Potrebbero piacerti anche
- PUBH6001 Policy Analysis EssayDocumento8 paginePUBH6001 Policy Analysis EssayAna Maria100% (1)
- Gerry Stimson - A Tale of Two EpidemicsDocumento11 pagineGerry Stimson - A Tale of Two EpidemicsmatNessuna valutazione finora
- 16.1 Teens and TobDocumento4 pagine16.1 Teens and TobGabriel ParksNessuna valutazione finora
- IQOS Paper 2-21-2020FDocumento313 pagineIQOS Paper 2-21-2020Falexandra popescu100% (1)
- Ministry of Health & Family Welfare, Government of IndiaDocumento6 pagineMinistry of Health & Family Welfare, Government of IndiarichakumariamityNessuna valutazione finora
- Report On TobaccoDocumento3 pagineReport On TobaccoV SHARAVANI MBANessuna valutazione finora
- BAB 1 Tobacco: 中 文 français русский españolDocumento6 pagineBAB 1 Tobacco: 中 文 français русский españolJenita SariNessuna valutazione finora
- 31 05 08 Smoking ConsultationDocumento110 pagine31 05 08 Smoking ConsultationBotany KC Anne Sevilleja-BrionesNessuna valutazione finora
- Anne Buttigieg: Abutt01@um - Edu.mt Anne - Buttigieg@gov - MTDocumento30 pagineAnne Buttigieg: Abutt01@um - Edu.mt Anne - Buttigieg@gov - MTTONY GO AWAYNessuna valutazione finora
- Global Tobacco EpidemicDocumento5 pagineGlobal Tobacco Epidemicsai vaibhavNessuna valutazione finora
- Population Health IssueDocumento10 paginePopulation Health Issuemini abrahamNessuna valutazione finora
- FCTC Article 6: Price and Tax Measures To Reduce The Demand of TobaccoDocumento6 pagineFCTC Article 6: Price and Tax Measures To Reduce The Demand of TobaccoAnonymous KN8SDURsM3Nessuna valutazione finora
- Ways of Increasing Smoking SafetyDocumento11 pagineWays of Increasing Smoking SafetyAckson gondoNessuna valutazione finora
- Annotated-Hlth 201050 20research 20paperDocumento6 pagineAnnotated-Hlth 201050 20research 20paperapi-709406220Nessuna valutazione finora
- Tobacco: Key FactsDocumento5 pagineTobacco: Key FactsRobert StevenNessuna valutazione finora
- Policy Brief PresentationDocumento9 paginePolicy Brief PresentationNoora ShresthaNessuna valutazione finora
- SmokingDocumento8 pagineSmokingMonda Bw'OnchwatiNessuna valutazione finora
- Research Proposal-A GondoDocumento6 pagineResearch Proposal-A GondoAckson gondoNessuna valutazione finora
- Tobacco SmokingDocumento9 pagineTobacco SmokingfresheruNessuna valutazione finora
- Team 1 Report-SmokingDocumento8 pagineTeam 1 Report-SmokingVanshika KhemkaNessuna valutazione finora
- Tobacco Term PaperDocumento7 pagineTobacco Term Papercvqvxrwgf100% (1)
- CPH Script For ReportingDocumento3 pagineCPH Script For ReportingTrëSNessuna valutazione finora
- Global and Regional Patterns of Tobacco Smoking and Tobacco Control PoliciesDocumento14 pagineGlobal and Regional Patterns of Tobacco Smoking and Tobacco Control PoliciesrekoaaNessuna valutazione finora
- Smoking Cessation Program: Dr. Rasha Salama PHD Community Medicine Suez Canal University EgyptDocumento52 pagineSmoking Cessation Program: Dr. Rasha Salama PHD Community Medicine Suez Canal University EgyptTep TepNessuna valutazione finora
- SCOPH Statement On Graphic Health Warnings For Tobacco ProductsDocumento2 pagineSCOPH Statement On Graphic Health Warnings For Tobacco ProductsAMSA_PhilippinesNessuna valutazione finora
- The Use and Abuse of Tobacco: Concept 18Documento4 pagineThe Use and Abuse of Tobacco: Concept 18Trang NguyenNessuna valutazione finora
- Smoking Cessation Program: RationaleDocumento5 pagineSmoking Cessation Program: RationaleJovic PocoNessuna valutazione finora
