Potrebbero piacerti anche
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (120)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (73)
- Functional Assessment Tool For Behavior PDFDocumento2 pagineFunctional Assessment Tool For Behavior PDFads100% (1)
- Nanda NCP BasedDocumento14 pagineNanda NCP Baseddeliejoyce100% (1)
- Seismic Design of Industrial StructuresDocumento73 pagineSeismic Design of Industrial StructuresALONSO GOMEZ100% (2)
- Ocean PoemsDocumento14 pagineOcean PoemsIsabel CristinaNessuna valutazione finora
- SACS BrochureDocumento12 pagineSACS Brochurejakeer7100% (1)
- Natural Disaster Monitoring and Alert System Using IOT For Earthquake Fire and LandslidesDocumento4 pagineNatural Disaster Monitoring and Alert System Using IOT For Earthquake Fire and LandslidesInternational Journal of Innovative Science and Research TechnologyNessuna valutazione finora
- Finding Your Inner SelfDocumento5 pagineFinding Your Inner SelfdeliejoyceNessuna valutazione finora
- Finding Your Inner SelfDocumento5 pagineFinding Your Inner SelfdeliejoyceNessuna valutazione finora
- Finding Your Inner SelfDocumento5 pagineFinding Your Inner SelfdeliejoyceNessuna valutazione finora
- NSCP 1992 PDFDocumento70 pagineNSCP 1992 PDFanon_181338447100% (1)
- NCP PEDIA TonsillitisDocumento2 pagineNCP PEDIA Tonsillitisdeliejoyce100% (1)
- Earthquakes and Faults LectureDocumento41 pagineEarthquakes and Faults Lectureervynsana100% (1)
- ICU Case PresentationDocumento51 pagineICU Case Presentationdeliejoyce0% (1)
- Designer's Guide To EUROCODE 4Documento257 pagineDesigner's Guide To EUROCODE 4Stefan Fiorano0% (1)
- Pearson Edexcel International Advanced Level in Geography SCHEME OF WORK: Unit 1: Global ChallengesDocumento13 paginePearson Edexcel International Advanced Level in Geography SCHEME OF WORK: Unit 1: Global ChallengesEnriqueMinhazNessuna valutazione finora
- Lap CholeDocumento5 pagineLap CholedeliejoyceNessuna valutazione finora
- CRUSH SYNDROME Defines AsDocumento4 pagineCRUSH SYNDROME Defines AsdeliejoyceNessuna valutazione finora
- Condom For Male and FemaleDocumento3 pagineCondom For Male and FemaledeliejoyceNessuna valutazione finora
- Presentation 1Documento17 paginePresentation 1deliejoyceNessuna valutazione finora
- Anatomy and Physiology of The BrainDocumento1 paginaAnatomy and Physiology of The BraindeliejoyceNessuna valutazione finora
- Hope 1Documento2 pagineHope 1deliejoyceNessuna valutazione finora
- Anatomy and PhysiologyDocumento5 pagineAnatomy and PhysiologydeliejoyceNessuna valutazione finora
- Nursing Care PlanDocumento3 pagineNursing Care PlandeliejoyceNessuna valutazione finora
- ETO NA TALAGA Tapos Na Ang LahatDocumento32 pagineETO NA TALAGA Tapos Na Ang LahatdeliejoyceNessuna valutazione finora
- Hope 12Documento2 pagineHope 12deliejoyceNessuna valutazione finora
- Dura - : The Tough Outermost Membrane Enveloping The Brain and Spinal CordDocumento1 paginaDura - : The Tough Outermost Membrane Enveloping The Brain and Spinal CorddeliejoyceNessuna valutazione finora
- Weaning Guidelines 2007Documento4 pagineWeaning Guidelines 2007deliejoyceNessuna valutazione finora
- Mechanical Ventilation Indication: Acute Respiratory Failure?Documento1 paginaMechanical Ventilation Indication: Acute Respiratory Failure?deliejoyceNessuna valutazione finora
- Stroke and Cerebrovascular Disease GN Rs 5Documento41 pagineStroke and Cerebrovascular Disease GN Rs 5deliejoyceNessuna valutazione finora
- Weaning Guidelines 2007Documento4 pagineWeaning Guidelines 2007deliejoyceNessuna valutazione finora
- Acute Tonsillopharyngitis Exudative Case Study 2013Documento27 pagineAcute Tonsillopharyngitis Exudative Case Study 2013deliejoyceNessuna valutazione finora
- Cardiorespiratory Fitness:: 2. Muscular StrengthDocumento3 pagineCardiorespiratory Fitness:: 2. Muscular StrengthdeliejoyceNessuna valutazione finora
- Your CompanyDocumento6 pagineYour CompanydeliejoyceNessuna valutazione finora
- Thesis Manuscript 16may2017Documento108 pagineThesis Manuscript 16may2017deliejoyceNessuna valutazione finora
