Potrebbero piacerti anche
- Wjps 4 029Documento7 pagineWjps 4 029santy27Nessuna valutazione finora
- Ioi 140137Documento9 pagineIoi 140137santy27Nessuna valutazione finora
- WJCP 1 29 PDFDocumento5 pagineWJCP 1 29 PDFsanty27Nessuna valutazione finora
- Drury2013 PDFDocumento9 pagineDrury2013 PDFsanty27Nessuna valutazione finora
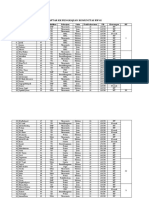
- Daftar KK Pengkajian Komunitas RW 02: Lampiran 6Documento4 pagineDaftar KK Pengkajian Komunitas RW 02: Lampiran 6santy27Nessuna valutazione finora
- International Journal of Nursing Studies: M Isabel Rı Os-Risquez, Mariano Garcı A-IzquierdoDocumento8 pagineInternational Journal of Nursing Studies: M Isabel Rı Os-Risquez, Mariano Garcı A-Izquierdosanty27Nessuna valutazione finora
- 10 1111@jog 12345Documento7 pagine10 1111@jog 12345santy27Nessuna valutazione finora
- Mortality Reduction For Fever, Hyperglycemia, and Swallowing Nurse-Initiated Stroke InterventionDocumento7 pagineMortality Reduction For Fever, Hyperglycemia, and Swallowing Nurse-Initiated Stroke Interventionsanty27Nessuna valutazione finora
- SEPSIS KASUSDocumento9 pagineSEPSIS KASUSDilessandro PieroNessuna valutazione finora
- Internet Video Chat Skype Family Conversations As A Treatment of Agitation in Nursing Home Residents With DementiaDocumento2 pagineInternet Video Chat Skype Family Conversations As A Treatment of Agitation in Nursing Home Residents With Dementiasanty27Nessuna valutazione finora
- Secret MessageDocumento2 pagineSecret Messagesanty27Nessuna valutazione finora
- DiscoveryDocumento1 paginaDiscoverysanty27Nessuna valutazione finora
- S110 FullDocumento10 pagineS110 Fullsanty27Nessuna valutazione finora
- Innovative Collaborations Summary FINALDocumento16 pagineInnovative Collaborations Summary FINALsanty27Nessuna valutazione finora
- Bits and Pieces in A TEYL Classroom - USD 2010Documento24 pagineBits and Pieces in A TEYL Classroom - USD 2010santy27Nessuna valutazione finora
- Bingo There Was A Farmer Had A Dog and Bingo Was His Name-O B-I-N-G-O, B-I-N-G-O, B-I-N-G-O and Bingo Was His Name-ODocumento1 paginaBingo There Was A Farmer Had A Dog and Bingo Was His Name-O B-I-N-G-O, B-I-N-G-O, B-I-N-G-O and Bingo Was His Name-Osanty27Nessuna valutazione finora
- Community Nursing Diagnosis and PrioritizingDocumento12 pagineCommunity Nursing Diagnosis and Prioritizingsanty27Nessuna valutazione finora
- Perkembangan AnakDocumento9 paginePerkembangan Anaksanty27Nessuna valutazione finora
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5783)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (587)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (72)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (265)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (119)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- Cotton-Top Tamarin - Husbandry - ManualDocumento98 pagineCotton-Top Tamarin - Husbandry - Manualjoaquin chan100% (1)
- EHV AC Transmission System Design and AnalysisDocumento104 pagineEHV AC Transmission System Design and Analysispraveenmande100% (1)
- NLE 08 Test IDocumento7 pagineNLE 08 Test IBrenlei Alexis NazarroNessuna valutazione finora
- Mamzelle Aurélie's RegretDocumento3 pagineMamzelle Aurélie's RegretDarell AgustinNessuna valutazione finora
- Task ManagerDocumento2 pagineTask Managersudharan271Nessuna valutazione finora
