Potrebbero piacerti anche
- Crimson Druid v1.1Documento3 pagineCrimson Druid v1.1Carter RobinsonNessuna valutazione finora
- NCP Abruptio PlacentaDocumento2 pagineNCP Abruptio PlacentaCarson Birth100% (1)
- NCP Alterations in Normal LaborDocumento9 pagineNCP Alterations in Normal LaborCameron De GuzmanNessuna valutazione finora
- NCP - PreeclampsiaDocumento3 pagineNCP - PreeclampsiaRap De la Cruz50% (2)
- Abruptio Placenta NCP 2 FinalDocumento19 pagineAbruptio Placenta NCP 2 FinalTin100% (1)
- Raddaily Ankle MRI ApproachDocumento10 pagineRaddaily Ankle MRI ApproachSandeep VodelaNessuna valutazione finora
- Abruptio Placenta NCPDocumento2 pagineAbruptio Placenta NCPNichole Audrey Saavedra100% (1)
- NCP Post PartumDocumento2 pagineNCP Post PartumsteffiNessuna valutazione finora
- Total LaryngectomyDocumento15 pagineTotal LaryngectomyKumaran Bagavathi RagavanNessuna valutazione finora
- Science 8 Q4M1 Digestive System 2021 2022Documento5 pagineScience 8 Q4M1 Digestive System 2021 2022carl helloNessuna valutazione finora
- Presentation For Gender and Society 2Documento24 paginePresentation For Gender and Society 2Fhebelyn TaborNessuna valutazione finora
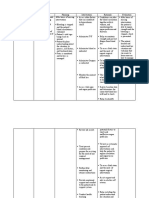
- Assessment Diagnosis Interference Planning Intervention Rationale EvaluationDocumento2 pagineAssessment Diagnosis Interference Planning Intervention Rationale EvaluationMelDred Cajes BolandoNessuna valutazione finora
- Care Plan PostpartumDocumento2 pagineCare Plan PostpartumSiwei Yang100% (1)
- Nursing Care Plans (NCP) of Abruptio PlacentaDocumento13 pagineNursing Care Plans (NCP) of Abruptio PlacentaKath76% (21)
- NCP Intra PartumDocumento4 pagineNCP Intra PartumElla Dayanghirang100% (1)
- Placenta Previa (NCP)Documento2 paginePlacenta Previa (NCP)jonna casumpangNessuna valutazione finora
- NCP: Prenatal InfectionDocumento10 pagineNCP: Prenatal InfectionJavieNessuna valutazione finora
- Altered Uteroplacental Tissue PerfusionDocumento5 pagineAltered Uteroplacental Tissue PerfusionArielle BajalaNessuna valutazione finora
- Brief Readings SWEDENBORG's PSYCHOLOGY Howard Davis Spoerl Swedenborg Foundation 1937Documento16 pagineBrief Readings SWEDENBORG's PSYCHOLOGY Howard Davis Spoerl Swedenborg Foundation 1937francis batt100% (1)
- Uterine AtonyDocumento3 pagineUterine AtonyArsheina Paradji100% (1)
- Neo Sepsis NCPDocumento15 pagineNeo Sepsis NCPmelodia gandezaNessuna valutazione finora
- PHIL-IRI-ENGLISH Screening TestDocumento4 paginePHIL-IRI-ENGLISH Screening Testjmar almazanNessuna valutazione finora
- Nursing Care Plan For Pregnancy Induced HypertensionDocumento9 pagineNursing Care Plan For Pregnancy Induced HypertensionMurugham DineshNessuna valutazione finora
- NCP On Postpartum MotherDocumento9 pagineNCP On Postpartum MotherM.S.H Tube100% (1)
- N E E D S C O G N I T I V E P E R P E T U A L RationaleDocumento14 pagineN E E D S C O G N I T I V E P E R P E T U A L RationaleArianna Jasmine MabungaNessuna valutazione finora
- New Born NCPDocumento8 pagineNew Born NCPCarl Vincent Marrion Rejuso100% (1)
- Educational Assistance LetterDocumento1 paginaEducational Assistance LetterTin100% (3)
- NCP For EclampsiaDocumento6 pagineNCP For EclampsiaXtine Soliman Zamora100% (3)
- All NCPsDocumento83 pagineAll NCPsDennis Nyambane Momanyi100% (6)
- (Letter of Invitation - Guest Speaker) - Usar (Do Not Include, Description Only) (Insert Sic Logo/ School Name)Documento2 pagine(Letter of Invitation - Guest Speaker) - Usar (Do Not Include, Description Only) (Insert Sic Logo/ School Name)Tin100% (1)
