-01-152Documento20 pagineROCHEM Alemania Tratamiento Lixiviados de Rellenos Sanitarios Brochure Leachate-Leaflet-20-01-152Manuel AlejandroNessuna valutazione finora
- Plumbing ResearchDocumento4 paginePlumbing ResearchJohn Renier AureadaNessuna valutazione finora
- Non-Renewable GW Management in SA by Ali Al-Tokhais-1Documento32 pagineNon-Renewable GW Management in SA by Ali Al-Tokhais-1Adly Al-SaafinNessuna valutazione finora
- Romanian Standard SR 1343 1ENG VERSIONDocumento29 pagineRomanian Standard SR 1343 1ENG VERSIONCristian SamsudeanNessuna valutazione finora
- Lecture 2 General Water Supply Design ConsiderationsDocumento9 pagineLecture 2 General Water Supply Design ConsiderationsSharif Gushgar0% (1)
- Draft Policy Recommendation On Domestic Was Tewater Management and Potential Project Prop Osal in Brunei DarussalamDocumento13 pagineDraft Policy Recommendation On Domestic Was Tewater Management and Potential Project Prop Osal in Brunei DarussalamHaqeem HNessuna valutazione finora
- KAP Customer Satisfaction Survey Questionnaire FinalDocumento7 pagineKAP Customer Satisfaction Survey Questionnaire FinalBongga Ka DayNessuna valutazione finora
- Filtration2014 EN WebDocumento6 pagineFiltration2014 EN WebNguyen AnNessuna valutazione finora
- CE405 Environmental Engineering - IDocumento2 pagineCE405 Environmental Engineering - IChithraNessuna valutazione finora
- En 8491 Water Supply EngineeringDocumento36 pagineEn 8491 Water Supply EngineeringsanthiamuthaNessuna valutazione finora
- PWA-RPD-CON-FM-1916 Completion and Taking Over Certificate Checklist R07Documento2 paginePWA-RPD-CON-FM-1916 Completion and Taking Over Certificate Checklist R07AbdelmonȜm MohNessuna valutazione finora
- INAE Project Report PDFDocumento211 pagineINAE Project Report PDFAkhilesh GuptaNessuna valutazione finora
- Sewerage Sanitation PlanDocumento18 pagineSewerage Sanitation PlanlengjavierNessuna valutazione finora
- Tool For Master Plan Formulation - Water Supply With Surface Water SourceDocumento25 pagineTool For Master Plan Formulation - Water Supply With Surface Water SourceaneeshmeloottuNessuna valutazione finora
- Accelerating The Provision of Safe Water Supply in Urban and Rural Areas of IndonesiaDocumento8 pagineAccelerating The Provision of Safe Water Supply in Urban and Rural Areas of IndonesiaOnggy Aries SekaNessuna valutazione finora
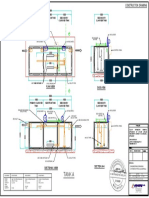
- Construction Drawing Example - Sepctic TankDocumento1 paginaConstruction Drawing Example - Sepctic TanknzhazmiNessuna valutazione finora