Potrebbero piacerti anche
- The Body in Sport - LearnerDocumento31 pagineThe Body in Sport - Learnerplumbs23Nessuna valutazione finora
- The Science of Bones 3rd Grade Textbook | Children's Biology BooksDa EverandThe Science of Bones 3rd Grade Textbook | Children's Biology BooksNessuna valutazione finora
- Skeletal SystemDocumento13 pagineSkeletal Systemariolajose5Nessuna valutazione finora
- SKELETAL SYSTEM-WPS OfficeDocumento7 pagineSKELETAL SYSTEM-WPS OfficeAlan Gandidze MotifNessuna valutazione finora
- The Skeletal SystemDocumento5 pagineThe Skeletal SystemMika SaldañaNessuna valutazione finora
- Skeletal PartsDocumento6 pagineSkeletal PartsResa MagusaraNessuna valutazione finora
- Module 2: Anatomy - The Skeleton: in This Module You Will LearnDocumento10 pagineModule 2: Anatomy - The Skeleton: in This Module You Will LearnMarkus KaltenhauserNessuna valutazione finora
- Drawing 2 M1-M2Documento20 pagineDrawing 2 M1-M2Vince VillanuevaNessuna valutazione finora
- What Is The Skeletal System?Documento21 pagineWhat Is The Skeletal System?Ezekiel A. NavarroNessuna valutazione finora
- Musculo Skeletal SystemDocumento3 pagineMusculo Skeletal SystemMARY JOY MANALANSANNessuna valutazione finora
- Systems of The BodyDocumento144 pagineSystems of The BodyTweetie Borja DapogNessuna valutazione finora
- Skeletal SystemDocumento4 pagineSkeletal Systemapi-26052253Nessuna valutazione finora
- Sketetal SystemDocumento11 pagineSketetal SystemBryan JagroopNessuna valutazione finora
- Skeletal SystemDocumento23 pagineSkeletal SystemNickmor OamlinNessuna valutazione finora
- PATHFITDocumento7 paginePATHFITkateeemadrid0Nessuna valutazione finora
- Skeletal SystemDocumento12 pagineSkeletal SystemGregg LegaspiNessuna valutazione finora
- Skeletal System Reading Comprehension Exercises - 126764Documento5 pagineSkeletal System Reading Comprehension Exercises - 126764Lucianny FilionNessuna valutazione finora
- The Human Skeletal SystemDocumento3 pagineThe Human Skeletal SystemFelix AyornuNessuna valutazione finora
- Track EventDocumento21 pagineTrack Eventbosshage2Nessuna valutazione finora
- Human Skeleton: Navigation SearchDocumento7 pagineHuman Skeleton: Navigation SearchvinaiyaNessuna valutazione finora
- Week 10 Bio 11 Skeletal SystemDocumento46 pagineWeek 10 Bio 11 Skeletal SystemDyah AnggraeniNessuna valutazione finora
- XI Unit 7 Phy. Edu. Fundamentals of Anatomy Physiology in SportsDocumento17 pagineXI Unit 7 Phy. Edu. Fundamentals of Anatomy Physiology in Sportsranike4842Nessuna valutazione finora
- Skeletal SystemDocumento7 pagineSkeletal SystemmikeNessuna valutazione finora
- Skeletal SystemDocumento19 pagineSkeletal Systemsmbdy tbhhhNessuna valutazione finora
- Class 5 - Science Chapter 3Documento18 pagineClass 5 - Science Chapter 3deviNessuna valutazione finora
- 02 SkeletalsystemDocumento18 pagine02 SkeletalsystemhorozukaNessuna valutazione finora
- Human SkeletalDocumento17 pagineHuman SkeletalMa Kristine CabyaoNessuna valutazione finora
- Diseases of The Skeletal SystemDocumento20 pagineDiseases of The Skeletal Systemlateef ramonNessuna valutazione finora
- Support and Movement SystemsDocumento3 pagineSupport and Movement SystemsJas TingNessuna valutazione finora
- 9.3 Bones Muscles and JointsDocumento5 pagine9.3 Bones Muscles and JointsDerick NKANDU KALUBANessuna valutazione finora
- Presentation AvyvsDocumento3 paginePresentation Avyvs10 Lê Viết Hiển 12.13Nessuna valutazione finora
- Bones in The Body 1. Skull: Skeletal SystemDocumento12 pagineBones in The Body 1. Skull: Skeletal SystemSolemnly SwearrNessuna valutazione finora
- AnatomyDocumento17 pagineAnatomyAb To zine doNessuna valutazione finora
- What Is The Skeletal SystemDocumento9 pagineWhat Is The Skeletal SystemTishonna DouglasNessuna valutazione finora