- Abruptio NCPDocumento4 pagineAbruptio NCPShien Samalea Vasquez100% (1)
- NCP (Acute Pain, Episiotomy)Documento6 pagineNCP (Acute Pain, Episiotomy)Jenny AjocNessuna valutazione finora
- Nursing Diagnosis: May Be Related To: Fluid Volume Deficit (Isotonic)Documento26 pagineNursing Diagnosis: May Be Related To: Fluid Volume Deficit (Isotonic)Ric Nacional75% (4)
- BOX 17.4 NCP Postpartum HemorrhageDocumento4 pagineBOX 17.4 NCP Postpartum HemorrhageJam AliNessuna valutazione finora
- Care Plan PostpartumDocumento2 pagineCare Plan Postpartumteokie082483% (6)
- Subjective: Short Term Goal: Independent: Short Term EvaluationDocumento2 pagineSubjective: Short Term Goal: Independent: Short Term EvaluationKyla Castro100% (1)
- Ncma219 Course Task 4Documento3 pagineNcma219 Course Task 4NikoruNessuna valutazione finora
- Threatened Abortion - Edited 1Documento55 pagineThreatened Abortion - Edited 1اكينو ستيفاني100% (1)
- NCP For Delivery RoomDocumento4 pagineNCP For Delivery RoomGiselle EstoquiaNessuna valutazione finora
- Hemorrhage NCPDocumento4 pagineHemorrhage NCPElishaNessuna valutazione finora
- Bielenda Professional Catalogue enDocumento88 pagineBielenda Professional Catalogue enBielendaProfessionalNessuna valutazione finora
- After 8 Hours of Nursing Interventions Patient Will Be Able To: Demonstrate Adequate Perfusion. Demonstrate Stable Vital SignsDocumento3 pagineAfter 8 Hours of Nursing Interventions Patient Will Be Able To: Demonstrate Adequate Perfusion. Demonstrate Stable Vital Signsroma_elonaNessuna valutazione finora
- NCP PPHDocumento2 pagineNCP PPHmikee-berredo-9975Nessuna valutazione finora
- Gi-Rle - NCP For Deficient Fluid VolumeDocumento2 pagineGi-Rle - NCP For Deficient Fluid VolumeEvangeline Villa de Gracia100% (1)
- Nursing Care PlanDocumento3 pagineNursing Care PlanArvan James Cabugayan TalboNessuna valutazione finora
- Precipitous Labor/Delivery or Unplanned/Out-of-Hospital DeliveryDocumento7 paginePrecipitous Labor/Delivery or Unplanned/Out-of-Hospital DeliveryLei Ortega100% (1)
- Hernandez NCP Drug StudyDocumento7 pagineHernandez NCP Drug StudyEliza Joyce HernandezNessuna valutazione finora
- Post-Partum Care Plan NCPDocumento2 paginePost-Partum Care Plan NCPRap De la CruzNessuna valutazione finora
- NCP - Diabetes Mellitus Prepregnancy/GestationalDocumento13 pagineNCP - Diabetes Mellitus Prepregnancy/GestationalClaudine Christophe100% (1)
- NCP Placenta PreviaDocumento2 pagineNCP Placenta PreviaCathy CnlsNessuna valutazione finora
- MR Right - Case Study Test - Summer 2018Documento7 pagineMR Right - Case Study Test - Summer 2018jadenNessuna valutazione finora
- NCP ObDocumento2 pagineNCP ObtimmyNessuna valutazione finora
- Nursing Care Plan For Knowledge DeficitDocumento3 pagineNursing Care Plan For Knowledge DeficitRegine BautistaNessuna valutazione finora
- Preterm Labor Prevention of DeliveryDocumento10 paginePreterm Labor Prevention of Deliverynursereview100% (1)
- NCP Example Pre EclampsiaDocumento6 pagineNCP Example Pre EclampsiaChristian Joseph OpianaNessuna valutazione finora
- Predisposing Factors:: Placenta Previa Lower Uterine SegmentDocumento11 paginePredisposing Factors:: Placenta Previa Lower Uterine Segmentjhachers100% (1)
- Abruptio Placenta Mini Case StudyDocumento20 pagineAbruptio Placenta Mini Case StudyAira AlaroNessuna valutazione finora
- NCP - BreastfeedingDocumento1 paginaNCP - Breastfeedingheather tbwn100% (1)
- Labor Nursing Care Plan 1Documento4 pagineLabor Nursing Care Plan 1Anna Mae DollenteNessuna valutazione finora
