Potrebbero piacerti anche
- Experiment 4 Rat RespiratoryDocumento5 pagineExperiment 4 Rat RespiratoryMuhammad Safwan100% (3)
- Chest PhysiotherapyDocumento22 pagineChest Physiotherapyغيداء الذويبي100% (1)
- Procedure On Chest PhysiotherapyDocumento13 pagineProcedure On Chest PhysiotherapyDimpal ChoudharyNessuna valutazione finora
- Breathing RetrainingDocumento39 pagineBreathing RetrainingAishwarya PanchalNessuna valutazione finora
- Respiratory Care ModalitiesDocumento5 pagineRespiratory Care ModalitiesWendy EscalanteNessuna valutazione finora
- Textbook of Physiotherapy For Obstetric and Gynecological Conditions MASUD PDFDocumento205 pagineTextbook of Physiotherapy For Obstetric and Gynecological Conditions MASUD PDFAlina Gherman-Haiduc75% (4)
- Lecture Notes - BIOS1170B (Body Systems - (Structure and Function) ) (Sydney)Documento86 pagineLecture Notes - BIOS1170B (Body Systems - (Structure and Function) ) (Sydney)SK AuNessuna valutazione finora
- Section IIDocumento32 pagineSection IImm3370350Nessuna valutazione finora
- Chest PhysiotherapyDocumento4 pagineChest Physiotherapyhakky gamyNessuna valutazione finora
- Physio in CovidDocumento4 paginePhysio in CovidshankerahulNessuna valutazione finora
- Respiratory Care ProceduresDocumento5 pagineRespiratory Care Proceduresrubycorazon_edizaNessuna valutazione finora
- Chest Physiotherapy NewDocumento35 pagineChest Physiotherapy NewbobinkNessuna valutazione finora
- Deep Breathing ExerciseDocumento7 pagineDeep Breathing ExerciseRuchika Kaushal100% (5)
- Chest PhysiotherapyDocumento8 pagineChest PhysiotherapyPoova RagavanNessuna valutazione finora
- Pediatric Chest PhysiotherapyDocumento25 paginePediatric Chest PhysiotherapyShubha DiwakarNessuna valutazione finora
- Nusing Skills Output (Nso)Documento3 pagineNusing Skills Output (Nso)leroux2890Nessuna valutazione finora
- Chest Physiotherapy BPTDocumento20 pagineChest Physiotherapy BPTWraith GAMINGNessuna valutazione finora
- Lecture# 7 PR-Postural DraingaeDocumento57 pagineLecture# 7 PR-Postural DraingaeHafsa AzizNessuna valutazione finora
- Percussion 2. Vibration 3. ShakingDocumento2 paginePercussion 2. Vibration 3. ShakingMokibulNessuna valutazione finora
- Demo ChecklistDocumento4 pagineDemo ChecklistDanielle Audrey BanNessuna valutazione finora
- Chest PhysiotherapyDocumento7 pagineChest PhysiotherapyNikhil Mohan100% (1)
- Chest PhysiotherapyDocumento42 pagineChest PhysiotherapyLovelights ZamoraNessuna valutazione finora
- 4 5764879888385313380Documento30 pagine4 5764879888385313380Mohamed MahmoudNessuna valutazione finora
- 4.3 Respi. Percussion VibrationDocumento8 pagine4.3 Respi. Percussion VibrationRiza Angela BarazanNessuna valutazione finora
- Breathing ExerciseDocumento32 pagineBreathing ExerciseAdyasha SharmaNessuna valutazione finora
- Breathing ExerciseDocumento43 pagineBreathing ExerciseRahul YadavNessuna valutazione finora
- Pulmonary Assessment: Components of The AssessmentDocumento6 paginePulmonary Assessment: Components of The AssessmentWenzy Razzie cruzNessuna valutazione finora
- Midterm Last TopicDocumento3 pagineMidterm Last TopicLynette BalodNessuna valutazione finora
- Demonstration On Chest Physiotherapy DefinitionDocumento3 pagineDemonstration On Chest Physiotherapy Definitiondileep0% (1)
- Breathing ExercisesDocumento35 pagineBreathing ExercisesShubham KathareNessuna valutazione finora
- Breathing and Incentive SpirometryDocumento41 pagineBreathing and Incentive SpirometryVillain DevilNessuna valutazione finora
- Lung Exam DetailsDocumento3 pagineLung Exam Detailsdidutza91Nessuna valutazione finora
- Breathingexercise 180416095927Documento43 pagineBreathingexercise 180416095927Vidya UtamaNessuna valutazione finora
- Postural DrainageDocumento6 paginePostural DrainageKit Alizon Barredo0% (1)