- AssignmentFile 18 06032024133208Documento15 pagineAssignmentFile 18 06032024133208kartikbansal232007Nessuna valutazione finora
- Pathfit ReviewerDocumento7 paginePathfit ReviewerbantayalagaNessuna valutazione finora
- Skeletal Joint: Dr. Vareishang Tangpu Assistant Professor in Zoology RIE, Mysore - 06Documento53 pagineSkeletal Joint: Dr. Vareishang Tangpu Assistant Professor in Zoology RIE, Mysore - 06Floriza de LeonNessuna valutazione finora
- Skeletal SystemDocumento7 pagineSkeletal SystemJovi Floresca AberinNessuna valutazione finora
- Skeletal SystemDocumento28 pagineSkeletal SystemAivee SumulongNessuna valutazione finora
- What Is OsteologyDocumento5 pagineWhat Is Osteology69722Nessuna valutazione finora
- Muscular and Skeletal SystemDocumento8 pagineMuscular and Skeletal SystemPrasad WasteNessuna valutazione finora
- What Is The Musculoskeletal SystemDocumento4 pagineWhat Is The Musculoskeletal SystemCarolyn TalabocNessuna valutazione finora
- Bones, Muscles, and Joints: What Are Bones and What Do They Do?Documento4 pagineBones, Muscles, and Joints: What Are Bones and What Do They Do?Rolavilla BartolomeNessuna valutazione finora
- Skeletal SystemDocumento29 pagineSkeletal SystemCrii XiaNessuna valutazione finora
- Interaction of Skeletal and Muscular SystemDocumento43 pagineInteraction of Skeletal and Muscular SystemJezebel MolinoNessuna valutazione finora
- Skeletal SystemDocumento29 pagineSkeletal SystemMB LoterteNessuna valutazione finora
- Musculoskeletal SystemDocumento62 pagineMusculoskeletal SystemAnjanette Lopez PorlucasNessuna valutazione finora
- Bones BiomechanicDocumento38 pagineBones BiomechanicTEH YU SHIAN SHARONNessuna valutazione finora
- 02 Handout 2 (4) 2Documento5 pagine02 Handout 2 (4) 2Senpai LeonNessuna valutazione finora
- Muscular system-WPS OfficeDocumento27 pagineMuscular system-WPS OfficeNiño Rey LavadorNessuna valutazione finora
- Lesson 3: Musculoskeletal, Circulatory and Respiratory System TermsDocumento6 pagineLesson 3: Musculoskeletal, Circulatory and Respiratory System TermsClaudine NaturalNessuna valutazione finora
- Module 3 PE FinalDocumento14 pagineModule 3 PE FinalStephanie De Guzman LimNessuna valutazione finora
- Skeletal System - mp4 - Google DriveDocumento7 pagineSkeletal System - mp4 - Google Drivefaresalesa2005Nessuna valutazione finora
- Anatomy 3 (Bone) Unilus ShortDocumento32 pagineAnatomy 3 (Bone) Unilus ShortMotasifa FxNessuna valutazione finora
- Textos I Medicina Level I 2020Documento18 pagineTextos I Medicina Level I 2020Valeria DonzelliNessuna valutazione finora
- The Skeletal SystemDocumento30 pagineThe Skeletal SystemFAtma HAnysNessuna valutazione finora
- Case Study in GoutDocumento17 pagineCase Study in GoutPaulette Olisco0% (1)
- T1 Condicion Fisica 4º EsoDocumento6 pagineT1 Condicion Fisica 4º EsoMartín Benítez del HoyoNessuna valutazione finora
- The Fascinating World of The Skeletal SystemDocumento13 pagineThe Fascinating World of The Skeletal SystemREBECCA MITRANessuna valutazione finora
- Main SIF&HIPO @202211Documento5 pagineMain SIF&HIPO @202211NguyenLinh27Nessuna valutazione finora
- 3M Cable Termination Installation InstructionDocumento8 pagine3M Cable Termination Installation Instructionnixsol75Nessuna valutazione finora
- Nasal TraumaDocumento5 pagineNasal TraumaRae Marie AquinoNessuna valutazione finora
- Dynamic Q Angle Is Increased in Patients With Chronic PatellofemoralDocumento8 pagineDynamic Q Angle Is Increased in Patients With Chronic PatellofemoralDavids MarinNessuna valutazione finora
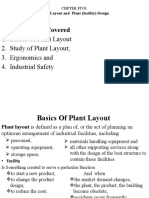
- Chapter 5Documento20 pagineChapter 5Berihu GirmayNessuna valutazione finora