- NCP - PCGHDocumento9 pagineNCP - PCGHLucelle ArellanoNessuna valutazione finora
- NCP Case 1Documento6 pagineNCP Case 1boomer SeargeNessuna valutazione finora
- Nursing Care Plan For Postpartum HemorrhageDocumento2 pagineNursing Care Plan For Postpartum HemorrhageDianne Mae100% (1)
- Pre EclampsiaDocumento3 paginePre EclampsiaJon Sayson100% (1)
- Nursing Care Plan Abruptio PlacentaeDocumento2 pagineNursing Care Plan Abruptio PlacentaeWann WannNessuna valutazione finora
- Actual Impairment of Skin Integrity in The Perineum Related To Episiotomy Wound Secondary To Normal Birth DeliveryDocumento2 pagineActual Impairment of Skin Integrity in The Perineum Related To Episiotomy Wound Secondary To Normal Birth DeliveryNathalieCaracaNessuna valutazione finora
- Ineffective Tissue PerfusionDocumento2 pagineIneffective Tissue PerfusionMary Hope BacutaNessuna valutazione finora
- Deficient Fluid Volume (Isotonic) : Anxiety FearDocumento2 pagineDeficient Fluid Volume (Isotonic) : Anxiety FearVincent Paul SantosNessuna valutazione finora
- Prenatal Hemorrhage: Client Assessment Data Base: General Findings CirculationDocumento11 paginePrenatal Hemorrhage: Client Assessment Data Base: General Findings CirculationLei OrtegaNessuna valutazione finora
- CASE STUDY PPT Group1 - Revised WithoutvideoDocumento34 pagineCASE STUDY PPT Group1 - Revised WithoutvideoSamantha BolanteNessuna valutazione finora
- Abortion, Spontaneous Abortion, Miscarriage Nursing Care PlanDocumento3 pagineAbortion, Spontaneous Abortion, Miscarriage Nursing Care PlanPotato BananaNessuna valutazione finora
- AssignmentDocumento6 pagineAssignmentTinNessuna valutazione finora
- Font 6Documento1 paginaFont 6TinNessuna valutazione finora
- Gospel in BriefDocumento10 pagineGospel in BriefTinNessuna valutazione finora
- Irrigation Engineering JournalDocumento5 pagineIrrigation Engineering JournalTinNessuna valutazione finora
- New Testament Contradictions (1995) : Paul CarlsonDocumento20 pagineNew Testament Contradictions (1995) : Paul CarlsonTinNessuna valutazione finora
- RespiDocumento18 pagineRespiChristine Joy CamachoNessuna valutazione finora
- EporeDocumento1 paginaEporeTinNessuna valutazione finora
- San Isidro College City of MalaybalayDocumento1 paginaSan Isidro College City of MalaybalayTinNessuna valutazione finora
- CHNDocumento3 pagineCHNTinNessuna valutazione finora
- PubertyDocumento1 paginaPubertyTinNessuna valutazione finora
- Thousand One Hundred Sixty Two Pesos & 19/100 (P 1,688,162.19) Only FDocumento1 paginaThousand One Hundred Sixty Two Pesos & 19/100 (P 1,688,162.19) Only FTinNessuna valutazione finora
- CHN InitialDocumento1 paginaCHN InitialTinNessuna valutazione finora
- Respi Nclex AnswersDocumento3 pagineRespi Nclex AnswersTinNessuna valutazione finora
- AnilaDocumento1 paginaAnilaTinNessuna valutazione finora
- Theo ADocumento3 pagineTheo ATinNessuna valutazione finora
- 220 Nursing Bullets Pediatric Nursing ReviewerDocumento2 pagine220 Nursing Bullets Pediatric Nursing ReviewerTinNessuna valutazione finora
- DocxDocumento15 pagineDocxTinNessuna valutazione finora
- Thousand One Hundred Sixty Two Pesos & 19/100 (P 1,688,162.19) Only FDocumento1 paginaThousand One Hundred Sixty Two Pesos & 19/100 (P 1,688,162.19) Only FTinNessuna valutazione finora
- Thousand One Hundred Sixty Two Pesos & 19/100 (P 1,688,162.19) Only FDocumento1 paginaThousand One Hundred Sixty Two Pesos & 19/100 (P 1,688,162.19) Only FTinNessuna valutazione finora