- Ineffective Airway ClearanceDocumento10 pagineIneffective Airway ClearanceHannah VueltaNessuna valutazione finora
- Pulmonary Assessment: Components of The AssessmentDocumento7 paginePulmonary Assessment: Components of The Assessmentjoanna gurtizaNessuna valutazione finora
- Chest PhysiotherapyDocumento13 pagineChest PhysiotherapyAlma Susan100% (1)
- 5) Breathing TechniquesDocumento6 pagine5) Breathing TechniquesAiza RayanNessuna valutazione finora
- CPRDocumento4 pagineCPRBhosxz MoniqueNessuna valutazione finora
- Types of CPR: 1) High Frequency Chest Compression CPRDocumento3 pagineTypes of CPR: 1) High Frequency Chest Compression CPRYoussef ElkomatyNessuna valutazione finora
- Chest Physiotherapy ProcedureDocumento2 pagineChest Physiotherapy ProcedurePiyali SahaNessuna valutazione finora
- Orthopedic Manual Therapy Chadcook3rdPTMASUDDocumento30 pagineOrthopedic Manual Therapy Chadcook3rdPTMASUDHisham Al ShamiNessuna valutazione finora
- Chest PhysiotherapyDocumento2 pagineChest PhysiotherapyCarmela Dawn MarcoNessuna valutazione finora
- Breathing Exercises: Mazyad AlotaibiDocumento32 pagineBreathing Exercises: Mazyad AlotaibiekaNessuna valutazione finora
- Chest PhysiotherpypptDocumento32 pagineChest PhysiotherpypptVillain DevilNessuna valutazione finora
- Treatment Modalities 1. Chest PhysiotherapyDocumento9 pagineTreatment Modalities 1. Chest PhysiotherapyJayferson SalesNessuna valutazione finora
- PT Treatmet PostoperativelyDocumento16 paginePT Treatmet PostoperativelyMartha ChaseNessuna valutazione finora
- Chest PhysiotherapyDocumento22 pagineChest PhysiotherapyGhia_Angeles_8457Nessuna valutazione finora
- Funda Lab Mod 5-7Documento13 pagineFunda Lab Mod 5-7Liane BartolomeNessuna valutazione finora
- Breathing ExerDocumento28 pagineBreathing ExerNeeraja M SureshNessuna valutazione finora
- NSO Chest PhysiotherapyDocumento5 pagineNSO Chest PhysiotherapyAlih KathlyannNessuna valutazione finora
- Cardio Pulmonary ResuscitationDocumento15 pagineCardio Pulmonary ResuscitationmubeenibrahimjuniorNessuna valutazione finora
- 1st Year GNMDocumento33 pagine1st Year GNMarunimasahadevan98Nessuna valutazione finora
- Chest ExaminationDocumento5 pagineChest Examinationalin malekNessuna valutazione finora
- Lung Transplantation and Role of PhysiotherapyDocumento17 pagineLung Transplantation and Role of PhysiotherapySherry bhattiNessuna valutazione finora
- Bronchial Hygiene or Airway Clearance TechniquesDocumento139 pagineBronchial Hygiene or Airway Clearance TechniquesPiyush Salgaonkar100% (1)
- Deep Breathing, Coughing, and Moving After SurgeryDocumento4 pagineDeep Breathing, Coughing, and Moving After SurgeryNessa Layos MorilloNessuna valutazione finora
- CPR and Airway Mgt.Documento26 pagineCPR and Airway Mgt.Pierenne Virgil Suarez PinlacNessuna valutazione finora
- CHEST PHYSIOTHERAPY IN NEONATES NotesDocumento14 pagineCHEST PHYSIOTHERAPY IN NEONATES NotesAnu YadavNessuna valutazione finora
- Chest PhysiotherapyDocumento15 pagineChest PhysiotherapyreconredulaNessuna valutazione finora
- BHTDocumento18 pagineBHTNitesh KumawatNessuna valutazione finora
- Risk Factors For Pulmonary Disease: What Equipment, Drains or Lines Are Attached To The Patient Are They Obese?Documento3 pagineRisk Factors For Pulmonary Disease: What Equipment, Drains or Lines Are Attached To The Patient Are They Obese?Anonymous b4P7PDNessuna valutazione finora
- Amputation Rehabilitation: Guidance For The Education of Pre-Registration Physiotherapy StudentsDocumento30 pagineAmputation Rehabilitation: Guidance For The Education of Pre-Registration Physiotherapy StudentsAnonymous b4P7PDNessuna valutazione finora