- HPSU RexorthDocumento409 pagineHPSU Rexorthf984jykhd6Nessuna valutazione finora
- Askep Luka BakarDocumento59 pagineAskep Luka BakarRahmiwulandariNessuna valutazione finora
- Dawson 2002 - Upper-Extremity Problems Caused by Playing InstrumentsDocumento6 pagineDawson 2002 - Upper-Extremity Problems Caused by Playing InstrumentsDiana MatiasNessuna valutazione finora
- Health and Safety For Greenhouses and NurseriesDocumento128 pagineHealth and Safety For Greenhouses and NurseriesEugenNessuna valutazione finora
- American Heart Association PPT - AIHA Webinar - FinalDocumento49 pagineAmerican Heart Association PPT - AIHA Webinar - FinalVina WineNessuna valutazione finora
- Confined Space Entry Rescue Plan GENERIC PDFDocumento10 pagineConfined Space Entry Rescue Plan GENERIC PDFaby131Nessuna valutazione finora
- OrifDocumento2 pagineOrifGene Edward D. ReyesNessuna valutazione finora
- Unit 8 Med Surg Study Guide NursingDocumento5 pagineUnit 8 Med Surg Study Guide Nursingatl_nurse_student100% (7)
- Psoas StretchesDocumento9 paginePsoas Stretcheswalterego58Nessuna valutazione finora
- Qashqai j10Documento297 pagineQashqai j10David Gonzalez PerezNessuna valutazione finora
- 6th Body Systems Packet WORKSHEETSDocumento39 pagine6th Body Systems Packet WORKSHEETSElizabeth Alvarez100% (1)
- Anatomical PositionDocumento7 pagineAnatomical PositionVanroNessuna valutazione finora
- OMM OMT Cheat SheetDocumento1 paginaOMM OMT Cheat SheetNabeel ShahzadNessuna valutazione finora
- Cover 1: Nick Saban: Middle of The Field Safety Coverage Principles (Part III - Cover 1)Documento12 pagineCover 1: Nick Saban: Middle of The Field Safety Coverage Principles (Part III - Cover 1)mdfishbein100% (2)
- Osha Report From Seaworld InvestigationDocumento47 pagineOsha Report From Seaworld InvestigationSusan MaeNessuna valutazione finora
- Frenectomy PDFDocumento6 pagineFrenectomy PDFzinniaNessuna valutazione finora
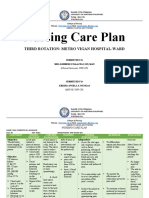
- Nursing Care Plan: Third Rotation: Metro Vigan Hospital-WardDocumento5 pagineNursing Care Plan: Third Rotation: Metro Vigan Hospital-WardKrizha Angela NicolasNessuna valutazione finora
- Foot Orthotics Claiming Checklist BLUE CROSSDocumento1 paginaFoot Orthotics Claiming Checklist BLUE CROSSBradley ChristmasNessuna valutazione finora
- OrthopaedicDocumento74 pagineOrthopaedicPrima Krishna Dharmawan100% (4)
- PT 2.2 2014 Student DossierDocumento89 paginePT 2.2 2014 Student DossierArturo Ruiz LeónNessuna valutazione finora
- 2017 Spine CPT Code Changes: Kim Pollock, RN, MBA, CPC, CMDPDocumento4 pagine2017 Spine CPT Code Changes: Kim Pollock, RN, MBA, CPC, CMDPZakariaAwaludinNessuna valutazione finora
- NUR11O1 Integrated Human Anatomy and Physiology Department of Biology Institute of Arts and Sciences Far Eastern UniversityDocumento6 pagineNUR11O1 Integrated Human Anatomy and Physiology Department of Biology Institute of Arts and Sciences Far Eastern UniversityPrancheska Abigayle Peneyra SantiagoNessuna valutazione finora
- Chapter 12: The Back: Vertebral ColumnDocumento7 pagineChapter 12: The Back: Vertebral ColumnJyrra NeriNessuna valutazione finora
- Expressing Pain Relief PleasureDocumento14 pagineExpressing Pain Relief PleasureTitik Winarti100% (3)
- V 4 I 5 CognitiveDocumento3 pagineV 4 I 5 CognitiveSusana Ruiz Losada BeainNessuna valutazione finora
- Horse Care 101: How to Take Care of a Horse for BeginnersDa EverandHorse Care 101: How to Take Care of a Horse for BeginnersValutazione: 4 su 5 stelle4/5 (5)
- Lead with Your Heart: Lessons from a Life with HorsesDa EverandLead with Your Heart: Lessons from a Life with HorsesValutazione: 4 su 5 stelle4/5 (8)