- Pre Eclampsia 1Documento3 paginePre Eclampsia 1TinNessuna valutazione finora
- Contin TDocumento3 pagineContin TTinNessuna valutazione finora
- Thousand One Hundred Sixty Two Pesos & 19/100 (P 1,688,162.19) Only FDocumento1 paginaThousand One Hundred Sixty Two Pesos & 19/100 (P 1,688,162.19) Only FTinNessuna valutazione finora
- Thousand One Hundred Sixty Two Pesos & 19/100 (P 1,688,162.19) Only FDocumento1 paginaThousand One Hundred Sixty Two Pesos & 19/100 (P 1,688,162.19) Only FTinNessuna valutazione finora
- Thousand One Hundred Sixty Two Pesos & 19/100 (P 1,688,162.19) Only FDocumento1 paginaThousand One Hundred Sixty Two Pesos & 19/100 (P 1,688,162.19) Only FTinNessuna valutazione finora
- Eighty Eight Thousand One Hundred Sixty Two Pesos & 19/100 (P 1,688,162.19) Only FDocumento1 paginaEighty Eight Thousand One Hundred Sixty Two Pesos & 19/100 (P 1,688,162.19) Only FTinNessuna valutazione finora
- Eight Thousand One Hundred Sixty Two Pesos & 19/100 (P 1,688,162.19) Only FDocumento1 paginaEight Thousand One Hundred Sixty Two Pesos & 19/100 (P 1,688,162.19) Only FTinNessuna valutazione finora
- تقرير ثرموداينمكDocumento5 pagineتقرير ثرموداينمكاحمد كاظمNessuna valutazione finora
- Rula SheetDocumento2 pagineRula SheetCarl Christian CabelloNessuna valutazione finora
- Nano DentistryDocumento6 pagineNano DentistryanugrasNessuna valutazione finora
- Human Anatomy 4th Edition McKinley Test Bank 1Documento35 pagineHuman Anatomy 4th Edition McKinley Test Bank 1donnawugnwsjrzcxt100% (27)
- 70037Documento4 pagine70037Nabila SaribanunNessuna valutazione finora
- MPSFPRG Unit3Documento14 pagineMPSFPRG Unit3Haruna Gibril BenduNessuna valutazione finora
- Irregular PluralsDocumento19 pagineIrregular PluralsDj-mauro Mulchen ChileNessuna valutazione finora
- Renal Physiology PDFDocumento12 pagineRenal Physiology PDFLolitaNessuna valutazione finora
- MCQ Physical EducationDocumento43 pagineMCQ Physical EducationDr Tilak Raj MeenaNessuna valutazione finora
- Zoology II (Em) BLM 21-22Documento99 pagineZoology II (Em) BLM 21-22GANESH KANDAGATLANessuna valutazione finora
- Binary FissionDocumento4 pagineBinary FissionVINDHYA SHANKERNessuna valutazione finora
- Class XI Practicals Term2Documento5 pagineClass XI Practicals Term2Prince KNessuna valutazione finora
- Data Alkes 2020 TerbaruDocumento23 pagineData Alkes 2020 TerbaruRoyliNessuna valutazione finora
- Antibiotic and Its ResistanceDocumento19 pagineAntibiotic and Its ResistanceSuryaAtmajayaNessuna valutazione finora
- Answer Key P2Documento5 pagineAnswer Key P2Marie Stephan De Gracia TanNessuna valutazione finora
- Week 6 Facilitator Copy Week 06 Renal Failure PDFDocumento7 pagineWeek 6 Facilitator Copy Week 06 Renal Failure PDFoxyc0n999Nessuna valutazione finora
- AnatomyDocumento8 pagineAnatomyRobbie WoelkersNessuna valutazione finora
- The Effect of Nacl 0.9% and Nacl 0.45% On Sodium, Chloride, and Acid - Base Balance in A Picu PopulationDocumento7 pagineThe Effect of Nacl 0.9% and Nacl 0.45% On Sodium, Chloride, and Acid - Base Balance in A Picu Populationzack dahlanNessuna valutazione finora
- Excretory ReviewDocumento2 pagineExcretory Reviewapi-240662720Nessuna valutazione finora
- 1 Il-10 ElisaDocumento15 pagine1 Il-10 ElisaYousra ZeidanNessuna valutazione finora
- Voice Disorder 2011 PDFDocumento6 pagineVoice Disorder 2011 PDFfaidgustisyarifNessuna valutazione finora
- Science7 q2 Week 4 Refined FinalDocumento18 pagineScience7 q2 Week 4 Refined FinalRonalynAlonsabeBernadasNessuna valutazione finora