- Finding Buyers Leather Footwear - Italy2Documento5 pagineFinding Buyers Leather Footwear - Italy2Rohit KhareNessuna valutazione finora
- A Complete Guide To Amazon For VendorsDocumento43 pagineA Complete Guide To Amazon For Vendorsnissay99Nessuna valutazione finora
- Indonesian Hotel Annual ReviewDocumento34 pagineIndonesian Hotel Annual ReviewSPHM HospitalityNessuna valutazione finora
- The German Tradition of Psychology in Literature and Thought 1700-1840 PDFDocumento316 pagineThe German Tradition of Psychology in Literature and Thought 1700-1840 PDFerhan savasNessuna valutazione finora
- Underground Cable FaultDocumento8 pagineUnderground Cable FaultMohammad IrfanNessuna valutazione finora
- Monroes Motivated Sequence LessonDocumento3 pagineMonroes Motivated Sequence Lessonapi-257123630Nessuna valutazione finora
- Writing Patterns NotesDocumento2 pagineWriting Patterns NoteslwitsfadontNessuna valutazione finora
- Green Schools Project LAC PlanDocumento2 pagineGreen Schools Project LAC PlanJolly Mar Tabbaban Mangilaya100% (1)
- Replit Ubuntu 20 EnablerDocumento4 pagineReplit Ubuntu 20 EnablerDurval Junior75% (4)
- SQL QuestionsDocumento297 pagineSQL Questionskeysp75% (4)
- Reflection Paper About Educational Administration (Ivy M. Peralta)Documento1 paginaReflection Paper About Educational Administration (Ivy M. Peralta)Ivy peraltaNessuna valutazione finora
- CCTV Effectiveness in Reducing CrimeDocumento31 pagineCCTV Effectiveness in Reducing CrimeNeil Adonis UsaragaNessuna valutazione finora
- Rio 20 Conference SummaryDocumento3 pagineRio 20 Conference SummaryAyush BishtNessuna valutazione finora
- 9th Science Term 3 Model Question Paper English MediumDocumento3 pagine9th Science Term 3 Model Question Paper English MediumStalin JesudossNessuna valutazione finora
- Guidance On The Design Assessment and Strengthening of Masonry Parapets On Highway StructuresDocumento93 pagineGuidance On The Design Assessment and Strengthening of Masonry Parapets On Highway Structuresalan_jalil9365Nessuna valutazione finora
- Parallel Merge Sort With MPIDocumento12 pagineParallel Merge Sort With MPIIrsa kanwallNessuna valutazione finora
- Effects of strategic changes on operations budgets and performanceDocumento3 pagineEffects of strategic changes on operations budgets and performanceluiduro100% (1)
- Learning Team Aet562 - Self-Guided Social Media Training ManualDocumento18 pagineLearning Team Aet562 - Self-Guided Social Media Training Manualapi-646128900Nessuna valutazione finora
- Principles of Clinical Chemistry Automation and Point-of-Care TestingDocumento27 paginePrinciples of Clinical Chemistry Automation and Point-of-Care TestingMalliga SundareshanNessuna valutazione finora
- Math 20-2 Unit Plan (Statistics)Documento4 pagineMath 20-2 Unit Plan (Statistics)api-290174387Nessuna valutazione finora
- A1 Paper4 TangDocumento22 pagineA1 Paper4 Tangkelly2999123Nessuna valutazione finora
- Event Driven Dynamic Systems: Bujor PăvăloiuDocumento35 pagineEvent Driven Dynamic Systems: Bujor Păvăloiuezeasor arinzeNessuna valutazione finora
- Archana PriyadarshiniDocumento7 pagineArchana PriyadarshiniJagriti KumariNessuna valutazione finora
- Magnesium Alloy Anodes For Cathodic ProtectionDocumento2 pagineMagnesium Alloy Anodes For Cathodic Protectiongautam100% (1)
- Enclosure No. 6.7: Parental ConsentDocumento3 pagineEnclosure No. 6.7: Parental ConsentRhea CarinoNessuna valutazione finora