- The Effect of Pre-Operative Exercises Education and Pain Control PDFDocumento26 pagineThe Effect of Pre-Operative Exercises Education and Pain Control PDFAnonymous b4P7PDNessuna valutazione finora
- The Effect of Pre-Operative Exercises Education and Pain Control PDFDocumento26 pagineThe Effect of Pre-Operative Exercises Education and Pain Control PDFAnonymous b4P7PDNessuna valutazione finora
- Urinary IncontinenceDocumento12 pagineUrinary IncontinenceAnonymous b4P7PDNessuna valutazione finora
- Petri DishDocumento7 paginePetri DishMizzannul HalimNessuna valutazione finora
- Perspectives: Down Syndrome and Genetics - A Case of Linked HistoriesDocumento11 paginePerspectives: Down Syndrome and Genetics - A Case of Linked Historiespeterr1022Nessuna valutazione finora
- Matilde-Tomaselli Cv-ShortDocumento4 pagineMatilde-Tomaselli Cv-Shortapi-308749490Nessuna valutazione finora
- Charnley Ankle ArthrodesisDocumento12 pagineCharnley Ankle Arthrodesisdr_s_ganeshNessuna valutazione finora
- Articulo 3Documento5 pagineArticulo 3Valeria Rodriguez GomezNessuna valutazione finora
- Blood DopingDocumento16 pagineBlood Dopingpriyanka lalwaniNessuna valutazione finora
- ENGLISH GRAMMER For STD 6Documento21 pagineENGLISH GRAMMER For STD 6Joy OtanielNessuna valutazione finora
- Cestode Parasites: Medical Parasitology, 2009 University of Palangkaraya Agus HaryonoDocumento45 pagineCestode Parasites: Medical Parasitology, 2009 University of Palangkaraya Agus HaryonoMeylisa Gerson BayanNessuna valutazione finora
- Treatment of CellulitisDocumento2 pagineTreatment of CellulitistreatmentcellNessuna valutazione finora
- CDCDocumento168 pagineCDCKing4Real100% (1)
- CLIA Acceptable Test Performance CriteriaDocumento4 pagineCLIA Acceptable Test Performance CriteriaMihaelaHorgaNessuna valutazione finora
- Roughdraft EditedDocumento7 pagineRoughdraft Editedapi-356188860Nessuna valutazione finora
- Child Immunization Record: Age in Months Nutrional StatusDocumento14 pagineChild Immunization Record: Age in Months Nutrional StatusMa. Jesica Salve LasundinNessuna valutazione finora
- CBSE Class 7 English - Comprehension PassageDocumento7 pagineCBSE Class 7 English - Comprehension PassagemotherhoodNessuna valutazione finora
- Annatomy Notes For Bpe StudDocumento14 pagineAnnatomy Notes For Bpe StudYoga KalyanamNessuna valutazione finora
- About Us: Vaccination AND Deworming ProgramDocumento1 paginaAbout Us: Vaccination AND Deworming ProgramTolitzjr CatayloNessuna valutazione finora
- Jaundice Natural RemediesDocumento12 pagineJaundice Natural RemediesprkshshrNessuna valutazione finora
- Asphyxia 2Documento55 pagineAsphyxia 2api-19916399100% (1)
- Vocabulary Exercises: 1) Complete in The Correct WayDocumento5 pagineVocabulary Exercises: 1) Complete in The Correct Waylaura1pinilla1domingNessuna valutazione finora
- ECCO 2 Hemodynamics TestDocumento3 pagineECCO 2 Hemodynamics TestpamoralesNessuna valutazione finora
- Reminiscences of An Old TimerDocumento524 pagineReminiscences of An Old TimersuneelmadhavNessuna valutazione finora
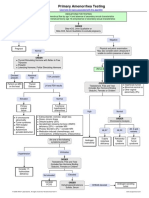
- Primary Amenorrhea Testing AlgorithmDocumento1 paginaPrimary Amenorrhea Testing AlgorithmGabriella AguirreNessuna valutazione finora
- Urinary IncontinenceDocumento334 pagineUrinary Incontinencealex100% (2)
- Variability and Accuracy of Sahlis Method InEstimation of Haemoglobin ConcentrationDocumento8 pagineVariability and Accuracy of Sahlis Method InEstimation of Haemoglobin Concentrationastrii 08Nessuna valutazione finora
- AyurvedicDocumento8 pagineAyurvedicVijay VishwakarmaNessuna valutazione finora
- Microbiology Mnemonics: Study Online atDocumento3 pagineMicrobiology Mnemonics: Study Online atKriselda May Torio100% (1)
- BSCI 4001 Transcript MidtermDocumento4 pagineBSCI 4001 Transcript MidtermLynell Caraang BarayugaNessuna valutazione finora