- Problem # 3 What Are The Factors That Contribute To The Respondent's Practices of Breastfeeding? A. Knowledge and Awareness B. Beliefs Table 8Documento6 pagineProblem # 3 What Are The Factors That Contribute To The Respondent's Practices of Breastfeeding? A. Knowledge and Awareness B. Beliefs Table 8deliejoyceNessuna valutazione finora
- What Is Complementary GoodDocumento2 pagineWhat Is Complementary GooddeliejoyceNessuna valutazione finora
- Anatomy and Physiology HeartDocumento11 pagineAnatomy and Physiology HeartKier_John_Kora_9076Nessuna valutazione finora
- Comparison of Hexagrid and Diagrid Structural System in Tall BuildingsDocumento7 pagineComparison of Hexagrid and Diagrid Structural System in Tall BuildingsFarhan DanishNessuna valutazione finora
- Lecture On Limit State Design by Manish BhutaniDocumento27 pagineLecture On Limit State Design by Manish BhutaniTarunNessuna valutazione finora
- Seismic Behavior of Squat Reinforced Concrete Shear WallsDocumento22 pagineSeismic Behavior of Squat Reinforced Concrete Shear WallstaosyeNessuna valutazione finora
- The Impact of Natural Disasters - SciencingDocumento4 pagineThe Impact of Natural Disasters - SciencingKuzo TribeNessuna valutazione finora
- Earth Science 2ND Quarter ReviewerDocumento1 paginaEarth Science 2ND Quarter ReviewerSophia Lorraine CabisonNessuna valutazione finora
- Erection All Risks Policy: Whereas The InsuredDocumento7 pagineErection All Risks Policy: Whereas The InsuredayshaNessuna valutazione finora
- Narrative Report: School Disaster Risk Reduction and Management (SDRRM)Documento8 pagineNarrative Report: School Disaster Risk Reduction and Management (SDRRM)EMELIE PUYOSNessuna valutazione finora
- Ursa Major Elementary School Collapse Prevention Findings ReportDocumento33 pagineUrsa Major Elementary School Collapse Prevention Findings ReportAlaska's News SourceNessuna valutazione finora
- Plate BoundariesDocumento20 paginePlate BoundariesMarian Christy TigueNessuna valutazione finora
- Shamsabadi Model - Closed-Form Force-Displacement Backbone Curves For Bridge AbutmentDocumento10 pagineShamsabadi Model - Closed-Form Force-Displacement Backbone Curves For Bridge AbutmentSaeedNessuna valutazione finora
- Jurnal Aceh MedikaDocumento5 pagineJurnal Aceh MedikaUmi LailatulNessuna valutazione finora
- Seismic Energy Dissipation of A Building UsingDocumento4 pagineSeismic Energy Dissipation of A Building UsingDiegoHenaoLeonNessuna valutazione finora
- Hazus-Mh MR3Documento19 pagineHazus-Mh MR3Bipul PoudelNessuna valutazione finora
- AAA - Stability - Lecture - SummaryDocumento146 pagineAAA - Stability - Lecture - SummaryIvan EstradaNessuna valutazione finora
- 02 2011 ANIDIS GavricDocumento13 pagine02 2011 ANIDIS GavricDavid MartinsNessuna valutazione finora
- M.Tech. (Full-Time) - Structural Engineering Department of Civil Engineering Curriculum & SyllabusDocumento45 pagineM.Tech. (Full-Time) - Structural Engineering Department of Civil Engineering Curriculum & SyllabusRavi MalikNessuna valutazione finora
- Newsademic Issue 057 BDocumento17 pagineNewsademic Issue 057 BsinanschNessuna valutazione finora
- Findings On The Earthquake Risk Preparedness La Paz JABADDocumento11 pagineFindings On The Earthquake Risk Preparedness La Paz JABADKetsmy DesrosiersNessuna valutazione finora
- Seismic EventsDocumento37 pagineSeismic EventsAndres Loja100% (1)
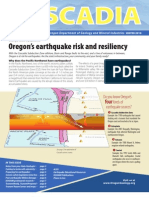
- Oregon's Earthquake Risk and Resiliency (Oregon Department of Geology and Mineral Industries)Documento12 pagineOregon's Earthquake Risk and Resiliency (Oregon Department of Geology and Mineral Industries)Statesman JournalNessuna valutazione finora
- 2010 Collaborative Middle School Tournament Round 3 TossupsDocumento8 pagine2010 Collaborative Middle School Tournament Round 3 TossupsJerry LiNessuna valutazione finora
- Computation of Base ShearDocumento77 pagineComputation of Base ShearCivil Engineering PDFNessuna valutazione finora