- In The Name of God, The Compassionate, The MercifulDocumento3 pagineIn The Name of God, The Compassionate, The MercifulkalikNessuna valutazione finora
- Global Tobacco EpidemicDocumento100 pagineGlobal Tobacco EpidemicIndonesia TobaccoNessuna valutazione finora
- Tabaquismo en El Adolescente: Adolescents and SmokingDocumento3 pagineTabaquismo en El Adolescente: Adolescents and SmokingDanaysi SeguraNessuna valutazione finora
- Tobacco ImpactDocumento5 pagineTobacco Impactayush kumarNessuna valutazione finora
- Anti SmokingDocumento31 pagineAnti SmokingAsad KhanNessuna valutazione finora
- Tobacco Smoking PDFDocumento5 pagineTobacco Smoking PDFJohn Michael CastroNessuna valutazione finora
- Review of Related LiteratureDocumento8 pagineReview of Related LiteratureRamsax VillasorNessuna valutazione finora
- Who Cop9 Oct 2021 (Letter)Documento11 pagineWho Cop9 Oct 2021 (Letter)Brent StaffordNessuna valutazione finora
- Tobacco Reflection PaperDocumento4 pagineTobacco Reflection Paperapi-356164412Nessuna valutazione finora
- Tobacco Research Paper OutlineDocumento7 pagineTobacco Research Paper Outlinehumin1byjig2100% (1)
- RRL LatestDocumento21 pagineRRL LatestDino DizonNessuna valutazione finora
- Cedlas Finalreport enDocumento35 pagineCedlas Finalreport enJesse DanzigNessuna valutazione finora
- Tobacco Control and E-CigarettesDocumento152 pagineTobacco Control and E-CigarettesNational Press Foundation100% (1)
- Vaping Among Youth and Young ADocumento8 pagineVaping Among Youth and Young Amikeb92556Nessuna valutazione finora
- Who Serves As TheDocumento7 pagineWho Serves As TheAarOn ChaizNessuna valutazione finora
- 2016 SGR Full Report Non-508 PDFDocumento298 pagine2016 SGR Full Report Non-508 PDFkamalkumar15Nessuna valutazione finora
- Ecigarete Use Among Youth and Young AdultsDocumento298 pagineEcigarete Use Among Youth and Young AdultsAsd EfgNessuna valutazione finora
- Treatment of Tobacco Use and Dependence: The Role of The Dental ProfessionalDocumento17 pagineTreatment of Tobacco Use and Dependence: The Role of The Dental ProfessionalAinur 'iin' RahmahNessuna valutazione finora
- HLSC November 21Documento5 pagineHLSC November 21Michael TruongNessuna valutazione finora
- Presentation of Anne Jones OAM in Lead Up To World Cancer Day 2017Documento12 paginePresentation of Anne Jones OAM in Lead Up To World Cancer Day 2017bobbyramakantNessuna valutazione finora
- Tobacco Use ThesisDocumento7 pagineTobacco Use Thesisericawrightalbuquerque100% (2)
- TobaccoDocumento2 pagineTobaccoDolphins' FriendNessuna valutazione finora
- Assignment 01 Submitted To: Iftekhar Mahfuz Course Code: BUS360 Section: 06 Submitted By: Mushfiqur Rahman ID # 1830858Documento6 pagineAssignment 01 Submitted To: Iftekhar Mahfuz Course Code: BUS360 Section: 06 Submitted By: Mushfiqur Rahman ID # 1830858Mushfiq ShinNessuna valutazione finora
- Cigarette Should Be BannedDocumento1 paginaCigarette Should Be Banneddhale3280Nessuna valutazione finora
- Tobacco Control: Kuswandewi, Nita Arisanti, Dadi S Argadiredja Department of Public Health FmupDocumento58 pagineTobacco Control: Kuswandewi, Nita Arisanti, Dadi S Argadiredja Department of Public Health FmupJessicaOktavianusNessuna valutazione finora
- Document 3 1Documento7 pagineDocument 3 1LucyNessuna valutazione finora
- Essay SmokingDocumento1 paginaEssay Smokingstevani120Nessuna valutazione finora
- Cigarette MarketingDocumento2 pagineCigarette MarketingSaad MajeedNessuna valutazione finora