- Project Solomon: The True Story of a Lonely Horse Who Found a Home--and Became a HeroDa EverandProject Solomon: The True Story of a Lonely Horse Who Found a Home--and Became a HeroValutazione: 5 su 5 stelle5/5 (9)
- The Power of the Herd: A Nonpredatory Approach to Social Intelligence, Leadership, and InnovationDa EverandThe Power of the Herd: A Nonpredatory Approach to Social Intelligence, Leadership, and InnovationNessuna valutazione finora
- Paddock Paradise: A Guide to Natural Horse BoardingDa EverandPaddock Paradise: A Guide to Natural Horse BoardingNessuna valutazione finora
- The Winning Horseplayer: An Advanced Approach to Thoroughbred Handicapping and BettingDa EverandThe Winning Horseplayer: An Advanced Approach to Thoroughbred Handicapping and BettingNessuna valutazione finora
- The Faraway Horses: The Adventures and Wisdom of America's Most Renowned HorsemenDa EverandThe Faraway Horses: The Adventures and Wisdom of America's Most Renowned HorsemenValutazione: 4.5 su 5 stelle4.5/5 (49)
- The Equine Listenology Guide - Essential Horsemanship, Horse Body Language & Behaviour, Groundwork, In-hand Exercises & Riding Lessons to Develop Softness, Connection & Collection.Da EverandThe Equine Listenology Guide - Essential Horsemanship, Horse Body Language & Behaviour, Groundwork, In-hand Exercises & Riding Lessons to Develop Softness, Connection & Collection.Valutazione: 5 su 5 stelle5/5 (1)
- Speak Your Horse's Language:: Communicating with the Driving HorseDa EverandSpeak Your Horse's Language:: Communicating with the Driving HorseNessuna valutazione finora
- How Long Can a Fly Fly?: 175 Answers to Possible and Impossible Questions about AnimalsDa EverandHow Long Can a Fly Fly?: 175 Answers to Possible and Impossible Questions about AnimalsNessuna valutazione finora
- Black Beauty (Illustrated): Classic of World LiteratureDa EverandBlack Beauty (Illustrated): Classic of World LiteratureValutazione: 4 su 5 stelle4/5 (2429)
- Wild Horses of the Summer Sun: A Memoir of IcelandDa EverandWild Horses of the Summer Sun: A Memoir of IcelandValutazione: 3.5 su 5 stelle3.5/5 (4)
- Joey: How a Blind Rescue Horse Helped Others Learn to SeeDa EverandJoey: How a Blind Rescue Horse Helped Others Learn to SeeValutazione: 5 su 5 stelle5/5 (23)
- Second-Chance Horses: True Stories of the Horses We Rescue and the Horses Who Rescue UsDa EverandSecond-Chance Horses: True Stories of the Horses We Rescue and the Horses Who Rescue UsNessuna valutazione finora
- Stable Relation: A Memoir of One Woman's Spirited Journey Home, by Way of the BarnDa EverandStable Relation: A Memoir of One Woman's Spirited Journey Home, by Way of the BarnValutazione: 5 su 5 stelle5/5 (4)
- The USPC Guide to Longeing and Ground TrainingDa EverandThe USPC Guide to Longeing and Ground TrainingValutazione: 4.5 su 5 stelle4.5/5 (3)
- The Tao Of Horses: Exploring How Horses Guide Us on Our Spiritual PathDa EverandThe Tao Of Horses: Exploring How Horses Guide Us on Our Spiritual PathValutazione: 5 su 5 stelle5/5 (1)
- The Everything Horse Care Book: A Complete Guide to the Well-being of Your HorseDa EverandThe Everything Horse Care Book: A Complete Guide to the Well-being of Your HorseNessuna valutazione finora
- Traditional Blacksmithing: The Fine Art of Horseshoeing and Wagon MakingDa EverandTraditional Blacksmithing: The Fine Art of Horseshoeing and Wagon MakingNessuna valutazione finora
- 101 Fun Facts and Trivia About Horses: All You Need To Know If You Are Crazy About HorsesDa Everand101 Fun Facts and Trivia About Horses: All You Need To Know If You Are Crazy About HorsesNessuna valutazione finora
- The Everything Horse Book: Buying, riding, and caring for your equine companionDa EverandThe Everything Horse Book: Buying, riding, and caring for your equine companionValutazione: 2 su 5 stelle2/5 (1)