- A3 Cigarette SmokingDocumento3 pagineA3 Cigarette Smokinggeraldandrin719Nessuna valutazione finora
- Surgeon General Report PDFDocumento790 pagineSurgeon General Report PDFPotato wedgesNessuna valutazione finora
- Final Thesis Topic About Sin Tax LawDocumento11 pagineFinal Thesis Topic About Sin Tax LawRomnick JesalvaNessuna valutazione finora
- TocDocumento727 pagineTocdjizhiee100% (1)
- Regulating Electronic Nicotine Delivery Systems and Heated Tobacco Products - Submission - 2019Documento21 pagineRegulating Electronic Nicotine Delivery Systems and Heated Tobacco Products - Submission - 2019babbettemdNessuna valutazione finora
- Stop Smoking: Proven Steps And Strategies To Make You Quit Smoking For GoodDa EverandStop Smoking: Proven Steps And Strategies To Make You Quit Smoking For GoodValutazione: 4 su 5 stelle4/5 (1)
- ThailandDocumento1 paginaThailandIndonesia TobaccoNessuna valutazione finora
- Community Partnership ContactsDocumento8 pagineCommunity Partnership ContactsIndonesia TobaccoNessuna valutazione finora
- NCDs Report Summary - WHODocumento8 pagineNCDs Report Summary - WHOIndonesia Tobacco100% (1)
- LatviaDocumento1 paginaLatviaIndonesia TobaccoNessuna valutazione finora
- MalaysiaDocumento1 paginaMalaysiaIndonesia TobaccoNessuna valutazione finora
- PakistanDocumento1 paginaPakistanIndonesia TobaccoNessuna valutazione finora
- SingaporeDocumento1 paginaSingaporeIndonesia TobaccoNessuna valutazione finora
- Source: WHODocumento2 pagineSource: WHOIndonesia TobaccoNessuna valutazione finora
- MauritusDocumento1 paginaMauritusIndonesia TobaccoNessuna valutazione finora
- IndiaDocumento1 paginaIndiaIndonesia TobaccoNessuna valutazione finora
- CanadaDocumento2 pagineCanadaIndonesia TobaccoNessuna valutazione finora
- IranDocumento1 paginaIranIndonesia TobaccoNessuna valutazione finora
- JordanDocumento1 paginaJordanIndonesia TobaccoNessuna valutazione finora
- EgyptDocumento1 paginaEgyptIndonesia TobaccoNessuna valutazione finora
- Googling Collection-The Web Authors Collected The Pictures Through Google. All Pictures Belong To Their Respective OwnersDocumento16 pagineGoogling Collection-The Web Authors Collected The Pictures Through Google. All Pictures Belong To Their Respective OwnersIndonesia TobaccoNessuna valutazione finora
- AustraliaDocumento4 pagineAustraliaIndonesia TobaccoNessuna valutazione finora
- VenezuelaDocumento2 pagineVenezuelaIndonesia TobaccoNessuna valutazione finora
- BruneiDocumento1 paginaBruneiIndonesia TobaccoNessuna valutazione finora
- Tobacco Industry ContactsDocumento70 pagineTobacco Industry ContactsIndonesia Tobacco100% (3)
- BrazilDocumento2 pagineBrazilIndonesia TobaccoNessuna valutazione finora
- Tobacco Control in The EUDocumento4 pagineTobacco Control in The EUIndonesia TobaccoNessuna valutazione finora
- DjarumDocumento4 pagineDjarumIndonesia TobaccoNessuna valutazione finora
- The European Tobacco Control Report - 2007Documento160 pagineThe European Tobacco Control Report - 2007Indonesia TobaccoNessuna valutazione finora
- Anti Tobacco Organizations Outside USDocumento83 pagineAnti Tobacco Organizations Outside USIndonesia TobaccoNessuna valutazione finora
- Tobacco Control ContactsDocumento112 pagineTobacco Control ContactsIndonesia TobaccoNessuna valutazione finora
- The Morality of Marketing The Marlboro ManDocumento4 pagineThe Morality of Marketing The Marlboro ManAngie BuneaNessuna valutazione finora
- Bo LeadsDocumento35 pagineBo LeadsBob100% (1)
- Good Times USA LLC Announces The Acquisition of Historic Tobacco BrandsDocumento2 pagineGood Times USA LLC Announces The Acquisition of Historic Tobacco BrandsPR.comNessuna valutazione finora
- Good To Them at The Time, They Don't Realize How Much Harm Smoking Can Cause."Documento3 pagineGood To Them at The Time, They Don't Realize How Much Harm Smoking Can Cause."Sharmaine L. LozanoNessuna valutazione finora
- Ban Smoking Thesis StatementDocumento7 pagineBan Smoking Thesis Statementchristinaramirezaurora100% (2)
- Fact Sheet On COTPADocumento4 pagineFact Sheet On COTPArohitsantaniNessuna valutazione finora
- History: Tobacco Was First Cultivated by The Indians of North andDocumento30 pagineHistory: Tobacco Was First Cultivated by The Indians of North andShivansh SharmaNessuna valutazione finora
- Test of EinsteinDocumento3 pagineTest of Einsteinamen100% (4)
- How To Recoil A Vape CoilDocumento11 pagineHow To Recoil A Vape CoilAlldelectro musicNessuna valutazione finora
- Point-Of-Sale Marketing of Heated Tobacco Products in IsraelDocumento3 paginePoint-Of-Sale Marketing of Heated Tobacco Products in IsraelGina Marcela Chaves HenriquezNessuna valutazione finora
- Narrative Report On Tobacco Control and Anti-Smoking: San Roque Elementary SchoolDocumento4 pagineNarrative Report On Tobacco Control and Anti-Smoking: San Roque Elementary SchoolLoriefy Dela Cruz0% (1)
- Crew Effect DeclarationDocumento1 paginaCrew Effect DeclarationVILLANUEVA, Marvin L.Nessuna valutazione finora
- A Qualitative Study On BehaviorDocumento5 pagineA Qualitative Study On BehaviorRobby RanidoNessuna valutazione finora
- 03 DOH Red Orchid Awards (Batch 1)Documento46 pagine03 DOH Red Orchid Awards (Batch 1)VikangAdor100% (1)
- E Cigarettes and Vaping Infograph - v1 Nov 2021Documento1 paginaE Cigarettes and Vaping Infograph - v1 Nov 2021hermannNessuna valutazione finora
- Fullpapers Jahie6b5f4d1e3fullDocumento12 pagineFullpapers Jahie6b5f4d1e3fullrifka yoesoefNessuna valutazione finora
- PMFTC World-Class QualityDocumento26 paginePMFTC World-Class Qualityiamrobidomingo1989Nessuna valutazione finora
- POT Lesson PlanDocumento4 paginePOT Lesson PlanMichelle ThereseNessuna valutazione finora
- Alphabetical Brand List: CEDF0966Documento36 pagineAlphabetical Brand List: CEDF0966Someguy95Nessuna valutazione finora
- TARRANT COUNTY - Fort Worth ISD - 2004 Texas School Survey of Drug and Alcohol UseDocumento115 pagineTARRANT COUNTY - Fort Worth ISD - 2004 Texas School Survey of Drug and Alcohol UseTexas School Survey of Drug and Alcohol UseNessuna valutazione finora
- Pendientes Sin CumplirDocumento19 paginePendientes Sin CumplirPaula Sofia Castiblanco SiabatoNessuna valutazione finora
- NDoc 3483Documento4 pagineNDoc 3483Paola CvitanovićNessuna valutazione finora
- Should Smoking Cigarette Be BannedDocumento4 pagineShould Smoking Cigarette Be BannedHusna SallehNessuna valutazione finora
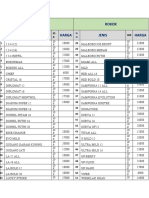
- Rokok Rokok Jenis Harga Jenis Harga: ID R IDRDocumento2 pagineRokok Rokok Jenis Harga Jenis Harga: ID R IDRAnanda putri sodiq mNessuna valutazione finora
- Persuasive EssayDocumento2 paginePersuasive EssayIkai CasisonNessuna valutazione finora
- Wills PPT For MBA Class Demo Strati OnDocumento26 pagineWills PPT For MBA Class Demo Strati Onknowsaurav1947Nessuna valutazione finora
- Oklahoma Fact SheetDocumento2 pagineOklahoma Fact Sheetnchc-scribdNessuna valutazione finora
- Why Do Cigarettes and Alcohol Considered Gateway DrugsDocumento33 pagineWhy Do Cigarettes and Alcohol Considered Gateway DrugsEricka Mae TizonNessuna valutazione finora